Download presentation
Presentation is loading. Please wait.

1
Michael Haines, MPH, RRT-NPS, AE-C
Asthma Michael Haines, MPH, RRT-NPS, AE-C

3
What is Asthma Asthma is a disease of inflammation and bronchial smooth muscle constriction that causes the trapping of gas and wheezing Asthma affects children more than adults due to anatomical diameter of the airway. You are never cured of asthma, you do however grow and the affects of asthma often lessen as you grow Asthma is completely treatable and manageable

4
What is Asthma Continued…
Asthma is one of the most chronic serious diseases in children and adolescents, affecting nearly nine million children under the age of 18. Fifty to 80% of children with asthma develop the symptoms of asthma before the age of 5. Asthma occurs when a stimulus triggers a reaction in the lung mucosa and nervous system causing muscle constriction This stimulus can occur as a result of a allergen or an irritant such as smoke

5
Who is at risk to develop asthma
Who is at risk to develop asthma? Asthma is commonly divided into two types: allergic (extrinsic) asthma and non-allergic (intrinsic) asthma Children whose immune systems are not fully developed are most at risk for developing the disease. However, there are no clear markers to predict who will develop asthma and who won't. Studies have shown that factors associated with the onset of asthma symptoms in children include: Infants and young children who wheeze with viral upper respiratory infections. Allergies. The relationship between asthma and allergies is very strong. A family history of asthma and/or allergy Prenatal exposure to tobacco smoke and allergens
 asthma and non-allergic (intrinsic) asthma. Children whose immune systems are not fully developed are most at risk for developing the disease. However, there are no clear markers to predict who will develop asthma and who won t. Studies have shown that factors associated with the onset of asthma symptoms in children include: Infants and young children who wheeze with viral upper respiratory infections. Allergies. The relationship between asthma and allergies is very strong. A family history of asthma and/or allergy. Prenatal exposure to tobacco smoke and allergens.")
6
The most common form of asthma among children is allergic asthma
The most common form of asthma among children is allergic asthma. In this form, otherwise harmless allergens, such as dust mites, cat and dog dander or other environmental allergens, can trigger an asthma attack. In addition to allergy symptoms brought on by exposure to these allergens-watery eyes, sneezing and itching-asthmatics can experience severe airway constriction. (Dust mites live primarily in Humid Environments, they are microscopic)
")
7
Allergens Important treatment= stay away from your allergens!
If you don’t know what you are allergic to get a allergy test

8
The Role of Heredity in Asthma
Heredity. To some extent, asthma seems to run in families. People whose brothers, sisters or parents have asthma are more likely to develop the illness themselves. Atopy. A person is said to have atopy (or to be atopic) when he or she is prone to have allergies. For reasons that are not fully known, some people seem to inherit a tendency to develop allergies. This is not to say that a parent can pass on a specific type of allergy to a child. In other words, it doesn't mean that if your mother is allergic to bananas, you will be too. But you may develop allergies to something else, like pollen or mold. In addition, several factors must be present for asthma symptoms to develop: Specific genes must be acquired from parents. Exposure to allergens or triggers to which you have a genetically programmed response. Environmental factors such as quality of air, exposure to irritants, behavioral factors such as smoking, etc.
 when he or she is prone to have allergies. For reasons that are not fully known, some people seem to inherit a tendency to develop allergies. This is not to say that a parent can pass on a specific type of allergy to a child. In other words, it doesn t mean that if your mother is allergic to bananas, you will be too. But you may develop allergies to something else, like pollen or mold. In addition, several factors must be present for asthma symptoms to develop: Specific genes must be acquired from parents. Exposure to allergens or triggers to which you have a genetically programmed response. Environmental factors such as quality of air, exposure to irritants, behavioral factors such as smoking, etc.")
9
Allergy Test Skin test- numerous known substances are placed on the skin, reactions are noted and allergens are then determined

10
Allergy Test Besides the skin allergy test they also due blood tests
The RAST test measures the levels of the allergy antibody IgE that is produced when your blood is mixed with a series of allergens in a laboratory.

