Download presentation
Presentation is loading. Please wait.

1
Urothelial Carcinoma: Cancer of the bladder, Ureter, Renal pelvis

2
Epidemiology 1-bladder cancer three time more common in men than in women. But women 30% higher chance of dying of bladder cancer / 2-bladder cancer is rare <50years, 3-median ages at diagnosis of around 70 years. 4-bladder cancer also occurs about half in whites than in African. 5- bladder cancer is never found incidentally at autopsy.and differences in incidence between genders, races,age

3
Basics &CLINICAL BIOLOGY All malignancies involve aberrations of normal mechanisms regulating cell differentiation. ( Alteration IN DNA ) 1-activation of oncogenes. 2-inactivation tumor suppressor genes. 3-loss of suppressor genes. Loss of genetic material on chromosome 911p(c- Ha-ras proto oncogene ) -17p.p53
 1-activation of oncogenes. 2-inactivation tumor suppressor genes. 3-loss of suppressor genes. Loss of genetic material on chromosome 911p(c- Ha-ras proto oncogene ) -17p.p53.")
4
Agent VIRUSES Chmical carcinogens. Physical stimuli.(X-ray.ultraviolet.stone

5
P 53 (1) 1-p53 is a suppressor gene loci on chromosome 17p. 2-this gene is the most frequently altered gene in human cancer. 3-the gene transcription factor that suppresses cell proliferation.repair of damaged DNA. 4-p53 mutation.genomic instability. 5-bladder cancer with p53 abnormalities is aggressive behaviors

6
P53 (2) 1-wild type p53 induces the expression of potent inhibitor of angiogenesis thrombospondin-1 (TSP-1 ) is extra cellular matrix.whereas mutant P53 absent or dose not. 2-p53 its under tight regulation. MDM2, whose expression by p53 and binds to p53 –N-terminal 3-wild type p53 only very briefly in the cell nucleus.whereas mutated accumulate and detected by immunohistchmistery.

7
Risk factors 1-Smoking.50%men and 31%women. 2-Occupational.15-35%men and 1-6% women workers in the chemical, dye, rubber,petroleum,leather printing industries. 3-ocuupational carcinogen Benzedrine, Betanaphthylamine,4-aminobiphenyl 4-cyclophosphamid. 5-Artificial sweeteners 6-Trauma -Infection,instrumentation -calculi

