Download presentation
Presentation is loading. Please wait.

1
Journal Club 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi 2015 年 4 月 2 日 8:30-8:55 8階 医局 Robinson JG, Farnier M, Krempf M, Bergeron J, Luc G, Averna M, Stroes ES, Langslet G, Raal FJ, Shahawy ME, Koren MJ, Lepor NE, Lorenzato C, Pordy R, Chaudhari U, Kastelein JJ; ODYSSEY LONG TERM Investigators. Efficacy and Safety of Alirocumab in Reducing Lipids and Cardiovascular Events. N Engl J Med. 2015 Mar 15. [Epub ahead of print] Bateman BT, Hernandez-Diaz S, Fischer MA, Seely EW, Ecker JL, Franklin JM, Desai RJ, Allen-Coleman C, Mogun H, Avorn J, Huybrechts KF. Statins and congenital malformations: cohort study. BMJ. 2015 Mar 17;350:h1035. doi: 10.1136/bmj.h1035.

2
http://www.pcsk9forum.org/

3
statins ezetimibe partial ileal bypass portacaval shunt liver transplantation LDL apheresis mipomersen lomitapide Treatment of homozygous familial hypercholesterolaemia alirocumab evolocumab bococizumab (ALN-PCS) PCSK9 target
 PCSK9 target")
4
KYNAMROTM (mipomersen sodium) KYNAMRO TM is an oligonucleotide inhibitor of apolipoprotein B-100 synthesis Lancet 2010; 375: 998–1006
 KYNAMRO TM is an oligonucleotide inhibitor of apolipoprotein B-100 synthesis Lancet 2010; 375: 998–1006")
5
Lomitapide (INN, marketed as Juxtapid) is a drug for the treatment of familial hypercholesterolemia, developed by Aegerion Pharmaceuticals. It has been tested in clinical trials as single treatment and in combinations with atorvastatin, ezetimibe and fenofibrate. The US Food and Drug Administration (FDA) approved lomitapide on 21 December 2012, as an orphan drug to reduce LDL cholesterol, total cholesterol, apolipoprotein B, and non-high-density lipoprotein (non-HDL) cholesterol in patients with homozygous familial hypercholesterolemia (HoFH). http://en.wikipedia.org/wiki/Lomitapide Lomitapide inhibits the microsomal triglyceride transfer protein (MTP or MTTP) which is necessary for very low-density lipoprotein (VLDL) assembly and secretion in the liver.
 approved lomitapide on 21 December 2012, as an orphan drug to reduce LDL cholesterol, total cholesterol, apolipoprotein B, and non-high-density lipoprotein (non-HDL) cholesterol in patients with homozygous familial hypercholesterolemia (HoFH). Lomitapide inhibits the microsomal triglyceride transfer protein (MTP or MTTP) which is necessary for very low-density lipoprotein (VLDL) assembly and secretion in the liver..")
6
PCSK9 (neural apoptosis-regulated convertase, NARC-1) is a 692-residue extracellular protein representing the 9th member of the secretory subtilase family expressed primarily in the kidneys, liver and intestines. http://caltagmedsystems.blogspot.jp/2012/04/pcsk9-attractive-drug-target-for.html Genetic studies mapped PCSK9 along with LDLR and APOB to cause autosomal dominant hypercholesterolemia (ADH). Gain-of-function mutations increased plasma levels of low-density lipoprotein cholesterol (LDL-C), whereas nonsense or missense (loss-of-function) mutations, which interfere with folding or secretion of PCSK9, led to a reduction of plasma levels of LDL-C and an 88% decrease in the risk of coronary heart disease (CHD). Proprotein convertase subtilisin/kexin type 9
. Gain-of-function mutations increased plasma levels of low-density lipoprotein cholesterol (LDL-C), whereas nonsense or missense (loss-of-function) mutations, which interfere with folding or secretion of PCSK9, led to a reduction of plasma levels of LDL-C and an 88% decrease in the risk of coronary heart disease (CHD). Proprotein convertase subtilisin/kexin type 9.")
7
Lancet. 2014 Jan 4;383(9911):60-8.
:60-8.")
8
N Engl J Med 2012;366:1108-18. single ascending-dose studies of REGN727 抗体治療!! Alirocumab SAR236553 (REGN727)
.")
