Download presentation
Presentation is loading. Please wait.

1
IN THE NAME OF GOD

2
Evaluation and Management of the Patient with a Neck Mass
Dr.mirvakili Shahid sadoghi university

3
definition The general definition of a neck mass is any abnormal enlargement, swelling, or growth from the level of the base of skull to the clavicles.

4
Anatomy Prominent landmarks Hyoid bone Thyroid cartilage (men)
Cricoid cartilage (women) Trachea Sternocleidomastoid muscle
 Trachea. Sternocleidomastoid muscle.")
5
Anatomy Triangles of the neck Anterior
Anterior border of the SCM, midline, lower border of the mandible Subdivisions: inferior carotid, superior carotid, submandibular, submental Posterior Posterior border of SCM, clavicle, anterior border of trapezius Subdivisions: subclavian, occipital

6
General Considerations
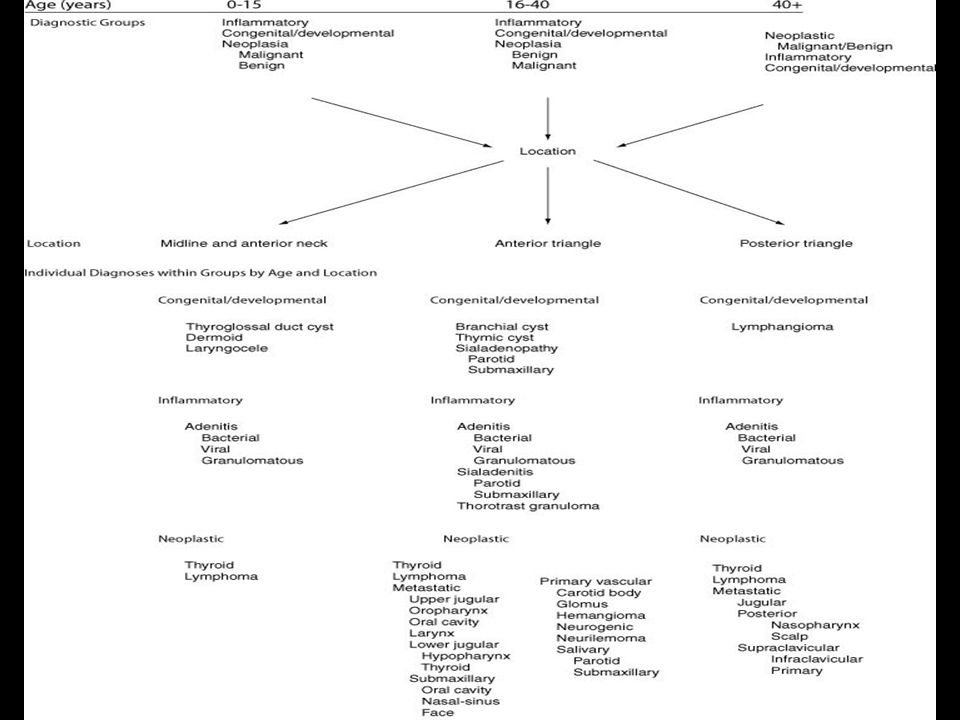
Patient age Pediatric (0 – 15 years): 90% benign Young adult (16 – 40 years): similar to pediatric Late adult (>40 years): “rule of 80s” Location Congenital masses: consistent in location Metastatic masses: key to primary lesion
: 90% benign. Young adult (16 – 40 years): similar to pediatric. Late adult (>40 years): rule of 80s Location. Congenital masses: consistent in location. Metastatic masses: key to primary lesion.")
7
General Considerations
Location of mass Congenital and developmental consistent Metastatic masses - help identify possible primary Treat each case individually *

9
Diagnostic Steps History Careful and complete
Developmental time course Associated symptoms (dysphagia, otalgia, hoarseness) Personal habits (smoking, alcohol) Prior trauma, irradiation or surgery
 Personal habits (smoking, alcohol) Prior trauma, irradiation or surgery.")
10
Diagnostic Steps Physical Examination Complete head and neck exam
Visualize all mucosal surfaces (direct, indirect) Palpate oral and pharyngeal surfaces Emphasize location, mobility and consistency of neck mass (vascular, salivary, nodal, inflammatory, congenital, neoplastic)
 Palpate oral and pharyngeal surfaces. Emphasize location, mobility and consistency of neck mass (vascular, salivary, nodal, inflammatory, congenital, neoplastic)")
11
Empirical Antibiotics
Inflammatory mass suspected Two week trial of antibiotics Follow-up for further investigation