12
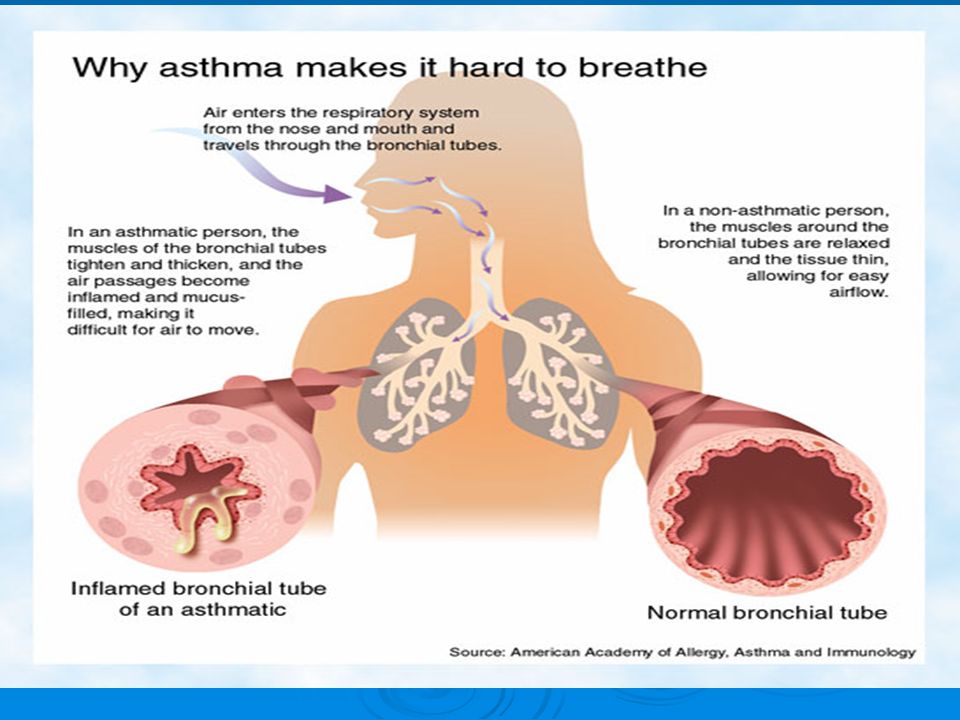
What Happens During an Asthma Episode?
During normal breathing, the airways to the lungs are fully open, allowing air to move in and out freely. But people with asthma have inflamed, super-sensitive airways. Their triggers cause the following airway changes, which in turn cause asthma symptoms: The lining of the airways swell and become more inflamed Mucus clogs the airways Muscles tighten around the airways (bronchospasm) These changes narrow the airways until breathing becomes difficult and stressful, like trying to breathe through a straw stuffed with cotton.
 These changes narrow the airways until breathing becomes difficult and stressful, like trying to breathe through a straw stuffed with cotton.")
13
The lung is lined with a mucosa layer which is basically a layer of cells responsible for lubrication and debris movement out of the lung During an allergic reaction and subsequent asthma attack, this mucosa releases histamines from mast cells, mucus from goblet cells and inflammatory cells; all of which increase the thickness and narrowing of the airways. At the same time the muscle around the lung tightens

