Download presentation
Presentation is loading. Please wait.

1
An Overview of Clinical Cancer Genetics
Mónica Alvarado, MS, CGC Certified Genetic Counselor Regional Administrator, Genetic Services Kaiser Permanente, Southern California

3
New cases in U.S. each year
Breast cancer: >185,000 Colorectal cancer: >150,000 Ovarian cancer: > 25,000 If 5% to 10% of these are due to hereditary cancer syndromes then…Each year between 18,000 to 36,000 newly diagnosed patients would be appropriate for referral to a cancer genetic counselor Reports indicate that only about 5% to 7% of patients who have a personal/family history of cancer suggestive of hereditary cancer are ever referred for genetic counseling.

4
GENETIC vs. INHERITED CANCER IS ALWAYS GENETIC BUT RARELY INHERITED

5
Cancer Arises From Gene Mutations
Germline mutations Somatic mutations Parent Child All cells affected in offspring Somatic mutation (eg, breast) Mutation in egg or sperm Occur in nongermline tissues Are nonheritable Present in egg or sperm Are heritable Cause cancer family syndromes
 Mutation in egg or sperm. Occur in nongermline tissues. Are nonheritable. Present in egg or sperm. Are heritable. Cause cancer family syndromes.")
6
When to Suspect Hereditary Cancer Syndrome
Cancer in 2 or more close relatives (on same side of family) Early age at diagnosis (< 45 yrs) Multiple primary tumors Bilateral or multiple rare cancers Constellation of tumors consistent with specific cancer syndrome (eg, breast and ovary, colon & endometrium) Evidence of autosomal dominant transmission Triple negative breast cancer plus any one of the above
 Early age at diagnosis (< 45 yrs) Multiple primary tumors. Bilateral or multiple rare cancers. Constellation of tumors consistent with specific cancer syndrome (eg, breast and ovary, colon & endometrium) Evidence of autosomal dominant transmission. Triple negative breast cancer plus any one of the above.")
7
Autosomal Dominant Inheritance
Each child has 50% chance of inheriting the mutation No “skipped generations” Equally transmitted by men and women Affected Normal

