Download presentation
Presentation is loading. Please wait.

1
THE PLACENTA Presenters: LIJOHI, Fatma Abdallah (MMED-OBS&GYN)
Dr. LIKONDANGOMA, Shaaban Alli (MMED-OBS&GYN ) Facilitator: Prof. D. Ngassapa
 Facilitator: Prof. D. Ngassapa.")
2
outline Introduction Development Structure Circulation of the placenta
Placental membrane Functions Classification Clinical application

3
introduction The placenta (Greek, plakuos = flat cake) named on the basis of this organs gross anatomical appearance Is a mateno-fetal organ which begins developing at implantation of the blastocyst and is delivered with the fetus at birth During the 9 month period it provides nutrition, gas exchange, waste removal, endocrine and immune support for the developing fetus

4
Shape and size The human placenta at term, is flat and circular or oval in shape Average volume of 500ml; average weight of 500mg The diameter of 15 to 25cm while the average thickness is about 3cm The placenta is thickest at the middle and thin at the periphery where it is continuous with the chorion leave

5
Appearance and surface
Has a smooth shiny fetal surface and rough and granular maternal surface The fetal surface is covered by amnion and beneath it is the chorion which has mottled appearance Umbilical cord attaches near the center of the fetal surface and branches of the umbilical vessels spread out under the amnion from this area The umbilical vein are larger and deeper than the arteries.

6
Cont… The remnants of the yolk sac and connecting stalk can also be found beneath amnion in the fetal surface The roughness of the maternal surface is due to presence of 15 to 20 lobes separated by a series of fissures or grooves. The lobes are termed cotyledons while the grooves correspond to the bases of incomplete placenta septae

7
Diagram of the placenta

8
Development The fetal component of the placenta is derived from the trophoblast and extraembryonic mesoderm (the chorionic plate); the maternal component is derived from the uterine endometrium The development of placenta can be summarized in the following steps; 1)Formation of blood filled lacunae and intervening trabeculae in the syntiotrophoblast
; the maternal component is derived from the uterine endometrium. The development of placenta can be summarized in the following steps; 1)Formation of blood filled lacunae and intervening trabeculae in the syntiotrophoblast.")
10
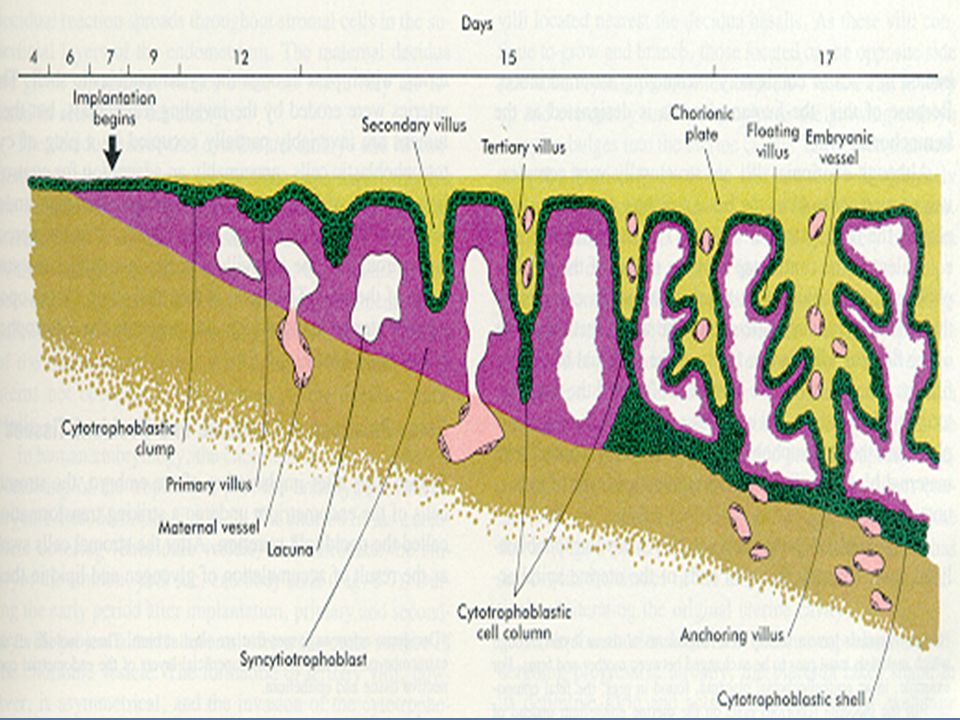
Development cont 2) invasion of trabeculae by the trophoblast (to form primary villi) by extraembryonic mesoderm (to form secondary villi) and by blood vessels ( to form tertiary stem villi) Stem villi are also known as anchoring villi, they connect the chorion to the basal plate 3)lateral spread of the cytotrophoblast to form the cytotrophoblast shell thereby converting the lacunae into intervillous spaces. The cytotrophoblastic shell is a mechanism to allow for rapid circumferential growth of the chorion (and later the placenta).This leads to expansion of the intervillous space
 invasion of trabeculae by the trophoblast (to form primary villi) by extraembryonic mesoderm (to form secondary villi) and by blood vessels ( to form tertiary stem villi) Stem villi are also known as anchoring villi, they connect the chorion to the basal plate. 3)lateral spread of the cytotrophoblast to form the cytotrophoblast shell thereby converting the lacunae into intervillous spaces. The cytotrophoblastic shell is a mechanism to allow for rapid circumferential growth of the chorion (and later the placenta).This leads to expansion of the intervillous space.")
11
Development cont 4) Sprouting of primary villous stems into the intervillous space. By the 21st postovulatory day these have developed into highly branched secondary and tertiary villi. Stem villi do not reach the basal plate 5)Degeneration of villi on the side of the decidua parietalis while those in the decidua basalis persist as the chorion frondosum 6) proliferation and growth of the chorion frondosum into the definitive placenta. Formation of chorion leave and chorion frondosum occur btn 21st postovulatory day and the end of fourth month of gestation
 Sprouting of primary villous stems into the intervillous space. By the 21st postovulatory day these have developed into highly branched secondary and tertiary villi. Stem villi do not reach the basal plate. 5)Degeneration of villi on the side of the decidua parietalis while those in the decidua basalis persist as the chorion frondosum. 6) proliferation and growth of the chorion frondosum into the definitive placenta. Formation of chorion leave and chorion frondosum occur btn 21st postovulatory day and the end of fourth month of gestation.")
13
Development cont 7) the appearance of folds of the basal plate which grow towards the chorionic plate These folds are known as placental septae and appear during third month of gestation They result from regional variability of placental growth and partly by pulling of the basal plate into the intervillous space by anchoring villi with a poor growth rate The placental septa divide maternal surface into 15 to 20 lobes(cotyledons)
")
14
Development of the Placenta