14
Following an Asthma attack; the patient will have congestion and increased sputum production for several days

15
Causes Substances that cause allergies (allergens) such as dust mites, pollens, molds, pet dander, and even cockroach droppings. In many people with asthma, the same substances that cause allergy symptoms can also trigger an asthma episode. These allergens may be things that you inhale, such as pollen or dust, or things that you eat, such as shellfish. It is best to avoid or limit your exposure to known allergens in order to prevent asthma symptoms. Irritants in the air, including smoke from cigarettes, wood fires, or charcoal grills. Also, strong fumes or odors like household sprays, paint, gasoline, perfumes, and scented soaps. Although people are not actually allergic to these particles, they can aggravate inflamed, sensitive airways. Today most people are aware that smoking can lead to cancer and heart disease. Smoking is also a risk factor for asthma in children, and a common trigger of asthma symptoms for all ages
 such as dust mites, pollens, molds, pet dander, and even cockroach droppings. In many people with asthma, the same substances that cause allergy symptoms can also trigger an asthma episode. These allergens may be things that you inhale, such as pollen or dust, or things that you eat, such as shellfish. It is best to avoid or limit your exposure to known allergens in order to prevent asthma symptoms. Irritants in the air, including smoke from cigarettes, wood fires, or charcoal grills. Also, strong fumes or odors like household sprays, paint, gasoline, perfumes, and scented soaps. Although people are not actually allergic to these particles, they can aggravate inflamed, sensitive airways. Today most people are aware that smoking can lead to cancer and heart disease. Smoking is also a risk factor for asthma in children, and a common trigger of asthma symptoms for all ages.")
16
Causes Respiratory infections such as colds, flu, sore throats, and sinus infections. These are the number one asthma trigger in children GERD: Gastric espohgeal reflux disease, stomach acid can be aspirated and inflam the airway Exercise and other activities that make you breathe harder. Exercise—especially in cold air—is a frequent asthma trigger. A form of asthma called exercise-induced asthma is triggered by physical activity. Symptoms of this kind of asthma may not appear until after several minutes of sustained exercise. (When symptoms appear sooner than this, it usually means that the person needs to adjust his or her treatment.) The kind of physical activities that can bring on asthma symptoms include not only exercise, but also laughing, crying, holding one's breath, and hyperventilating (rapid, shallow breathing). The symptoms of exercise-induced asthma usually go away within a few hours
 The kind of physical activities that can bring on asthma symptoms include not only exercise, but also laughing, crying, holding one s breath, and hyperventilating (rapid, shallow breathing). The symptoms of exercise-induced asthma usually go away within a few hours.")
17
More Causes… Weather such as dry wind, cold air, or sudden changes in weather can sometimes bring on an asthma episode. Expressing strong emotions like anger, fear or excitement. When you experience strong emotions, your breathing changes -- even if you don’t have asthma. When a person with asthma laughs, yells, or cries hard, natural airway changes may cause wheezing or other asthma symptoms. Some medications like aspirin can also be related to episodes in adults who are sensitive to aspirin. Irritants in the environment can also bring on an asthma episode. These irritants may include paint fumes, smog, aerosol sprays and even perfume.

18
Why Does My Asthma Act Up at Night?
For reasons we don't fully understand, uncontrolled asthma -- with its underlying inflammation -- often acts up at night. It probably has to do with natural body rhythms and changes in your body’s hormones, as well as the fact that some symptoms appear hours after you come in contact with a trigger. Also during sleep you release less norepinephrine (adrenaline) which acts as your bodies natural bronchodilator
 which acts as your bodies natural bronchodilator.")
19
Symptoms

20
Symptoms Coughing. Coughing from asthma is often worse at night or early in the morning, making it hard to sleep. Wheezing. Wheezing is a whistling or squeaky sound when you breathe. Chest tightness. This can feel like something is squeezing or sitting on your chest. Shortness of breath. Some people say they can't catch their breath, or they feel breathless or out of breath. You may feel like you can't get enough air in or out of your lungs. Tachypnea and tachycardia Desaturation *In children the only symptom may be a persistent cough, that occurs more the morning

21
Status Asthmaticus As severe asthma attack not responsive to bronchodilators Typically requires intubation and mechanical ventilation due to respiratory failure Typically, patients present a few days after the onset of a viral respiratory illness, following exposure to a potent allergen or irritant, or after exercise in a cold environment. Frequently, patients have underused or have been underprescribed anti-inflammatory therapy. Illicit drug use may play a role in poor adherence to anti-inflammatory therapy. Patients report chest tightness, rapidly progressive shortness of breath, dry cough, and wheezing and may have increased their beta-agonist intake (either inhaled or nebulized) to as often as every few minutes.
 to as often as every few minutes.")
22
Vitals signs and Lab tests used to diagnose:
Periods of coughing, wheezing, shortness of breath, or chest tightness that come on suddenly or occur often or seem to happen during certain times of year or season Colds that seem to "go to the chest" or take more than 10 days to get over Medicines you may have used to help your breathing Your family history of asthma and allergies What things seem to cause asthma symptoms or make them worse.

23
Early and Late Asthmatic Response
Late response is usually more severe and longer lasting.

24
Spirometry The test measures how much air and how fast you can blow air out of your lungs after taking a deep breath. The results will be lower than normal if your airways are inflamed and narrowed, as in asthma, or if the muscles around your airways have tightened up. Sometimes bronchial provocation is used to trigger an attack and then bronchodilators are given to test for reversibility (Asthma is the only reversible COPD and is considered very treatable). A substance such as methacholine, which causes narrowing of the airways in asthma, is inhaled. The effect is measured by spirometry. Children under age 5 usually cannot use a spirometer successfully. If spirometry cannot be used, the doctor may decide to try medication for a while to see if the child's symptoms get better.
. A substance such as methacholine, which causes narrowing of the airways in asthma, is inhaled. The effect is measured by spirometry. Children under age 5 usually cannot use a spirometer successfully. If spirometry cannot be used, the doctor may decide to try medication for a while to see if the child s symptoms get better.")
25
Spirometry