8
Syndrome Gene Cancers Hereditary Breast/Ovarian BRCA1 BRCA2
Breast, Ovarian, Pancreas, Others Lynch Syndrome/Hereditary Non-Polyposis Colorectal Cancer (HNPCC) MLH1 MSH2 MSH6 PMS2 Colorectal (CRC), Endometrial, Gastric, Ovarian, Other GI, Urinary tract Familial Adenomatous Polyposis (FAP) APC Colorectal, Duodenal, Thyroid, Brain
 MLH1 MSH2 MSH6. PMS2. Colorectal (CRC), Endometrial, Gastric, Ovarian, Other GI, Urinary tract. Familial Adenomatous Polyposis (FAP) APC. Colorectal, Duodenal, Thyroid, Brain.")
9
Colorectal Cancer: >150,000 cases annually in the US
Sporadic (~60%) Familial (~30%) Rare syndromes (~4%) FAP (<1%) HNPCC (3-5%) Slide 2 HNPCC: Autosomal Dominant Inheritance of Colorectal Cancer Risk Colorectal cancer (CRC) is the second leading cause of cancer death in the United States, with more than 130,000 cases diagnosed annually. In general, CRC is classified into three categories, based on increasing hereditary influence and cancer risk: Sporadic CRC comprises about 60% of cases. Patients with sporadic CRC do not have a notable family history of CRC nor do they have, by definition, an identifiable inherited gene mutation that accelerates cancer development. Familial CRC comprises up to 30% of cases and refers to patients who have at least one blood relative with CRC or an adenoma. However, no specific germline mutation or clear pattern of inheritance is identifiable. Familial CRC probably has multifactorial causes, such as shared exposure to carcinogens or interactions between the environment and multiple or weakly penetrant genes. Hereditary CRC syndromes account for approximately 10% of CRC. These autosomal dominant disorders confer the highest risk of colorectal cancer and result from inheritance of single gene mutations in highly penetrant cancer susceptibility genes. Hereditary nonpolyposis colorectal cancer (HNPCC) is the most common hereditary CRC syndrome, comprising about 3% to 5% of all CRCs. Familial adenomatous polyposis (FAP) is responsible for less than 1% of all CRC, while several rare disorders, such as Peutz-Jeghers syndrome and juvenile polyposis, make up the remaining small fraction. References Liu B, Parsons R, Papadopoulos N, et al. Analysis of mismatch repair genes in hereditary nonpolyposis colorectal cancer patients. Nature Medicine 1996;2: Ivanovich JL, Read TE, Ciske DJ. A practical approach to familial and hereditary colorectal cancer. American Journal of Medicine 1999;107:68-77. Nat Med 1996; 2:169-74
 Familial (~30%) Rare syndromes (~4%) FAP (<1%) HNPCC (3-5%) Slide 2. HNPCC: Autosomal Dominant Inheritance of Colorectal Cancer Risk. Colorectal cancer (CRC) is the second leading cause of cancer death in the United States, with more than 130,000 cases diagnosed annually. In general, CRC is classified into three categories, based on increasing hereditary influence and cancer risk: Sporadic CRC comprises about 60% of cases. Patients with sporadic CRC do not have a notable family history of CRC nor do they have, by definition, an identifiable inherited gene mutation that accelerates cancer development. Familial CRC comprises up to 30% of cases and refers to patients who have at least one blood relative with CRC or an adenoma. However, no specific germline mutation or clear pattern of inheritance is identifiable. Familial CRC probably has multifactorial causes, such as shared exposure to carcinogens or interactions between the environment and multiple or weakly penetrant genes. Hereditary CRC syndromes account for approximately 10% of CRC. These autosomal dominant disorders confer the highest risk of colorectal cancer and result from inheritance of single gene mutations in highly penetrant cancer susceptibility genes. Hereditary nonpolyposis colorectal cancer (HNPCC) is the most common hereditary CRC syndrome, comprising about 3% to 5% of all CRCs. Familial adenomatous polyposis (FAP) is responsible for less than 1% of all CRC, while several rare disorders, such as Peutz-Jeghers syndrome and juvenile polyposis, make up the remaining small fraction. References. Liu B, Parsons R, Papadopoulos N, et al. Analysis of mismatch repair genes in hereditary nonpolyposis colorectal cancer patients. Nature Medicine 1996;2: Ivanovich JL, Read TE, Ciske DJ. A practical approach to familial and hereditary colorectal cancer. American Journal of Medicine 1999;107: Nat Med 1996; 2:")
10
Familial Risk for Colorectal Cancer
70% Approximate lifetime CRC risk to age 70 yrs (%) 17% 10% 6% 8% 2% None One 1° One 1° and two 2° One 1° age <45 Two 1° HNPCC mutation Aarnio M et al. Int J Cancer 64:430, 1995 Houlston RS et al. Br Med J 301:366, 1990 St John DJ et al. Ann Intern Med 118:785, 1993 Affected family members 4
 17% 10% 6% 8% 2% None. One 1° One 1° and two 2° One 1° age <45. Two 1° HNPCC mutation. Aarnio M et al. Int J Cancer 64:430, Houlston RS et al. Br Med J 301:366, St John DJ et al. Ann Intern Med 118:785, Affected family members. 4.")
11
Lynch Syndrome (HNPCC)- About 3% of all Colorectal Cancer
Early (but variable) onset of CRC: Average age of onset of CRC is 45 years Defects in one of 4 mismatch repair genes: MLH1, MSH2, MSH6, PMS2 Tumors tend to be right sided 90% or more of CRC tumors exhibit microsatellite instability Muir-Torre syndrome is a variant of HNPCC associated with sebaceous adenomas
 onset of CRC: Average age of onset of CRC is 45 years. Defects in one of 4 mismatch repair genes: MLH1, MSH2, MSH6, PMS2. Tumors tend to be right sided. 90% or more of CRC tumors exhibit microsatellite instability. Muir-Torre syndrome is a variant of HNPCC associated with sebaceous adenomas.")
12
LS Increases the Risk of Colorectal Cancer
By age 50 By age 70 Slide 5 HNPCC Increases the Risk of Colorectal Cancer Without medical intervention, most people with inherited mutations in the MMR genes will develop colorectal cancer. The risk of colorectal cancer in mutation carriers is at least 25% by age 50 and about 80% by age 70. By comparison, the risk of colorectal cancer by age 70 in the general population is about 2%. Early onset of colorectal cancer is a hallmark of HNPCC. The average age of diagnosis of HNPCC-associated colorectal cancer is 45 years, and some patients develop the disease in their teens or twenties. It must be emphasized that although adenomatous polyps may form at a relatively early age in patients with HNPCC, a profusion of polyps is not a feature of HNPCC. HNPCC-associated colorectal cancers also appear to be biologically different from sporadic colorectal cancers. Compared with sporadic colorectal cancer, HNPCC-associated tumors most commonly develop in the right side of the colon, with nearly 70% found proximal to the splenic flexure. For this reason, endoscopic surveillance in HNPCC families should be performed with colonoscopy, not flexible sigmoidoscopy. Several studies also have reported better survival in HNPCC-associated colorectal cancer than sporadic colorectal cancer when matched for cancer stage. In addition, a particular DNA abnormality known as “microsatellite instability” is highly characteristic of HNPCC-associated colorectal cancers but occurs much less frequently in sporadic colorectal cancer. References Vasen HFA, Wijnen JT, Menko FH, et al. Cancer risk in families with hereditary nonpolyposis colorectal cancer diagnosed by mutation analysis. Gastroenterology 1996; 110: Aarnio M, Sankila R, Pukkala E, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. International Journal of Cancer 1999; 81:214-8. Population Risk 0.2% 2% LS Risk >25% 80% Gastroenterology 1996;110:1020-7 Int J Cancer 1999;81:214-8