9
N Engl J Med 2012;367:1891-900. DOI: 10.1056/NEJMoa1201832 抗体治療 + スタチン Alirocumab SAR236553 (REGN727) primary hypercholesterolemia
 primary hypercholesterolemia.")
10
Lancet. 2014 Jan 4;383(9911):60-8.Effect of ALN-PCS treatment on serum LDL cholesterol ALN-PCS:a small interfering RNA that inhibits PCSK9 synthesis
:60-8.Effect of ALN-PCS treatment on serum LDL cholesterol ALN-PCS:a small interfering RNA that inhibits PCSK9 synthesis.")
11
Lancet. 2015 Jan 24;385(9965):341-50.
:")
12
the University of Iowa, Iowa City (J.G.R.); Point Médical, Dijon (M.F.), Centre Hospitalier Universitaire de Nantes– Hôpital Nord Laennec, Saint-Herblain (M.K.), University Hospital of Lille, Lille (G. Luc), and Sanofi, Chilly-Mazarin (C.L.) — all in France; Clinique des Maladies Lipidiques de Québec, Quebec, QC, Canada (J.B.); Università di Palermo–Policlinico P. Giaccone, Palermo, Italy (M.A.); the Department of Vascular Medicine, Academic Medical Center, Amsterdam (E.S.S., J.J.P.K.); Lipid Clinic, Oslo University Hospital, Oslo (G. Langslet); University of the Witwatersrand, Johannesburg (F.J.R.); Cardiovascular Center of Sarasota, Sarasota (M.E.S.), and Jacksonville Center for Clinical Research, Jacksonville (M.J.K.) — both in Florida; Westside Medical Associates of Los Angeles, Beverly Hills, CA (N.E.L.); Regeneron Pharmaceuticals, Tarrytown, NY (R.P.); and Sanofi, Bridgewater, NJ (U.C.). N Engl J Med. 2015 Mar 15. [Epub ahead of print]
, and Sanofi, Chilly-Mazarin (C.L.) — all in France; Clinique des Maladies Lipidiques de Québec, Quebec, QC, Canada (J.B.); Università di Palermo–Policlinico P. Giaccone, Palermo, Italy (M.A.); the Department of Vascular Medicine, Academic Medical Center, Amsterdam (E.S.S., J.J.P.K.); Lipid Clinic, Oslo University Hospital, Oslo (G. Langslet); University of the Witwatersrand, Johannesburg (F.J.R.); Cardiovascular Center of Sarasota, Sarasota (M.E.S.), and Jacksonville Center for Clinical Research, Jacksonville (M.J.K.) — both in Florida; Westside Medical Associates of Los Angeles, Beverly Hills, CA (N.E.L.); Regeneron Pharmaceuticals, Tarrytown, NY (R.P.); and Sanofi, Bridgewater, NJ (U.C.). N Engl J Med Mar 15. [Epub ahead of print].")
13
Background Alirocumab, a monoclonal antibody that inhibits proprotein convertase subtilisin–kexin type 9 (PCSK9), has been shown to reduce low-density lipoprotein (LDL) cholesterol levels in patients who are receiving statin therapy. Larger and longer-term studies are needed to establish safety and efficacy.

14
Methods We conducted a randomized trial involving 2341 patients at high risk for cardiovascular events who had LDL cholesterol levels of 70 mg per deciliter (1.8 mmol per liter) or more and were receiving treatment with statins at the maximum tolerated dose (the highest dose associated with an acceptable side- effect profile), with or without other lipid-lowering therapy. Patients were randomly assigned in a 2:1 ratio to receive alirocumab (150 mg) or placebo as a 1-ml subcutaneous injection every 2 weeks for 78 weeks. The primary efficacy end point was the percentage change in calculated LDL cholesterol level from baseline to week 24.
 or placebo as a 1-ml subcutaneous injection every 2 weeks for 78 weeks. The primary efficacy end point was the percentage change in calculated LDL cholesterol level from baseline to week 24..")