15
structure Placenta consists of a chorionic plate (fetal component of the placenta) and a basal plate (maternal component) of the placenta The latter has no villous stems and their branches The intervillous space which is filled with maternal blood intervenes btn the two plates

17
Structure cont On the fetal side, the placenta is bordered by the chorionic plate, on its maternal side, it is bordered by the decidua basalis, of which the decidual plate is most intimately incorporated into the placenta In the junctional zone, trophoblast and decidual cells intermingle. This zone, characterized by decidual and syncytial giant cells, is rich in amorphous extracellular material

18
Structure cont By this time, most cytotrophoblast cells have degenerated Between the chorionic and decidual plates are the intervillous spaces, which are filled with maternal blood They are derived from lacunae in the syncytiotrophoblast and are lined with syncytium of fetal origin The villous trees grow into the intervillous blood lakes

19
Structure cont During the fourth and fifth months, the decidua forms a number of decidual septa, which project into intervillous spaces but do not reach the chorionic plate These septa have a core of maternal tissue, but their surface is covered by a layer of syncytial cells, so that at all times, a syncytial layer separates maternal blood in intervillous lakes from fetal tissue of the villi As a result of this septum formation, the placenta is divided into a number of compartments, or cotyledons Because the decidual septa do not reach the chorionic plate, contact between intervillous spaces in the various cotyledons is maintained

20
Structure cont As a result of the continuous growth of the fetus and expansion of the uterus, the placenta also enlarges. Its increase in surface area roughly parallels that of the expanding uterus, and throughout pregnancy, it covers approximately 15% to 30% of the internal surface of the uterus. The increase in thickness of the placenta results from arborization of existing villi and is not caused by further penetration into maternal tissues

21
Circulation of the Placenta
Cotyledons receive their blood through 80 to 100 spiral arteries that pierce the decidual plate and enter the intervillous spaces at more or less regular intervals. Pressure in these arteries forces the blood deep into the intervillous spaces and bathes the numerous small villi of the villous tree in oxygenated blood. As the pressure decreases, blood flows back from the chorionic plate toward the decidua, where it enters the endometrial veins. Hence, blood from the intervillous lakes drains back into the maternal circulation through the endometrial veins.