13
LS Increases the Risk of Endometrial Cancer
By age 50 By age 70 Slide 6 HNPCC Increases the Risk of Endometrial Cancer Women who inherit HNPCC-associated germline mutations also have a greatly elevated risk of endometrial cancer. The risk of endometrial cancer in HNPCC is at least 20% by age 50 and up to 60% by age 70, compared with a less than 2% risk by age 70 in the general population. As with HNPCC-associated colorectal cancer, endometrial cancer in these patients occurs at an unusually young age, usually before age 50. Some studies have reported that if a woman carries an MLH1 or MSH2 mutation, her risk of endometrial cancer may be even higher than her risk of colorectal cancer. Early onset of endometrial cancer should therefore raise suspicion for HNPCC, especially in women with a family history of colorectal cancer or endometrial cancer. References Vasen HFA, Wijnen JT, Menko FH, et al. Cancer risk in families with hereditary nonpolyposis colorectal cancer diagnosed by mutation analysis. Gastroenterology 1996; 110: Aarnio M, Sankila R, Pukkala E, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. International Journal of Cancer 1999; 81:214-8. Population Risk 0.2% 1.5% LS Risk 20% 60% Gastroenterology 1996;110:1020-7 Int J Cancer 1999;81:214-8

14
The Family History Is Key to Diagnosing LS
CRC dx 50s CRC dx 45 CRC dx 61 CRC dx 75 Ovarian Ca, dx 64 CRC dx 48 CRC dx 52 Endometrial Ca, dx 59 45 CRC dx 42 32