15
Figure S1. Study Design Abbreviations: CV, cardiovascular; HeFH, heterozygous familial hypercholesterolemia; LDL-C, lowdensity lipoprotein cholesterol; LLT, lipid-lowering therapy; Q2W, every other week; SC, subcutaneous; W, week. ClinicalTrials.gov identifier: NCT01507831

16
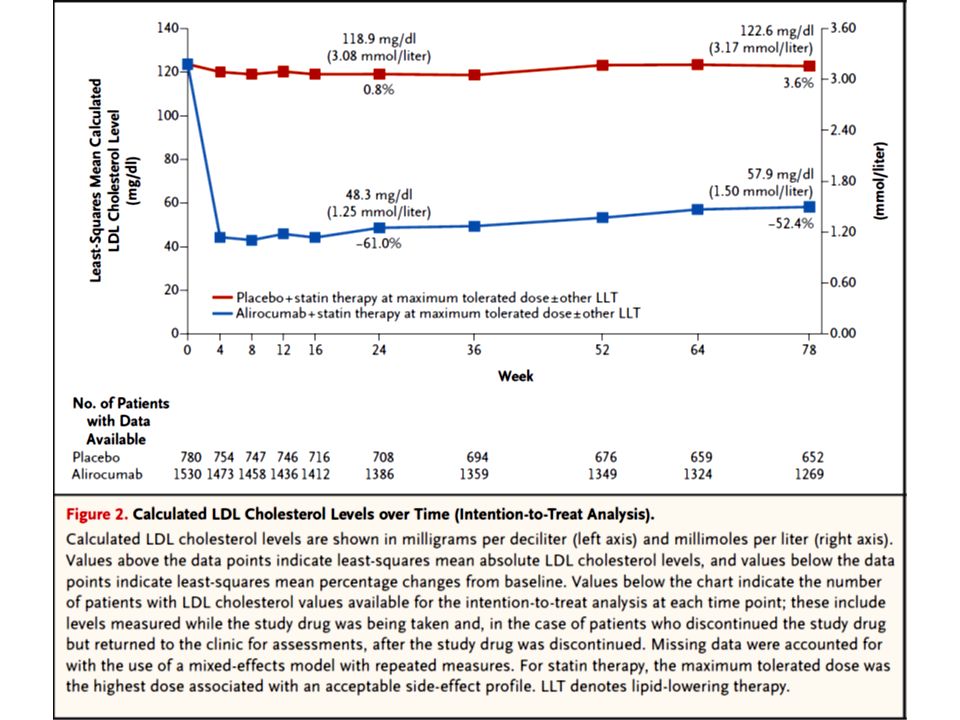
Figure 1. Randomization and Treatment. The intention-to-treat population included all randomly assigned patients who had both a baseline calculated low-density lipoprotein (LDL) cholesterol value and at least one calculated LDL cholesterol value during one of the analysis windows up to week 24. The three patients in the alirocumab group who underwent randomization but did not receive treatment are included in the intention-to-treat population. Completion of the study was defined, as per the electronic case-report form, in the following way: the last study-drug injection was received (week 76), and the end-of-treatment visit (week 78) occurred within 21 days after the last injection and at least 525 days after randomization.
 cholesterol value and at least one calculated LDL cholesterol value during one of the analysis windows up to week 24. The three patients in the alirocumab group who underwent randomization but did not receive treatment are included in the intention-to-treat population. Completion of the study was defined, as per the electronic case-report form, in the following way: the last study-drug injection was received (week 76), and the end-of-treatment visit (week 78) occurred within 21 days after the last injection and at least 525 days after randomization..")
17
* Plus–minus values are means ±SD. The P value for all between-group comparisons was greater than 0.05, indicating no significant differences. To convert the values for cholesterol to millimoles per liter, multiply by 0.02586. To convert the values for triglycerides to millimoles per liter, multiply by 0.01129. HDL denotes high-density lipoprotein, and LDL low-density lipoprotein. † Race was self-reported. ‡ The body-mass index is the weight in kilograms divided by the square of the height in meters. § Heterozygous familial hypercholesterolemia was diagnosed by means of genotyping in 40.2% of the patients in the two groups combined and by clinical criteria (World Health Organization–Simon Broome diagnostic criteria) in 59.8% of the patients in the two groups combined. ¶ Coronary heart disease risk equivalents were defined as peripheral arterial disease, ischemic stroke, moderate chronic kidney disease (estimated glomerular filtration rate, 30 to 2+ protein; preproliferative or proliferative retinopathy or laser treatment for retinopathy; or a family history of premature coronary heart disease). ‖ High-dose statin therapy was defined as a daily dose of 40 to 80 mg of atorvastatin, 20 to 40 mg of rosuvastatin, or 80 mg of simvastatin. ** LDL cholesterol levels were calculated with the use of the Friedewald formula and also measured by means of betaquantification (see Table S1 in the Supplementary Appendix).