8
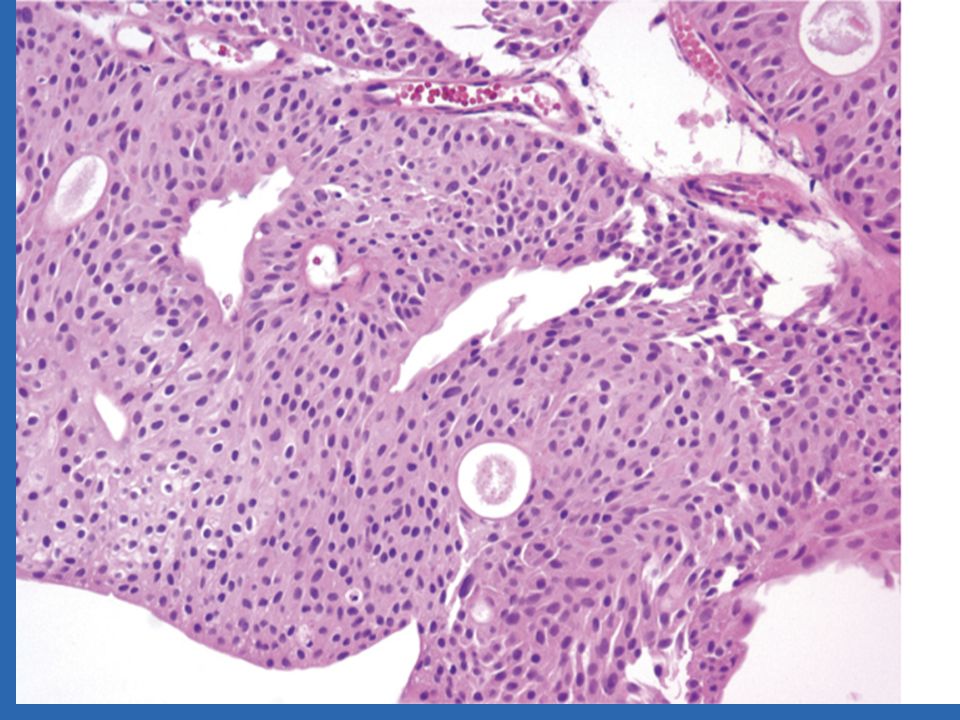
Histopathology. 1-90% of all bladder carcinoma TCC,s papillary, exophytic.sessile or ulcerated. 2-Carcinoma in situ (CI S ) flat ana plastic epithelium. 3-non TCC,s ACC <2% _SCC 5-10%all B.C 4-Undifferentiatd carcinoma <2% 5-Mixed carcinoma 4-6% (TCC-ACC-SCC- undi, 6-Rare epithelial carcinoma.villous adenoma, carcinoid tumor,carcinosarcumas,melanoma Pheochromocytoma lymphomas chriocarcinomas Sarcuma myosarcuma. Metastatic
 flat ana plastic epithelium. 3-non TCC,s ACC <2% _SCC 5-10%all B.C 4-Undifferentiatd carcinoma <2% 5-Mixed carcinoma 4-6% (TCC-ACC-SCC- undi, 6-Rare epithelial carcinoma.villous adenoma, carcinoid tumor,carcinosarcumas,melanoma Pheochromocytoma lymphomas chriocarcinomas Sarcuma myosarcuma. Metastatic.")
9
Clinical Finding A. Symptoms ; hematuria,85-90 % Vesical irritability,frequency,urgency,dysuria,Symptoms of advanced disease,bone pain flak pain. B Signs.bladder wall thickening (bimanual exm ) hepatomegaly,Supraclavicular node Lymph edema.
 hepatomegaly,Supraclavicular node Lymph edema..")
10
Laboratory Finding 1-urinalysis :hematuria,pyuria. 2-Azotemia,anemia 3-Urinary cytology,positive rate high in CIS. 4-tumor marker ; BTA (bladder tumor antigen). NMP22(nuclear matrix protein 22) Quanticyt system (Computer based cytology
. NMP22(nuclear matrix protein 22) Quanticyt system (Computer based cytology.")
12
Imaging Sonography IVP, ) CT.SCAN (w&wo contrast) 40-85% accuracy range, MRI (50-90%) A.R lymph node >1cm metastasis Chest x-ray.bone scan (alkaline phosphates' is high). Cystoscopy.

18
Staging (1) Ta papillary,epithelium confined Tis flat carcinoma in situ T1 Lamina propria invasion. T2a superficial propria invasion T2b deep muscularis propria invasion. T3a microscopic extention into perivesical fat. T3b macroscopic E.P F

19
Staging (2) T4a cancer invading pelvic viscera. T4b extention to pelvic sidewall abdoman wall / No no histologic pelvic node metastasis N1 single positive node < 2 cm below common iliacs N2 single positive node 2-5cm N3 positive node >5cm

20
Stage(3) M0 nodal status unknown M1 distant metastases documented Mx distant metastases status uncertain
 M0 nodal status unknown M1 distant metastases documented Mx distant metastases status uncertain")
21
Grading Grading system is now accepted ( 1up 3 ) Grade1 :minimal architectural abnormalities ;and nuclear atypical.papilllomas (recurrence- Not risk of progression, LOW grade. High grade

27
Treatment Tis complete TUR followed inra vesicle BCG. Ta (single low to moderate grate not recurrent) complete TUR. Ta (large multiple,high grate,or recurrent ). complete TUR +intra vesicles chemio -or immuno- T1 complete TUR +chimo -or immuno-(intra - ves. T2-T4 radical cystectomy or neoadjuvant chemio-+radical cystectomy.Radical cys -+ adju - chemio. neoadj -chemio-+chemio & Radio
 complete TUR. Ta (large multiple,high grate,or recurrent ). complete TUR +intra vesicles chemio -or immuno- T1 complete TUR +chimo -or immuno-(intra - ves. T2-T4 radical cystectomy or neoadjuvant chemio-+radical cystectomy.Radical cys -+ adju - chemio. neoadj -chemio-+chemio & Radio.")
28
Treatment(continue ) Any T,,N+ M+. Systemic chemotherapy followed by selective Surgery or Irradiation