15
LS: Clinical Characteristics of Colorectal Cancer
Early age of diagnosis mean age <45 yrs Predominantly proximal (right) colon cancer Improved survival Patients develop similar numbers of adenomas as the general population 3 or more relatives with verified CRC in family One case a first-degree relative of the other two Two or more generations One CRC by age 50 FAP excluded
 colon cancer. Improved survival. Patients develop similar numbers of adenomas as the general population. 3 or more relatives with verified CRC in family. One case a first-degree relative of the other two. Two or more generations. One CRC by age 50. FAP excluded.")
16
LS Cancer Risks Colorectal: Up to 80% lifetime risk
Endometrial: 30% to 60% lifetime risk Ovary: % by age 70 Stomach: % by age 70 Other Urinary tract (4% by age 70) Small intestine (100-fold relative risk, but < 5%) Biliary tract (2% by age 70) Brain (~4% by age 70) Slide 7 HNPCC Increases the Risks of Other Cancers HNPCC is also associated with an increased risk of cancers of the stomach and ovary, each estimated to be slightly higher than 10% by age 70. In addition, HNPCC also increases the risks of various rare cancers, including those of the urinary tract, small intestine and biliary tract, and brain, although each of these risks is usually below 5% during a person’s lifetime. Sebaceous skin tumors also occur in some patients and are a characteristic feature of a rare variant of HNPCC called Muir-Torre syndrome. References Vasen HFA, Wijnen JT, Menko FH, et al. Cancer risk in families with hereditary nonpolyposis colorectal cancer diagnosed by mutation analysis. Gastroenterology 1996; 110: Aarnio M, Sankila R, Pukkala E, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. International Journal of Cancer 1999; 81:214-8. Gastroenterology 1996;110: Int J Cancer 1999;81:214-8
 Small intestine (100-fold relative risk, but < 5%) Biliary tract (2% by age 70) Brain (~4% by age 70) Slide 7. HNPCC Increases the Risks of Other Cancers. HNPCC is also associated with an increased risk of cancers of the stomach and ovary, each estimated to be slightly higher than 10% by age 70. In addition, HNPCC also increases the risks of various rare cancers, including those of the urinary tract, small intestine and biliary tract, and brain, although each of these risks is usually below 5% during a person’s lifetime. Sebaceous skin tumors also occur in some patients and are a characteristic feature of a rare variant of HNPCC called Muir-Torre syndrome. References. Vasen HFA, Wijnen JT, Menko FH, et al. Cancer risk in families with hereditary nonpolyposis colorectal cancer diagnosed by mutation analysis. Gastroenterology 1996; 110: Aarnio M, Sankila R, Pukkala E, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. International Journal of Cancer 1999; 81: Gastroenterology 1996;110: Int J Cancer 1999;81:")
17
Management of LS

18
Colonoscopy Prevents Cancer in Mutation Carriers
Proportion free of CRC Surveillance 81.7% 100 57.8% No surveillance 80 60 40 5 10 15 Follow-up time (years) Gastroenterology 118:829, 2000
 Gastroenterology 118:829,")
19
Microsatellite Instability (MSI)
10% to 15% of sporadic tumors have MSI 95% of LS colon tumors have MSI Can be used as a screening test If colorectal tumor is MSI-H and family history is positive for CRC very high likelihood of LS

20
IHC tumor test for LS

21
IHC Test & Results Rationale for IHC tumor test
Universal IHC screening detects nearly twice as many cases of LS as targeting younger patients Cost effective can be internalized results point to which MMR genes to analyze Results 80% all proteins present Most likely not LS 20% one or more proteins absent Most will not have LS Approximately a third of these patients will test positive for a MMR mutation