 in 59.8% of the patients in the two groups combined. ¶ Coronary heart disease risk equivalents were defined as peripheral arterial disease, ischemic stroke, moderate chronic kidney disease (estimated glomerular filtration rate, 30 to 2+ protein; preproliferative or proliferative retinopathy or laser treatment for retinopathy; or a family history of premature coronary heart disease). ‖ High-dose statin therapy was defined as a daily dose of 40 to 80 mg of atorvastatin, 20 to 40 mg of rosuvastatin, or 80 mg of simvastatin. ** LDL cholesterol levels were calculated with the use of the Friedewald formula and also measured by means of betaquantification (see Table S1 in the Supplementary Appendix)..")
18
* Plus–minus values are least-squares means ±SE, unless otherwise indicated. Primary and secondary efficacy analyses were performed with the use of an intention-to-treat approach, which included patients with a baseline calculated LDL cholesterol value and at least one calculated LDL cholesterol value during or after receipt of the study drug within one of the analysis windows up to week 24. A prespecified analysis that included only patients who were receiving the study drug was also performed (Table S3 in the Supplementary Appendix). Least-squares means (±SE) and P values were calculated with the use of a mixed-effects model with repeated-measures analysis (except for end points noted in the footnotes below). The P values are significant according to the fixed hierarchical approach used to ensure control of the overall type I error rate at the 0.05 level. To convert values for cholesterol to millimoles per liter, multiply by 0.02586. CI denotes confidence interval. † Plus–minus values are means ±SD. ‡ The analysis of this end point was performed with the use of multiple imputation, followed by logistic regression. The combined estimate of the proportion of patients was obtained by calculation of the average of all the imputed proportions of patients meeting the level of interest. § The P value has not been adjusted for multiple testing and is provided for descriptive purposes only. ¶ The percentage change in levels of lipoprotein(a) and triglycerides was analyzed with the use of multiple imputation, followed by robust regression. A combined estimate for adjusted mean (±SE) is shown.