29
Chemotherapy 15%of patient have regional or distant metastases and 30-40 % with invasive diseases Cisplatin ( single agent).30%responses Methotrexate,doxorubicin -vinblastine – cyclophosphamide –gemcitabine -5fu (MVAC)combination therapy the most commonly used for advanced bladder cancer
.30%responses Methotrexate,doxorubicin -vinblastine – cyclophosphamide –gemcitabine -5fu (MVAC)combination therapy the most commonly used for advanced bladder cancer")
30
Radiotherapy External beam irradiation (5000-7000 cGy-) in 5- 8 week. 5yearys survival rate for stage T2-T3 is 18- 40% and Recurrence is 33-68%

31
ureteral& renal pelvic cancer. Renal pelvis and ureteral cancer are rare.4% The ratio of bladder/real pelvis-ureter.51-3-1. M /F ratio is 2/4.2. Mean age 65 years. With upper tract carcinoma bladder CA-(30-50%) &conversely <2%). Contra lateral.upper tract (2-4%). AfterbladderCA &CA in situ and BCG therapy risk of development CA in upper tract 10%at5years and26% (5-10-yr )and 34% (>10yr )
 &conversely <2%). Contra lateral.upper tract (2-4%). AfterbladderCA &CA in situ and BCG therapy risk of development CA in upper tract 10%at5years and26% (5-10-yr )and 34% (>10yr ).")
32
Etiology As with bladder -CA smoking,industrial dyes or solvents. Excessive analgesic (acetaminophen –aspirin. caffeine – phenacetin (Balkan nephropathy ).
..")
33
Pathology. 90-97% is TCCs. Grading is similar of bladder CA. Papillomas (15-20%).and 50%have multiple papillomas. Most upper tract CA is localized and most common metastases site regional lymph node. Bone and lung. SCC :10% ACC is rare.mesodermal tumor is rare.metastases from stomach,prostate,kidney,breast and lymphoma
.and 50%have multiple papillomas. Most upper tract CA is localized and most common metastases site regional lymph node. Bone and lung. SCC :10% ACC is rare.mesodermal tumor is rare.metastases from stomach,prostate,kidney,breast and lymphoma.")
34
Staging. Ta,Tis confined to mucosa. 0 (Batata sys-) T1 invasion to lamina propria. A T2 invasion to muscularis. B T3 extension through muscularis. C in to fat or renal parenchyma T4. spread to adjacent organ. D N+ lymph node metastases. D M+ metastases D

35
Clinical Findings Gross hematuria (70-90%). Flank pain (8-50%). Voiding symptom (5-10%) Anorexia,weight loss, lethargy (metastases). Flank mass,tenderness. Supraclavicular node,inguinal node. Hepathomegaly
 Anorexia,weight loss, lethargy (metastases). Flank mass,tenderness. Supraclavicular node,inguinal node. Hepathomegaly.")
36
Laboratory& Imaging Hematuria, liver function test abnormality, Pyuria,bacteriuria.urincytology positive (30- 40%)low-grade and (60%) in high grade. IVP,retrograde pyelography.(goblet sign ) CT,urography (choice for evaluating the upper tract. Sonography – CT SCAN –MRI Ureteropyeloscopy
 CT,urography (choice for evaluating the upper tract. Sonography – CT SCAN –MRI Ureteropyeloscopy.")
37
treatment THE standard therapy is nephroureterectomy and excision of bladder cuff,(open or laparoscopic ). Distal ureterectomy &reimplantation, Endoscopic excision (recurrences 15-80%) and,maybe avoided by treatingwith BCG orChmiothrapy.(local) Radiotherapy. Systemic chemotherapy (cisplatin)
 and,maybe avoided by treatingwith BCG orChmiothrapy.(local) Radiotherapy. Systemic chemotherapy (cisplatin).")
Similar presentations