22
2011 KPSC IHC Pilot Proposal
Surgery provide the “IHC fact sheet” to patients scheduled for CRC tumor surgery Pathology order reflex IHC testing on all CRC ≤ 50 yrs at diagnosis(~185 to 200 cases/yr) Immunohistochemistry lab performs IHC on tumor specimens per protocol sends all abnormal IHC tumor results (~20% of cases) to surgeon and local genetics contact Genetics Arranges follow-up of all abnormal IHC MMR results including: Contacts patient to offer genetics consultation as needed Coordinates follow-up tumor & germ line testing and appropriate counseling Dr. Tiller
 Immunohistochemistry lab. performs IHC on tumor specimens per protocol. sends all abnormal IHC tumor results (~20% of cases) to surgeon and local genetics contact. Genetics. Arranges follow-up of all abnormal IHC MMR results including: Contacts patient to offer genetics consultation as needed. Coordinates follow-up tumor & germ line testing and appropriate counseling. Dr. Tiller.")
23
Lynch Syndrome: Key Points
Most common form of hereditary CRC. Autosomal Dominant inheritance About 3% or colorectal and endometrial cancers Uterine/Endometrial cancer second most common after CRC in HNPCC families Family/Personal history and IHC and/or MSI can help identify affected individuals Identifying individuals with LS can minimize impact of disorder for them and their family members High risk of multiple primary CRC and extra-intestinal tumors Colonoscopic surveillance can improve survival in at-risk individuals For every individual identified with LS there are approx. 3 affected family members. Potential for preventing CRC in unaffected persons 45

24
Familial Adenomatous Polyposis (FAP)
About 1% of all CRC; Incidence 1 in 8,000 Multiple colonic adenomas (100s) beginning in childhood or teen years Autosomal dominant pattern of CRC: Average age of CRC is 36 Risk of CRC by age 40 nearly 100% Mutations in APC gene on 5q 80% are protein truncating mutations Up to 30% are new mutations
 beginning in childhood or teen years. Autosomal dominant pattern of CRC: Average age of CRC is 36. Risk of CRC by age 40 nearly 100% Mutations in APC gene on 5q. 80% are protein truncating mutations. Up to 30% are new mutations.")
25
Family with FAP Colon CA dx. 47 Age 45 FAP, dx. 27 Colectomy
CRC dx. 31, d. 35 Age 42 FAP dx.38 APC+ Colectomy Age 40 APC - Age 18 APC+ FAP dx. 15 Surveillance

26
Clinical Features of FAP
Estimated penetrance for adenomas >90% Risk of extracolonic tumors (upper GI, desmoid, osteoma, thyroid, brain, other) CHRPE may be present Untreated polyposis leads to 100% risk of cancer 6
 CHRPE may be present. Untreated polyposis leads to 100% risk of cancer. 6.")
27
Other Cancers Associated with FAP
Cancer Risk Lifetime Risk Duodenal & periampullary cancer % Thyroid cancer % Pancreatic cancer % Hepatoblastoma (childhood) % Gastric cancer % CNS tumors <1 % Burt, Gastroenterology 2000; 119:837-53
 2 % Gastric cancer 0.5 % CNS tumors <1 % Burt, Gastroenterology 2000; 119:")
28
Gardner’s Syndrome: A Variant of FAP
Features of FAP plus extraintestinal lesions: Epidermoid cyst Desmoid tumors Osteomas Dental abnormalities CHRPE Soft tissue skin tumors Jaw osteoma 12