26
Diagnosis Diagnosis of Asthma is made with clinical symptoms and assessment; allergy awareness; PFT’s that show reverability of >10% post bronchodilator and the ruling out of other possible problems. To rule out asthma the doctor would order: A chest X-ray (asthmatics usually have normal CXR; use to find foreign bodies) Tests to see if you have gastroesophageal reflux disease (GERD) EKG: Rule out cardiac problems that may lead to SOB and cardiac wheezing ABG not necessarily useful
 Tests to see if you have gastroesophageal reflux disease (GERD) EKG: Rule out cardiac problems that may lead to SOB and cardiac wheezing. ABG not necessarily useful.")
27
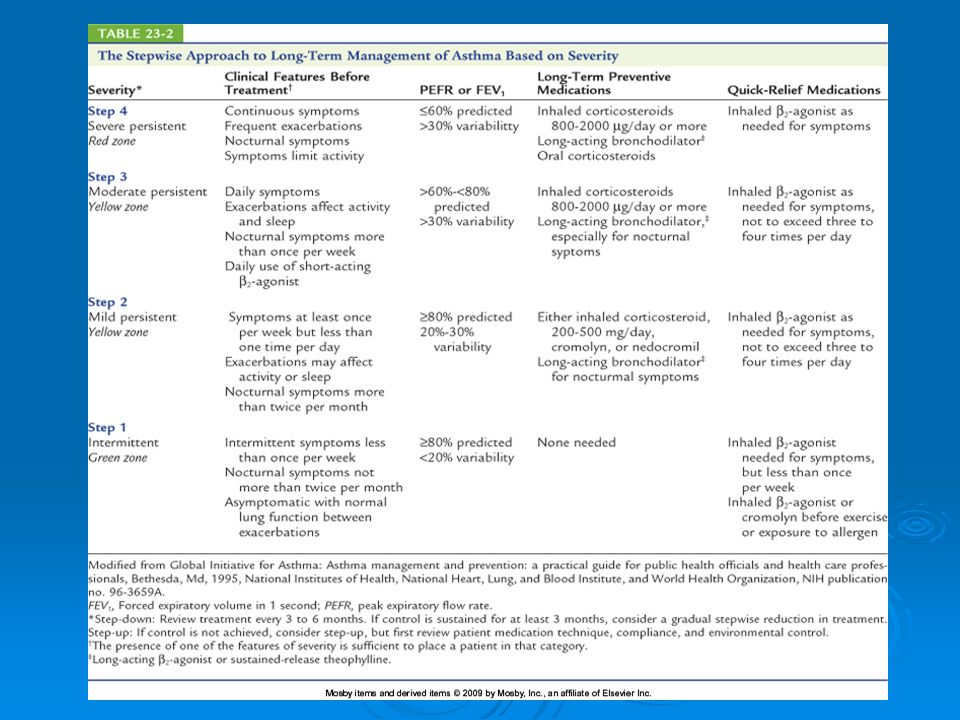
Once Diagnosed… Based on symptoms, the four levels of asthma severity classification are: Mild Intermittent (comes and goes)--when your asthma is not well controlled, you have asthma symptoms twice a week or less, and you are bothered by symptoms at night twice a month or less. Mild persistent asthma--when your asthma is not well controlled, you have asthma symptoms more than twice a week, but no more than once in a single day. You are bothered by symptoms at night more than twice a month. You may have asthma attacks that affect your activity. Moderate persistent asthma--when your asthma is not well controlled, you have asthma symptoms every day, and you are bothered by nighttime symptoms more than once a week. Asthma attacks may affect your activity. Severe persistent asthma--when your asthma is not well controlled, you have symptoms throughout the day on most days, and you are bothered by nighttime symptoms often. In severe asthma, your physical activity is likely to be limited.