22
cont Collectively, the intervillous spaces of a mature placenta contain approximately 150 mL of blood, which is replenished about three or four times per minute This blood moves along the chorionic villi, which have a surface area of 4 to 14 m2 Placental exchange does not take place in all villi, however, only in those that have fetal vessels in intimate contact with the covering syncytial membrane In these villi, the syncytium often has a brush border consisting of numerous microvilli, which greatly increases the surface area and consequently the exchange rate between maternal and fetal circulations

24
Placental membrane or barrier
The placental membrane separates maternal and fetal blood; is composed of four layers from the fetus to mother: (1) the endothelial lining of fetal vessels, (2) the connective tissue in the villus core, (3) the cytotrophoblastic layer, and (4) the syncytium From the fourth month on, the placental membrane thins because the endothelial lining of the vessels comes in intimate contact with the syncytial membrane, greatly increasing the rate of exchange
 the endothelial lining of fetal vessels, (2) the connective tissue in the villus core, (3) the cytotrophoblastic layer, and. (4) the syncytium. From the fourth month on, the placental membrane thins because the endothelial lining of the vessels comes in intimate contact with the syncytial membrane, greatly increasing the rate of exchange.")
25
cont Sometimes it is called the placental barrier, but it is not a true barrier, as many substances pass through it freely Because the maternal blood in the intervillous spaces is separated from the fetal blood by a chorionic derivative, the human placenta is considered to be of the hemochorial type Normally, there is no mixing of maternal and fetal blood However, small numbers of fetal blood cells occasionally escape across microscopic defects in the placental membrane

27
Placental growth The placenta increases in both surface area and thickness in the first half of pregnancy Growth in depth is due to elongation of the villous and not by further invasion of the decidua By the fourth month of gestation the placenta has achieved its definite form In the second half of pregnancy the placenta doubles its surface area by continued growth and arborization of the villous tree and formation of fresh villi

28
Functions of the placenta
1) respiratory gases exchange by uptake of oxygen from the intervillous space and the release of carbondioixde into intervillous space 2) passive and active transport of nutritive materials eg water, glucose, aa,lipids, vitamins,electrolytes to reach the fetus 3) route of excretion of the end products of fetal metabolism.eg urea, uric, creatinine 4)provides protection in two ways -prevents passage of pathogenic organisms and toxins. -allows passage of maternal antibodies into the fetus(especially IgG).
 respiratory gases exchange by uptake of oxygen from the intervillous space and the release of carbondioixde into intervillous space. 2) passive and active transport of nutritive materials eg water, glucose, aa,lipids, vitamins,electrolytes to reach the fetus. 3) route of excretion of the end products of fetal metabolism.eg urea, uric, creatinine. 4)provides protection in two ways. -prevents passage of pathogenic organisms and toxins. -allows passage of maternal antibodies into the fetus(especially IgG).")
29
Cont… 5)Immunological barrier btn the fetus and the mother
The fetal-placental unit is dissmilar to maternal tissue, however doesnot elicite any apparent allograft rejection reactions. This is b’coz the trophoblast acts as immunological barrier by the following factors; -absence of MHC antigens in the trophoblast rendering it nonantigenic. - secretion of fibrinoid or sialomucin by trophoblastic cells to mask surface antigens. -binding of receptors on the trophoblast by Ag-Ab complex which inhibit immunological interaction -suppresion of cellular and humoral immunity of the mother by trophoblastic hormones(progesterone,HCG)
")
30
Cont… 6)chorionic plate of the placenta is an endocrine organ responsible for production of estrogen,progesterone,HCG,HCS(human chorionic somatomammotropin),HCT(human chorionic thyrotropin)
chorionic plate of the placenta is an endocrine organ responsible for production of estrogen,progesterone,HCG,HCS(human chorionic somatomammotropin),HCT(human chorionic thyrotropin)")
31
Classification of placenta
Placenta can be classified according to the following criteria: A)Attachment of umbilical cord and vessels -battle-dore placenta- umbilical cord is attached close to the margin of the placenta -velamentous placenta-umbilical vessels are not gathered together to form an umbilical cord attaching directly to the placenta but ramify on the chorion leave before entering the placenta
Attachment of umbilical cord and vessels -battle-dore placenta- umbilical cord is attached close to the margin of the placenta -velamentous placenta-umbilical vessels are not gathered together to form an umbilical cord attaching directly to the placenta but ramify on the chorion leave before entering the placenta")
32
Velamentous placenta

34
Classification cont B)site of implantation eg
placenta praevia- the blastocyst becomes implanted into the lower segment of the uterus near the internal os. it can be Central placental praevia-completely covers the os. Partial placenta praevia-only the edge of the placenta covers part of the os. Marginal placenta praevia-the placenta reaches only the lower segment.