29
Medical Management of FAP
Annual flexible sigmoidoscopy beginning at age 101 Prophylactic total colectomy after polyp detection chemoprevention: celecoxib after surgery2 NSAIDs (eg., sulindac) after surgery (investigational) Subsequent surveillance for rectal and extracolonic tumors 1Gastroenterology 2001; 121:197-7 2Steinbach, NEJM 2000; 342:
 after surgery (investigational) Subsequent surveillance for rectal and extracolonic tumors. 1Gastroenterology 2001; 121: Steinbach, NEJM 2000; 342:")
30
FAP: Key Points Autosomal dominant with early onset of polyposis
However, up to 30% new mutations (no family hx) Severe polyposis makes it easier to identify affected individuals CRC risk is 100% in untreated patients Genetic testing identifies most APC mutation carriers Endoscopic surveillance and colectomy can significantly improve survival Noncarriers can avoid anxiety and unnecessary tests Genetic testing of children has medical benefit
 Severe polyposis makes it easier to identify affected individuals. CRC risk is 100% in untreated patients. Genetic testing identifies most APC mutation carriers. Endoscopic surveillance and colectomy can significantly improve survival. Noncarriers can avoid anxiety and unnecessary tests. Genetic testing of children has medical benefit.")
32
Tumor Suppressor Genes
Normal genes (prevent cancer) 1st mutation (susceptible carrier) 2nd mutation or loss (leads to cancer)
 1st mutation. (susceptible carrier) 2nd mutation or loss (leads to cancer)")
33
BRCA1 Approximately 1 in 500 women may be carriers of alterations in BRCA1 Breast tumors tend to be triple negative (ER, PR and Her2Neu negative), basal type, excess of medullary Ovarian tumors: epithelial, high grade, mucinous and borderline tumors rare Specific alterations observed in ~1% Ashkenazi Jewish individuals: 185delAG, 5382insC
, basal type, excess of medullary. Ovarian tumors: epithelial, high grade, mucinous and borderline tumors rare. Specific alterations observed in ~1% Ashkenazi Jewish individuals: 185delAG, 5382insC.")
34
BRCA2 Gene is twice the size of BRCA1
Breast tumors tend to be ER +, and no specific histopathology observed Ovarian tumors: epithelial, high grade, mucinous and borderline tumors rare Wider spectrum of cancer types Specific alteration in 1.5% of Ashkenazi Jewish individuals: 6174delT

35
BRCA1 and BRCA2 in Ashkenazi Jewish Individuals
1 in 40 will have mutation in BRCA1/2 regardless of family history Founder effect: 3 mutations account for the majority of carriers Ashkenazi Jewish heritage must be identified for proper risk assessment and mutation analysis

36
The BRCA1 and 2 Genes

37
BRCA1 & BRCA2-Associated Cancers: Lifetime Risk
ASCO Curriculum: Cancer Genetics & Cancer Predisposition Testing BRCA1 & BRCA2-Associated Cancers: Lifetime Risk breast cancer (often < 50 yrs) 40%-85% Contralateral breast cancer 40-60% ovarian cancer 10%-40% male breast cancer elevated (6%) Pancreas & prostate cancers may also be elevated Breast and Ovarian Cancer 10
 40%-85% Contralateral breast cancer % ovarian cancer. 10%-40% male breast cancer elevated (6%) Pancreas & prostate cancers. may also be elevated. Breast and Ovarian Cancer. 10.")
38
BRCA1/2 Mutations Increase Risk of Breast and Ovarian Cancer
By age By age By age 70 Slide 5 HNPCC Increases the Risk of Colorectal Cancer Without medical intervention, most people with inherited mutations in the MMR genes will develop colorectal cancer. The risk of colorectal cancer in mutation carriers is at least 25% by age 50 and about 80% by age 70. By comparison, the risk of colorectal cancer by age 70 in the general population is about 2%. Early onset of colorectal cancer is a hallmark of HNPCC. The average age of diagnosis of HNPCC-associated colorectal cancer is 45 years, and some patients develop the disease in their teens or twenties. It must be emphasized that although adenomatous polyps may form at a relatively early age in patients with HNPCC, a profusion of polyps is not a feature of HNPCC. HNPCC-associated colorectal cancers also appear to be biologically different from sporadic colorectal cancers. Compared with sporadic colorectal cancer, HNPCC-associated tumors most commonly develop in the right side of the colon, with nearly 70% found proximal to the splenic flexure. For this reason, endoscopic surveillance in HNPCC families should be performed with colonoscopy, not flexible sigmoidoscopy. Several studies also have reported better survival in HNPCC-associated colorectal cancer than sporadic colorectal cancer when matched for cancer stage. In addition, a particular DNA abnormality known as “microsatellite instability” is highly characteristic of HNPCC-associated colorectal cancers but occurs much less frequently in sporadic colorectal cancer. References Vasen HFA, Wijnen JT, Menko FH, et al. Cancer risk in families with hereditary nonpolyposis colorectal cancer diagnosed by mutation analysis. Gastroenterology 1996; 110: Aarnio M, Sankila R, Pukkala E, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. International Journal of Cancer 1999; 81:214-8. Breast Cancer Population Risk <0.5% ~2% ~7% BRCA Carrier Risk 2 - 3% % 40-85% Ovarian Cancer <<<1% <1% 1% <<1% 2 - 20% %