--when your asthma is not well controlled, you have asthma symptoms twice a week or less, and you are bothered by symptoms at night twice a month or less. Mild persistent asthma--when your asthma is not well controlled, you have asthma symptoms more than twice a week, but no more than once in a single day. You are bothered by symptoms at night more than twice a month. You may have asthma attacks that affect your activity. Moderate persistent asthma--when your asthma is not well controlled, you have asthma symptoms every day, and you are bothered by nighttime symptoms more than once a week. Asthma attacks may affect your activity. Severe persistent asthma--when your asthma is not well controlled, you have symptoms throughout the day on most days, and you are bothered by nighttime symptoms often. In severe asthma, your physical activity is likely to be limited.")
28
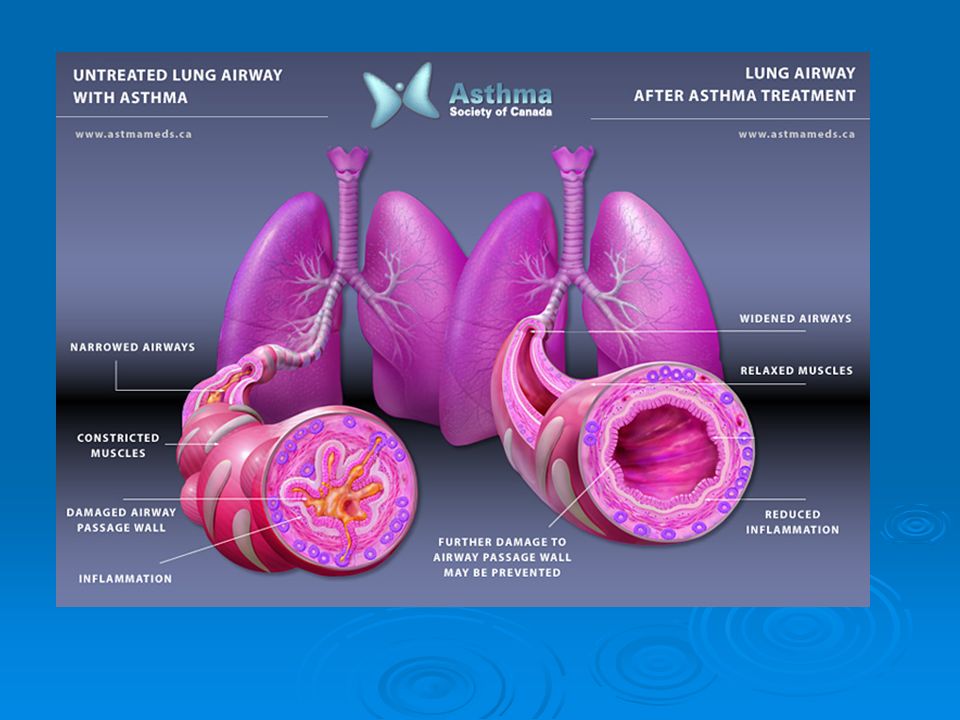
Treatment Treatment and Management-
Avoiding things that bring on your asthma symptoms or make symptoms worse. Doing so can reduce the amount of medicine you need to control your asthma. Allergy medicine and allergy shots in some cases may help your asthma. Using asthma medicines. Medications for asthma. There are two main types of medicines for asthma: 1. Quick Relief medicines give rapid, short-term treatment and are taken when you have worsening asthma symptoms that can lead to asthma episodes or attacks. You will feel the effects of these medicines within minutes. 2. Long-term Control medicines are taken every day, usually over long periods of time, to control chronic symptoms and to prevent asthma episodes or attacks. You will feel the full effects of these medicines after taking them for a few weeks. People with persistent asthma need long-term control medicines.