35
Classification cont C) presence of accessory lobes –there is an accessory lobe called the placenta succenturiata D) degree of penetration -placenta accreta-pathological adhesion of the chorion to the deciduas basalis -placenta incerta-chorionic villi enter myometrium -placenta perceta-villi broach the entire uterine wall
 presence of accessory lobes –there is an accessory lobe called the placenta succenturiata D) degree of penetration -placenta accreta-pathological adhesion of the chorion to the deciduas basalis -placenta incerta-chorionic villi enter myometrium -placenta perceta-villi broach the entire uterine wall")
36
Classification cont E) Classification on the basis of histological (microscopic) structural organization and layers between fetal and maternal circulation. Five groups: Haemochorial - placenta where the chorion comes in direct contact with maternal blood (human) Endotheliochorial - maternal endometrial blood vessels are bare to their endothelium and these comes in contact with the chorion (dogs, cats) Epitheliochorial - maternal epithelium of the uterus comes in contact with the chorion, considered as primitive (pigs, cows) Syndesmochorial- endometrial epithelium is missing and the chorion is separated from maternal blood by endometrial stroma and fetal endothelium(cattle) Haemo-endothelial- is like haemochorial variety with additional disappearance of trophoblastic cells of chorion so that maternal blood is in contact with endothelium of fetal vessels(rabbits)
 Classification on the basis of histological (microscopic) structural organization and layers between fetal and maternal circulation. Five groups: Haemochorial - placenta where the chorion comes in direct contact with maternal blood (human) Endotheliochorial - maternal endometrial blood vessels are bare to their endothelium and these comes in contact with the chorion (dogs, cats) Epitheliochorial - maternal epithelium of the uterus comes in contact with the chorion, considered as primitive (pigs, cows) Syndesmochorial- endometrial epithelium is missing and the chorion is separated from maternal blood by endometrial stroma and fetal endothelium(cattle) Haemo-endothelial- is like haemochorial variety with additional disappearance of trophoblastic cells of chorion so that maternal blood is in contact with endothelium of fetal vessels(rabbits)")
37
Clinical correlation Placenta Accreta - abnormal adherence, with absence of decidua basalis The incidence of placenta accreta also significantly increases in women with previous cesarean section compared to those without a prior surgical delivery Placenta Increta - occurs when the placenta attaches deep into the uterine wall and penetrates into the uterine muscle, but does not penetrate the uterine serosa. Placenta increta accounts for approximately 15-17% of all cases Placenta Percreta - placental villi penetrate myometrium and through to uterine serosa

38
cont Placenta Previa - In this placental abnormality, the placenta overlies internal os of uterus, essentially covering the birth canal This condition occurs in approximately 1 in 200 to 250 pregnancies In the third trimester and at term, abnormal bleeding can require caesarian delivery Vasa Previa - (vasa praevia) placental abnormality where the fetal vessels lie within the membranes close too or crossing the inner cervical os (opening) This occurs normally in 1: pregnancies and leads to complications similar too those for Placenta Previa Type II is defined as the condition where the fetal vessels are found crossing over the internal os connecting either a bilobed placenta or a succenturiate lobe with the main placental mass.
 placental abnormality where the fetal vessels lie within the membranes close too or crossing the inner cervical os (opening) This occurs normally in 1: pregnancies and leads to complications similar too those for Placenta Previa. Type II is defined as the condition where the fetal vessels are found crossing over the internal os connecting either a bilobed placenta or a succenturiate lobe with the main placental mass.")
39
cont Abruptio Placenta - a retroplacental blood clot formation, abnormal hemorrhage prior to delivery Chronic Intervillositis - (massive chronicintervillositis, chronic histiocytic intervillositis) Rare placental abnormality and pathology defined by inflammatory placental lesions, mainly in the intervillous space (IVS), with a maternal infiltrate of mononuclear cells (monocytes, lymphocytes, histiocytes) and intervillous fibrinoid deposition Hydatidiform mole - placental tumor with no embryo development. Several forms of hydatidiform mole: partial mole, complete mole and persistent gestational trophoblastic tumor Many of these tumours arise from a haploid sperm fertilizing an egg without a female pronucleus (the alternative form, an embryo without sperm contribution, is called parthenogenesis) The tumour has a "grape-like" placental appearance without enclosed embryo formation. Following a first molar pregnancy, there is approximately a 1% risk of a second molar pregnancy
 Rare placental abnormality and pathology defined by inflammatory placental lesions, mainly in the intervillous space (IVS), with a maternal infiltrate of mononuclear cells (monocytes, lymphocytes, histiocytes) and intervillous fibrinoid deposition. Hydatidiform mole - placental tumor with no embryo development. Several forms of hydatidiform mole: partial mole, complete mole and persistent gestational trophoblastic tumor. Many of these tumours arise from a haploid sperm fertilizing an egg without a female pronucleus (the alternative form, an embryo without sperm contribution, is called parthenogenesis) The tumour has a grape-like placental appearance without enclosed embryo formation. Following a first molar pregnancy, there is approximately a 1% risk of a second molar pregnancy.")
40
References Essentials of Human Embryology by Ngassapa,D & Kaduri
Langmans medical embryology

Similar presentations
















>")