39
Identification of women at high risk for HBOC
Family History & Presentation Two or more cases of breast and/or ovarian cancer on same side of the family Consider both sides of the family, ethnicity Ashkenazi Jewish heritage Early age of onset, multiple primaries, TNBC Breast cancer <45 yrs at diagnosis Breast & ovarian cancer in the same woman, multiple breast primaries TNBC: ER, PR and Her2 negative (BRCA1) Autosomal dominant pattern of cancer
 Autosomal dominant pattern of cancer.")
40
Management of BRCA Mutation Positive Patient
BRCA1 or BRCA2 Mutation Offer test to relatives Lifestyle Changes Increased Surveillance Chemo- prevention Prophylactic Surgery Adapted from Myriad Genetics

41
BRCA Carriers: Cancer Screening
Breast cancer screening Monthly BSE from age 18 Clinical breast exam 2-4 times per year (beginning at age 25) Annual mammography and MRI starting at age 25 or individualized based on earliest age of onset in family MRI is most sensitive imaging modality for surveillance of BRCA carriers. 80% to 92% MRI vs 23% to 33% Mammo (based on 4 studies, N=714) Ovarian cancer screening Concurrent TVU, Pelvic exam and CA125 q6 months starting at age 35 or 5-10 years earlier than earliest onset in family No proven benefit
 Annual mammography and MRI starting at age 25 or individualized based on earliest age of onset in family. MRI is most sensitive imaging modality for surveillance of BRCA carriers. 80% to 92% MRI vs 23% to 33% Mammo (based on 4 studies, N=714) Ovarian cancer screening. Concurrent TVU, Pelvic exam and CA125 q6 months starting at age 35 or 5-10 years earlier than earliest onset in family. No proven benefit.")
42
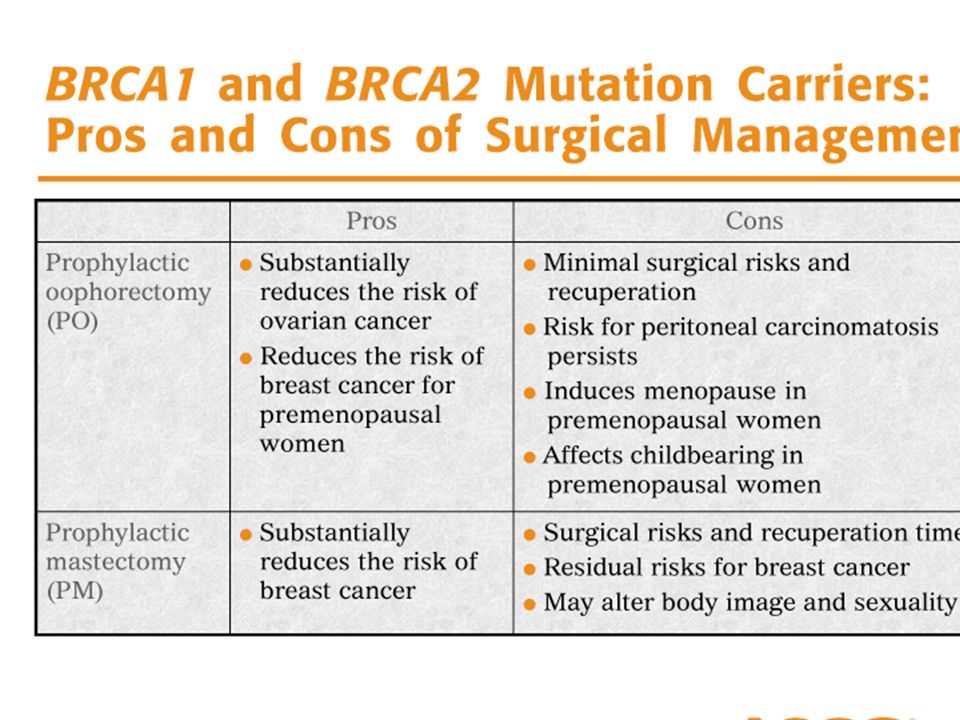
Prophylactic Surgery in BRCA1/2 carriers
Prophylactic mastectomy Reduces risk by ~90% Total (simple) mastectomy recommended Nipple sparing mastectomy may be good alternative Risk-reducing salpingo-oopherectomy Reduces risk by 85%-95% or more Must remove ovaries and tubes; hysterectomy currently optional in most centers Peritoneal washings recommended due to high incidence of occult malignancy Breast cancer risk reduction 55-70% if done pre-menopausally Does not eliminate risk for primary peritoneal cancer Residual risk reported as 1% to 4.3%
 mastectomy recommended. Nipple sparing mastectomy may be good alternative. Risk-reducing salpingo-oopherectomy. Reduces risk by 85%-95% or more. Must remove ovaries and tubes; hysterectomy currently optional in most centers. Peritoneal washings recommended due to high incidence of occult malignancy. Breast cancer risk reduction % if done pre-menopausally. Does not eliminate risk for primary peritoneal cancer. Residual risk reported as 1% to 4.3%")
44
Chemoprevention for BRCA1/2 Carriers
Breast Cancer Tamoxifen & Raloxifene: Very little data on carriers; few choose it Tamoxifen may be less effective in BRCA1 carriers One case control study reported ~50% contralateral cancer risk reduction from Tamoxifen use in BRCA1/2 carriers No evidence that Tamoxifen post BSO reduces breast cancer risk Ovarian Cancer Oral Contraceptives reduce risk by 50% to 70% with 5 yr use Data unclear: two large studies reached opposite conclusions on effects of OCs in ovarian cancer risk for BRCA1/2 carriers Use should be evaluated on case by case basis Narod et al, Lancet, 2000