29
Treatment Cont… Quick Acting Drugs are called Beta 2 Adrenergic Bronchodilators. They include such drugs as Albuterol and Xopenex They react within minutes and generally last between 4-8 hours MDI or Nebulizer

30
Treatments Cont… Fast Acting Bronchodilators work to quickly relax bronchial smooth muscle. Long Acting Drugs work to maintain open lungs but are not to be given during an acute attack. Steroids are long acting drugs; common ones include Advair, Azmacort and Pulmicort Advair Azmacort

31
Treatments Continued…
Other treatments include drugs that prevent mast cells from releasing histamines; such as Singular and other allergen targeted drugs (given before attack occurs) Avoiding Allergens Mast Cell inhibitors such as Intal or Foradil Allergy Shots given annually
 Avoiding Allergens. Mast Cell inhibitors such as Intal or Foradil. Allergy Shots given annually.")
33
Pharmacotherapy Corticosteroids
Most effective mediation in treatment of asthma Reduces symptoms and mortality Use of inhaled steroids for long-term treatment preferred Use spacer and rinse mouth to eliminate or minimize side effects Long-term use of oral steroids should be restricted to patients with asthma refractory to other treatment. Short-term oral steroid use during exacerbation reduces severity, duration, and mortality. Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 33

34
Pharmacotherapy (cont.)
Cromolyn (NSAID) Protective against allergens, cold air, exercise Administered prophylactically, CANNOT be used during an acute asthma attack Of limited use in adults Drug of choice for atopic children with asthma Nedocromil (NSAID) Similar to cromolyn, it is 4–10 times more potent in preventing acute allergic bronchospasm. NSAID - Nonsteroidal antiinflammatory drug Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 34
 Protective against allergens, cold air, exercise. Administered prophylactically, CANNOT be used during an acute asthma attack. Of limited use in adults. Drug of choice for atopic children with asthma. Nedocromil (NSAID) Similar to cromolyn, it is 4–10 times more potent in preventing acute allergic bronchospasm. NSAID - Nonsteroidal antiinflammatory drug. Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 34.")
35
Pharmacotherapy (cont.)
Leukotriene inhibitors Leukotrienes mediate inflammation and bronchospasm. Modestly effective to control mild to moderate asthma Inhaled steroids remain the antiinflammatory drug of choice for the treatment of asthma. Methyxanthines (use is controversial) Oral or IV use if admitted for acute asthma attack NSAIDs have not been found to be more effective then steroids Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 35
 Oral or IV use if admitted for acute asthma attack. NSAIDs have not been found to be more effective then steroids. Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 35.")
36
Pharmacotherapy (cont.)
2-Adrenergic agonists Most rapid and effective bronchodilator Drug of choice for exercise-induced asthma and emergency relief of bronchospasm Should be used PRN Improves symptoms not underlying inflammation Regular use may worsen asthma control and increase risk of death. Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 36

37
Pharmacotherapy (cont.)
Anticholinergics Can be used as adjunct to first-line bronchodilators if there is an inadequate response Has an additive affect to 2-agonists Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc.

38
Asthma and Environmental Control
Recognized relationship between asthma and allergy 75–85% asthma patients react to inhaled allergens Environmental control is aimed at reducing exposure to allergens. Avoid outdoor allergens by remaining inside, windows closed, AC on Indoor allergens are combated by Air purifiers and no pets Dust mites: airtight covers on bed and pillow, no carpets in bedroom, chemical agents to kill mites Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 38

39
Special Considerations in Asthma Management (cont.)
Nocturnal asthma Present in two-thirds of poorly controlled asthmatics May be due to diurnal decrease in airway tone or gastric reflux Treatment should include: Steroid treatment targeted to relieve night symptoms Sustained release theophylline New long-acting 2-agonists Antacids for reflux Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 39

40
Special Considerations in Asthma Management (cont.)
Aspirin sensitivity 5% of adult asthmatics will have severe, life-threatening asthma attacks after taking NSAIDs. All asthmatics should avoid; suggest Tylenol use. Asthma during pregnancy A third of asthmatics have worse control at this time. Much higher fetal risk associated with uncontrolled asthma than that of asthma medications Theophyllines, 2-agonists, and steroids can be used without significant risk of fetal abnormalities. NSAIDs – nonsteroidal antiinflammatory drugs such as aspirin Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 40

41
Special Considerations in Asthma Management (cont.)
Sinusitis may cause asthma exacerbation. CT of sinuses will diagnosis problem. Treat: 2–3 weeks antibiotics, nasal decongestants, and nasal inhaled steroids Surgery Asthmatics at higher risk for respiratory complications Arrest during induction Hypoxemia with/without hypercarbia Impaired cough, atelectasis, pneumonia Optimize lung function preoperatively. Use steroids during procedure. Mosby items and derived items © 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 41

42
Using a Peak Flow A Peak Flow device is a assessment tool used to measure the effectiveness of fast acting bronchodilators. Given during the attack, before and after treatments It is a handheld device that the patient exhales forcibly on; as the airway opens and improves, the value increases

43
Peak Flow Continued…

44
Conclusion Asthma is a disease of inflammation and bronchial muscle constriction Caused by sensitive lungs that swell when introduced to an allergen or irritant Symptoms include cough, wheezing, chest congestion and tightness and SOB Diagnose with PFT, symptoms and allergy test Treat with Bronchodilators, Steroids, Allergen Medications and avoidance of allergies.

Similar presentations











 Asthma.>")




 illness in which the airways become blocked or narrowed>")