. Least-squares means (±SE) and P values were calculated with the use of a mixed-effects model with repeated-measures analysis (except for end points noted in the footnotes below). The P values are significant according to the fixed hierarchical approach used to ensure control of the overall type I error rate at the 0.05 level. To convert values for cholesterol to millimoles per liter, multiply by CI denotes confidence interval. † Plus–minus values are means ±SD. ‡ The analysis of this end point was performed with the use of multiple imputation, followed by logistic regression. The combined estimate of the proportion of patients was obtained by calculation of the average of all the imputed proportions of patients meeting the level of interest. § The P value has not been adjusted for multiple testing and is provided for descriptive purposes only. ¶ The percentage change in levels of lipoprotein(a) and triglycerides was analyzed with the use of multiple imputation, followed by robust regression. A combined estimate for adjusted mean (±SE) is shown..")
25
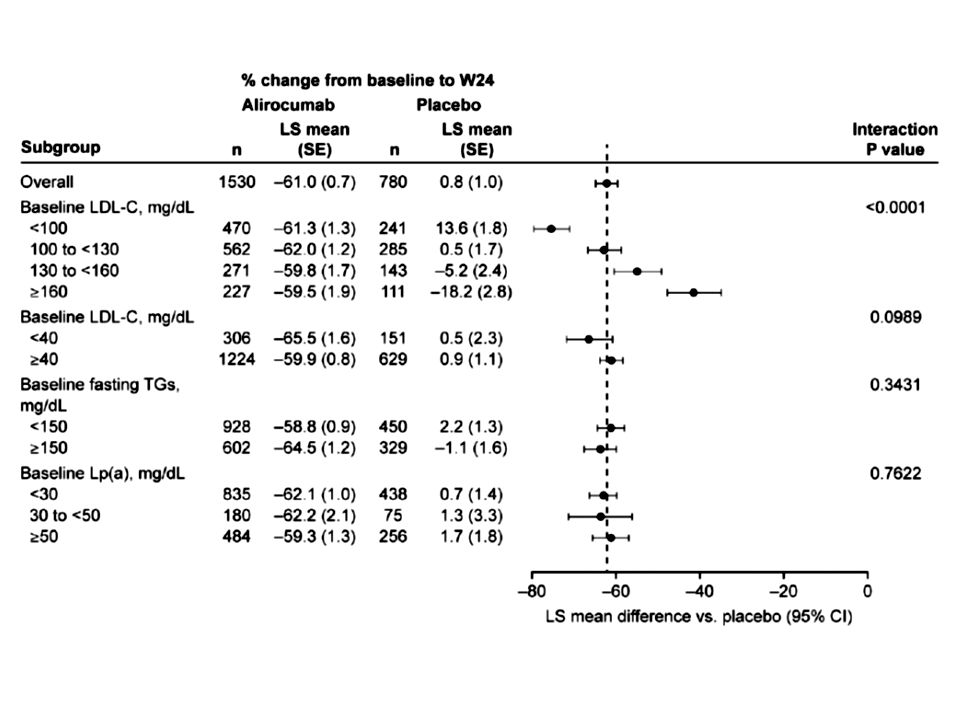
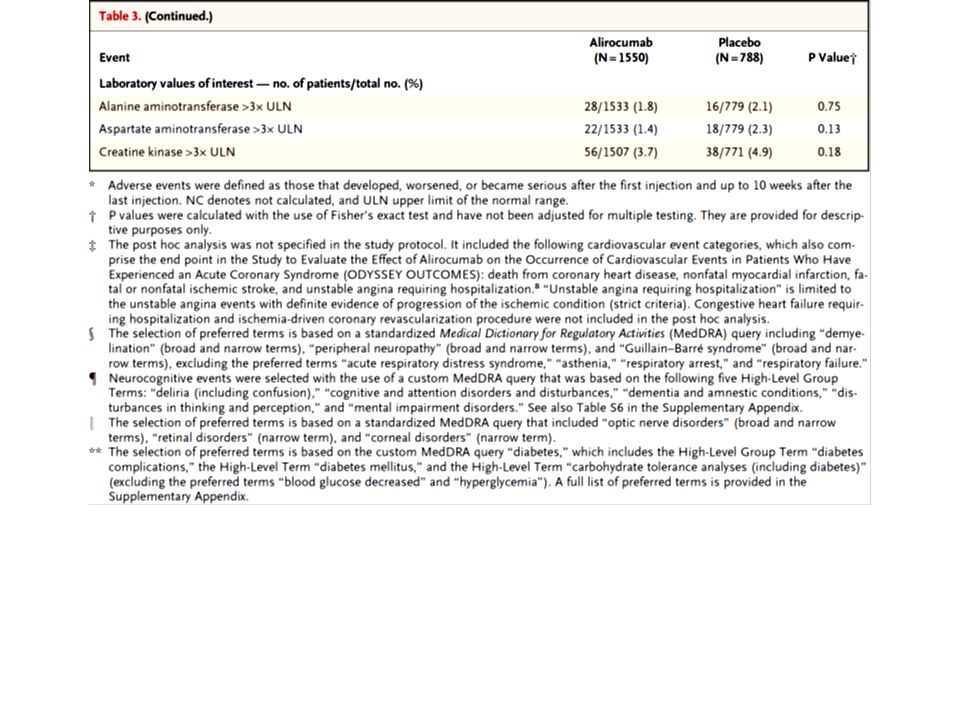
Results At week 24, the difference between the alirocumab and placebo groups in the mean percentage change from baseline in calculated LDL cholesterol level was −62 percentage points (P<0.001); the treatment effect remained consistent over a period of 78 weeks. The alirocumab group, as compared with the placebo group, had higher rates of injection-site reactions (5.9% vs. 4.2%), myalgia (5.4% vs. 2.9%), neurocognitive events (1.2% vs. 0.5%), and ophthalmologic events (2.9% vs. 1.9%). In a post hoc analysis, the rate of major adverse cardiovascular events (death from coronary heart disease, nonfatal myocardial infarction, fatal or nonfatal ischemic stroke, or unstable angina requiring hospitalization) was lower with alirocumab than with placebo (1.7% vs. 3.3%; hazard ratio, 0.52; 95% confidence interval, 0.31 to 0.90; nominal P=0.02).
, myalgia (5.4% vs. 2.9%), neurocognitive events (1.2% vs. 0.5%), and ophthalmologic events (2.9% vs. 1.9%). In a post hoc analysis, the rate of major adverse cardiovascular events (death from coronary heart disease, nonfatal myocardial infarction, fatal or nonfatal ischemic stroke, or unstable angina requiring hospitalization) was lower with alirocumab than with placebo (1.7% vs. 3.3%; hazard ratio, 0.52; 95% confidence interval, 0.31 to 0.90; nominal P=0.02)..")