12
Diagnostic Tests Fine needle aspiration biopsy (FNAB)
Computed tomography (CT) Magnetic resonance imaging (MRI) Ultrasonography Radionucleotide scanning PET scan
 Magnetic resonance imaging (MRI) Ultrasonography. Radionucleotide scanning. PET scan.")
13
Diagnostic Studies Fine needle aspiration biopsy (FNAB)
Standard of care Indications Not obvious abscess Persists following antibiotics No contraindications (vascular?) Fine gauge needle ( ) Skilled pathologist critical
 Fine gauge needle ( ) Skilled pathologist critical.")
14
Diagnostic Studies FNAB continued Needle track seeding not a concern
Bleeding complications reduced Can be performed in children Separates neoplasm from inflammatory & carcinoma from lymphoma Minimum of four separate needle passes

15
Diagnostic Studies Computed Tomography (CT) Very helpful tool
Solid versus cystic With contrast delineates vascularity Metastatic masses Unknown primary and staging purposes Lucent changes, >1.5 cm, loss of sharpness Avoid contrast in thyroid masses

16
Diagnostic Studies Magnetic Resonance Imaging (MRI)
Similar information as CT Better for upper neck and skull base Infusion may substitute for arteriography

17
Diagnostic Studies Ultrasonography Less important with advent of FNAB
Useful for solid versus cystic (congenital cyst vs. lymph node/glandular tumor) Noninvasive (pediatric)
 Noninvasive (pediatric)")
18
Diagnostic Studies Radionucleotide Scanning
Intra-glandular versus extra-glandular Functionality Salivary and thyroid masses FNAB preferred for thyroid nodules Solitary thyroid nodule Multinodular goiter with new increasing nodule Hashimoto’s with new nodule

19
Radionucleotide Scanning

20
PET scan Pet scan indicates the functional activity of a mass
A more radio-intense mass has greater metabolic activity and is usually neoplastic High false positive rate(warthin,s tumor)
")
22
Nodal Mass Workup in the Adult
Any solid asymmetric mass must be considered metastatic until proven otherwise Presenting symptom in 12% of cancers 80% are SCCa History of smoking and alcohol worrisome Suspicious symptoms and signs Ipsilateral otalgia with normal otoscopy Unilateral serous otitis media (nasopharynx)
")
23
Nodal Mass Workup in the Adult
Indications for panendoscopy Positive FNAB (staging, search for primary, synchronous primaries - 10 to 20%) Equivocal or negative FNAB in high risk Unknown primary Biopsy suspicious observed areas or suspicious abnormalities on CT/MRI None - biopsy nasopharynx, tonsil (ipsilateral tonsillectomy for jugulodigastric nodes), base of tongue, and pyriform sinuses
 Equivocal or negative FNAB in high risk. Unknown primary. Biopsy suspicious observed areas or suspicious abnormalities on CT/MRI. None - biopsy nasopharynx, tonsil (ipsilateral tonsillectomy for jugulodigastric nodes), base of tongue, and pyriform sinuses.")
24
Nodal Mass & Unknown Primary
Open excisional biopsy Repeated exam and workup fail to reveal 10 with an equivocal or negative FNAB 5% of the time Prepare for complete neck dissection Frozen section results Inflammatory or granulomatous: culture tissue Adenocarcinoma or lymphoma: close wound

25
Common Primary Tumors Thyroid Masses Lymphoma Salivary Tumors Lipoma
Carotid Body and Glomus Tumors Neurogenic Tumors

26
Thyroid Masses A leading cause of anterior neck masses Children
Most common neoplastic condition Male predominance Greater chance of malignancy Adults Mostly benign Female predominance

27
Thyroid Masses Lymph node metastatic 15% of papillary carcinomas
40% with malignant nodules Histologically in >90% (microscopic) FNAB is standard of care Decreases # of patients with surgery Increases # of malignant tumors found at surgery Doubles # of cases followed up Repeat negative aspiration in 1 month
 FNAB is standard of care. Decreases # of patients with surgery. Increases # of malignant tumors found at surgery. Doubles # of cases followed up. Repeat negative aspiration in 1 month.")
28
Rational approach to Management of a Thyroid nodule

29
Lymphoma More common in pediatric & young adults
80% of children with Hodgkin’s have neck mass Signs and symptoms Mass only, fever, hepatosplenomegaly, diffuse adenopathy FNAB - 1st line; open biopsy if suggestive CT scans (H&N, chest, abdomen) & bone marrow biopsy
 & bone marrow biopsy.")
30
Salivary Tumors Any preauricular enlarging mass or at the angle of the mandible is suspicious Benign - asymptomatic Metastatic - rapid growth, skin fixation or cranial nerve palsies Open excisional biopsy preferred