45
BRCA Carriers: Timing can influence decision making
How might a newly diagnosed breast cancer patient alter her treatment decisions? Surgery? Chemotherapy? How might her future cancer risk for cancer influence these decisions? Second breast cancer? Ovarian cancer? d. 59 Breast CA dx. 54 73 Breast CA dx. 60 d. 53 Breast CA dx. 42 49 Breast CA BRCA2 +

46
Could this be HBOC? How does Ashkenazi Jewish background affect probability of mutation in BRCA1 & 2? Non Ash.: 1.1%-5.6% Ash. Jewish: 8.2%-15.6% How might cousin’s TAH/BSO affect family history of breast and ovarian cancer in this family? Polish/Hungarian Jewish Unk CA d. 52 d.70s d. 53 Ovarian CA dx. 51 d 45

47
HBOC: Key Points Clues in the personal or family history of cancer can help identify individuals who may have an inherited susceptibility to breast or ovarian cancer Mutations in BRCA1/2: Can be passed down from the mother or father Are far more frequent in Ashkenazi Jewish families Are inherited in autosomal dominant fashion Genetic testing is offered only when personal and/or family history of cancer suggests inherited susceptibility Genetic testing can identify mutations in BRCA1/2 and influence risk management, and save lives

48
Cancer Genetics Resources
FORCE:Facing Our Risk of Cancer Empowered; support group for BRCA1/2 Cancer Genetics Services Directory: Johns Hopkins Digestive Disease Library: CDC Colorectal Cancer: Genetics of Cancer:

Similar presentations