26
Conclusions Over a period of 78 weeks, alirocumab, when added to statin therapy at the maximum tolerated dose, significantly reduced LDL cholesterol levels. In a post hoc analysis, there was evidence of a reduction in the rate of cardiovascular events with alirocumab. (Funded by Sanofi and Regeneron Pharmaceuticals; ODYSSEY LONG TERM ClinicalTrials.gov number, NCT01507831.)
.")
27
N Engl J Med. 2015 Mar 15. [Epub ahead of print] DOI: 10.1056/NEJMoa1500858
![N Engl J Med Mar 15. [Epub ahead of print] DOI: /NEJMoa](http://images.slideplayer.com/21/6328105/slides/slide_27.jpg "N Engl J Med Mar 15. [Epub ahead of print] DOI: /NEJMoa")
29
From the Departments of Medicine and Preventive Medicine and the Bluhm Cardiovascular Institute, Feinberg School of Medicine, Northwestern University, Chicago. Much work remains to be done, but PCSK9 inhibitors appear on track to become important arrows in our quiver for targeting reduction of cardiovascular events among higher-risk patients when statins are not enough.

30
Message 最大耐量スタチン治療下の患者 2341 人を対象に、 抗 PCSK9 モノクローナル抗体 alirocumab の LDL コレステロール低下効果を無作為化試験で検 討( ODYSSEY LONG TERM 試験)。プラセボ と比較したベースラインから 24 週の LDL コレス テロール変化率の差は- 62 %(P< 0.001 )で、 治療効果は 78 週間持続した。 https://www.m3.com/clinical/journal/15259 LDL-C はやはり低下させればさせるほどよいの であろうか???
。プラセボ と比較したベースラインから 24 週の LDL コレス テロール変化率の差は- 62 %(P< )で、 治療効果は 78 週間持続した。 LDL-C はやはり低下させればさせるほどよいの であろうか???")
32
BMJ 2015; 350 doi: http://dx.doi.org/10.1136/bmj.h1035 (Published 17 March 2015) 1 Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA, USA 2 Division of Obstetric Anesthesia, Department of Anesthesia, Critical Care, and Pain Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA 3 Department of Epidemiology, Harvard School of Public Health, Boston, MA, USA 4 Division of Endocrinology, Diabetes and Metabolism, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA 5 Department of Obstetrics and Gynecology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA
 1 Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA, USA 2 Division of Obstetric Anesthesia, Department of Anesthesia, Critical Care, and Pain Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA 3 Department of Epidemiology, Harvard School of Public Health, Boston, MA, USA 4 Division of Endocrinology, Diabetes and Metabolism, Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA 5 Department of Obstetrics and Gynecology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA")
33
Objective To examine the teratogenic potential of statins.

34
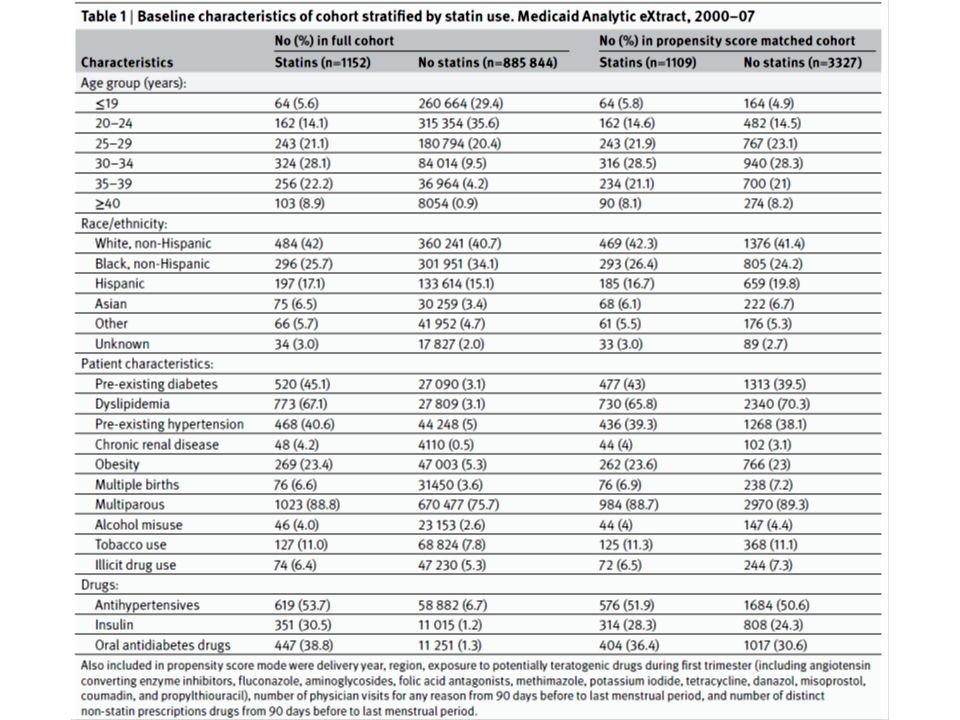
Design Cohort study. Setting United States. Participants A cohort of 886 996 completed pregnancies linked to liveborn infants of women enrolled in Medicaid from 2000 to 2007. Methods We examined the risk of major congenital malformations and organ specific malformations in offspring associated with maternal use of a statin in the first trimester. Propensity score based methods were used to control for potential confounders, including maternal demographic characteristics, obstetric and medical conditions, and use of other drugs.