31
Salivary Tumors FNAB Reduces # of patients with surgery by 1/3 Distinguishes intra-glandular lymph nodes, localized sialadenitis, benign cysts Accuracy >90% (better for benign) Sensitivity - 90%; Specificity - 80% May facilitate surgical planning or patient counseling Prepare for total parotidectomy & nerve sacrifice in unknown primaries
 Sensitivity - 90%; Specificity - 80% May facilitate surgical planning or patient counseling. Prepare for total parotidectomy & nerve sacrifice in unknown primaries.")
32
Carotid Body and Glomus Tumor
Rare in the pediatric population Classical presentation Adult Pulsatile, compressible mass at carotid bifurcation Mobile side to side Diagnosis confirmed by angiography or CT

33
Carotid Body and Glomus Tumor
Treatment Elderly adult Observation Irradiation to arrest growth Young adult Resection of small tumors Hypotensive anesthesia Preoperative embolization and measurement of catecholamines release

34
Lipoma Over age 35 usually Ill-defined, soft masses
Diagnosis confirmed by excisional biopsy

35
Neurogenic Tumors Peripheral nervous system tumors
Arise from neural crest derivatives Include schwannomas, neurofibromas and malignant peripheral nerve sheath tumors Increased incidence in NF syndromes Schwannomas occur most commonly MPNST uncommon in head and neck

36
Neurogenic Tumors Schwannoma Benign
Any age, but most common 20 to 50 years Solitary, slowly enlarging, painless mass Medial tonsillar displacement Hoarseness (vagus nerve) Horner’s (sympathetic chain) Surgical excision is treatment of choice
 Horner’s (sympathetic chain) Surgical excision is treatment of choice.")
37
Congenital and Developmental Masses
Epidermal and Sebaceous cysts Branchial Cleft Cysts Thyroglossal Duct Cysts Vascular Tumors

38
Epidermal and Sebaceous Cysts
Most common congenital mass Older age group most often Clinical diagnosis - movement and elevation of overlying skin Excisional biopsy confirms

39
Branchial Cleft Cysts Late childhood or early adulthood
Often appears rapidly after URI Skin erythema and tenderness after recent infection May express purulent material if sinus tract is present Treatment is initial control of infection, followed by surgical excision

40
Branchial Cleft Cysts 1st branchial cleft cyst 2nd most common
Inferior or angle of the mandible or below the ear lobe Close association with facial nerve possible Excision may require total parotidectomy and facial nerve dissection

41
Branchial Cleft Cysts 2nd branchial cleft cyst
Most common Underlying SCM Tract courses medial over 12th nerve and between internal and external carotids 3rd and 4th branchial cleft cysts Rarely reported

42
Thyroglossal Duct Cysts
Most common congenital neck mass Midline or near-midline mass Elevates on swallowing or protrusion of the tongue Differential: lymph nodes, dermoids, ectopic thyroid tissue Surgical removal (Sistrunk) after resolution of infection
 after resolution of infection.")
43
Vascular Tumors Almost always present within 1st year
CT/MRI help in diagnosis and defining extent of lesion Lymphangioma Remain unchanged into adulthood Soft, doughy, ill-defined Treatment: excision for easily accessible or vital function compromise

44
Vascular Tumors Hemangiomas Most often resolve spontaneously
Bluish, compressible Surgical treatment Rapid growth Associated thrombocytopenia Involvement of vital structures After failure of medical therapy

45
Inflammatory Disorders
Lymphadenitis Granulomatous lymphadenitis

46
Lymphadenitis Very common, especially during 1st decade
Marked tenderness, torticollis, trismus, and dysphagia Systemic signs of infection Initial treatment - directed antibiotics Close follow up

47
Lymphadenopathy Failure of antibiotics necessitates biopsy after complete head and neck work-up FNAB indications Progressively enlarging nodes Solitary, asymmetric nodal mass Supraclavicular mass Persistent nodes without infectious signs

48
Lymphadenopathy Equivocal or suspicious FNAB in the pediatric nodal mass requires open excisional biopsy to rule out lymphoma or granulomatous disease

49
Granulomatous Lymphadenitis
Develop over weeks and months Minimal systemic complaints or findings Firm glands, fixation and injection of skin Common etiologies Typical Mycobacterium tuberculosis (adults) Atypical Mycobacterium tuberculosis (children) Cat-scratch fever (Bartonella henselae) (children) Actinomycosis, Sarcoidosis
 Atypical Mycobacterium tuberculosis (children) Cat-scratch fever (Bartonella henselae) (children) Actinomycosis, Sarcoidosis.")
50
Granulomatous Lymphadenitis
Atypical TB Anterior triangle lymph nodes Brawny skin, induration and pain Usually responds to complete surgical excision Cat-scratch fever Preauricular or submandibular lymph nodes Spontaneous resolution 1-2 months Typical TB (rarely seen, posterior nodes)
")
51
Summary Extensive differential diagnosis Thorough work-up needed
FNAB invaluable Malignancy should never be overlooked Close follow-up and aggressive pursuit of a diagnosis essential

52
Good luck

Similar presentations