36
Propensity Score A propensity score is the probability of a unit (e.g., person, classroom, school) being assigned to a particular treatment given a set of observed covariates. Propensity scores are used to reduce selection bias by equating groups based on these covariates. Suppose that we have a binary treatment T, an outcome Y, and background variables X. The propensity score is defined as the conditional probability of treatment given background variables: Let Y(0) and Y(1) denote the potential outcomes under control and treatment, respectively. Then treatment assignment is (conditionally) unconfounded if potential outcomes are independent of treatment conditional on background variables X. This can be written compactly as where denotes statistical independence.[1] If unconfoundedness holds, then Judea Pearl has shown that existence of a simple graphical criterion called backdoor path implies the presence of confounding variables. To estimate the effect of treatment, backdoor paths need to be blocked. This blocking can be done either by adding the confounding variable as a control in regression, or by matching on the confounding variable.
 and Y(1) denote the potential outcomes under control and treatment, respectively. Then treatment assignment is (conditionally) unconfounded if potential outcomes are independent of treatment conditional on background variables X. This can be written compactly as where denotes statistical independence.[1] If unconfoundedness holds, then Judea Pearl has shown that existence of a simple graphical criterion called backdoor path implies the presence of confounding variables. To estimate the effect of treatment, backdoor paths need to be blocked. This blocking can be done either by adding the confounding variable as a control in regression, or by matching on the confounding variable..")
39
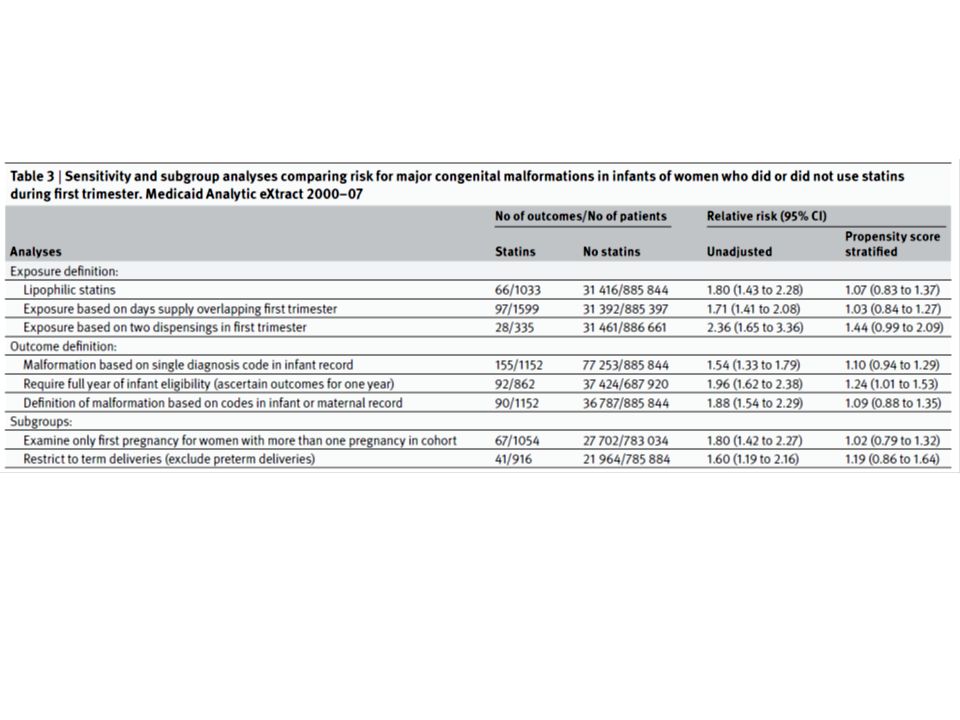
Results 1152 (0.13%) women used a statin during the first trimester. In unadjusted analyses, the prevalence of malformations in the offspring of these women was 6.34% compared with 3.55% in those of women who did not use a statin in the first trimester (relative risk 1.79, 95% confidence interval 1.43 to 2.23). Controlling for confounders, particularly pre-existing diabetes, accounted for this increase in risk (1.07, 0.85 to 1.37). There were also no statistically significant increases in any of the organ specific malformations assessed after accounting for confounders. Results were similar across a range of sensitivity analyses.
. Controlling for confounders, particularly pre-existing diabetes, accounted for this increase in risk (1.07, 0.85 to 1.37). There were also no statistically significant increases in any of the organ specific malformations assessed after accounting for confounders. Results were similar across a range of sensitivity analyses..")
40
Conclusions Our analysis did not find a significant teratogenic effect from maternal use of statins in the first trimester. However, these findings need to be replicated in other large studies, and the long term effects of in utero exposure to statins needs to be assessed, before use of statins in pregnancy can be considered safe.

41
Message 米国のメディケアデータ 88 万 6996 件を対象に、妊娠初 期のスタチン使用が産児の先天性奇形に与える影響をコ ホート研究で検討。 1152 人が妊娠初期にスタチンを使 用していた。奇形有病率はスタチン使用者 6.34 %、非 使用者 3.55 %(相対リスク 1.79 )。交絡因子で調整後 は 1.07 だった。調整後、臓器特異的な奇形有病率にも 増加はなかった。 https://www.m3.com/clinical/journal/15304 ただし、補正しなければ有意にリスクが増えるのは「妊娠可能性があるのにス タチンを用いているということ」自体がリスクなのであろう。 Propensity Score だと無作為化研究でなくても観察研究でそれに近い結果と なるらしい。最初 β ブロッカーの研究が有名らしい( Lindenauer PK, et al: Perioperative beta-blocker therapy and mortality after major noncardiac surgery. N Engl J Med. 2005 Jul 28;353(4):349-61. )
: ).")
42
sensitivity analysis 感応度分析 分析したいアウトプットをいくつかの変数(パラメータ)に分解し、その変数が変動し たとき、アウトプットにどの程度の影響を与えるかを調べる手法。 直感的に理解しやすい解析方法は、同じ治療割り当て確率の患者同士でペアを作って治 療群とコントロール群を比較する傾向スコアマッチング(プロペンシティスコアマッチ ング) propensity score (PS) matching 法です。このように傾向スコアの近い症例同士 をペアにするマッチング方法を caliper matching と呼び、症例 1 例に対してコントロー ル 1 例を割り当てる 1:1 マッチングが一般的です。 propensity score (PS) matching 傾向スコア
に分解し、その変数が変動し たとき、アウトプットにどの程度の影響を与えるかを調べる手法。 直感的に理解しやすい解析方法は、同じ治療割り当て確率の患者同士でペアを作って治 療群とコントロール群を比較する傾向スコアマッチング(プロペンシティスコアマッチ ング) propensity score (PS) matching 法です。このように傾向スコアの近い症例同士 をペアにするマッチング方法を caliper matching と呼び、症例 1 例に対してコントロー ル 1 例を割り当てる 1:1 マッチングが一般的です。 propensity score (PS) matching 傾向スコア")
Similar presentations













行列式の定義には、数学的な概念がいろいろ必要である。まずそれらを順に見ていく。>")






 入力データに含まれる、本来ほしくない 成分.>")
を体験したことにより興味を惹かれ るきっかけとなった。主な目的は、これ.>")



を生かした 確かな学力を形成する授業づく り ② 家庭との連携を図った家庭学習の習慣化.>")
