Download presentation
Presentation is loading. Please wait.

1
بسم الله الرحمن الرحیم

3
Randomised, controlled trial Population Sample Outcome Experimental intervention Control intervention Randomisation Time

4
scales and their modifications including: Jadad Maastricht Delphi List PEDro Maastricht-Amsterdam List (MAL) Van Tulder Bizzini Chalmers Reisch Andrew Imperiale Detsky Cho and Bero Balas Sindhu Downs and Black Nguyen Oxford Pain ValidityScale (OPVS) Arrive´ CONSORT Yates
 Van Tulder Bizzini Chalmers Reisch Andrew Imperiale Detsky Cho and Bero Balas Sindhu Downs and Black Nguyen Oxford Pain ValidityScale (OPVS) Arrive´ CONSORT Yates")
5
http://www.consort-statement.org/ http://www.consort-statement.org/

6
In 1993, 30 experts comprised of medical journal editors, clinical trialists, epidemiologists, and methodologists met in Ottawa, Canada with the aim of developing a new scale to assess the quality of randomized controlled trial (RCT) reports One outcome of the meeting was the Standardized Reporting of Trials (SORT) statement.This statement consisted of a 32-item checklist and flow diagram in which investigators were encouraged to report on the various aspects of how RCTs were conducted.
 reports One outcome of the meeting was the Standardized Reporting of Trials (SORT) statement.This statement consisted of a 32-item checklist and flow diagram in which investigators were encouraged to report on the various aspects of how RCTs were conducted.")
7
Concurrently, and independently, another group of experts, the Asilomar Working Group on Recommendations for Reporting of Clinical Trials in the Biomedical Literature, convened in Asilomar (California), USA, were working on a similar mandate At the suggestion of Drummond Rennie, Deputy Editor of JAMA, representatives from both groups met in 1996, in Chicago, USA.. The meeting resulted in the Consolidated Standards of Reporting Trials (CONSORT) Statement, which was first published in 1996
 Statement, which was first published in")
8
PRISMA for systematic reviews of randomized trials; MOOSE for systematic reviews of observational studies; STARD for diagnostic accuracy studies; REMARK for tumor marker prognostic studies; TREND for non- randomized evaluations of behavioural and public health interventions; STROBE for observational studies.PRISMAMOOSESTARDREMARKTREND STROBE

9
Consolidated Standards of Reporting Trials, encompasses various initiatives developed by the CONSORT Group to alleviate the problems arising from inadequate reporting of randomized controlled trials (RCTs).
.")
10
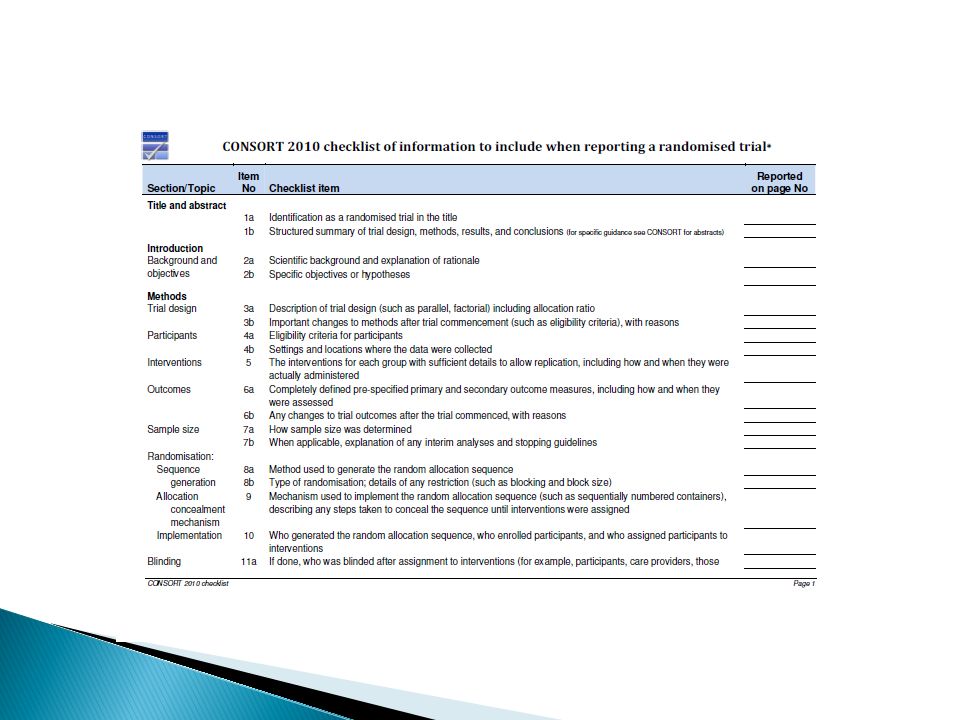
The CONSORT Statement comprises a 25-item checklist and a flow diagram, along with some brief descriptive text. The checklist items focus on reporting how the trial was designed, analyzed, and interpreted; the flow diagram displays the progress of all participants through the trial. checklistflow diagram

14
Item 1a - Identification as a randomised trial in the title. Item 1b - Structured summary of trial design, methods, results, and conclusions Item 1a - Identification as a randomised trial in the title. Item 1b - Structured summary of trial design, methods, results, and conclusions To help ensure that a study is appropriately indexed and easily identified, authors should use the word “randomised” in the title to indicate that the participants were randomly assigned to their comparison groups

16
Item 2a - Scientific background and explanation of rationale Item 2b - Specific objectives or hypotheses

17
Trial Design :Item 3a - Description of trial design (such as parallel, factorial) including allocation ratio Changes to trial design: Item 3b - Important changes to methods after trial commencement (such as eligibility criteria), with reasons Participants: Item 4a - Eligibility criteria for participants Study settings: Item 4b - Settings and locations where the data were collected
 including allocation ratio Changes to trial design: Item 3b - Important changes to methods after trial commencement (such as eligibility criteria), with reasons Participants: Item 4a - Eligibility criteria for participants Study settings: Item 4b - Settings and locations where the data were collected")
18
Item 5 - The interventions for each group with sufficient details to allow replication, including how and when they were actually administered

19
Item 6a - Completely defined pre-specified primary and secondary outcome measures, including how and when they were assessed Changes to outcomes :Item 6b - Any changes to trial outcomes after the trial commenced, with reasons Item 6a - Completely defined pre-specified primary and secondary outcome measures, including how and when they were assessed Changes to outcomes :Item 6b - Any changes to trial outcomes after the trial commenced, with reasons

20
Item 7a - How sample size was determined Interim analyses and stopping guidelines :Item 7b - When applicable, explanation of any interim analyses and stopping guidelines Item 7a - How sample size was determined Interim analyses and stopping guidelines :Item 7b - When applicable, explanation of any interim analyses and stopping guidelines

21
sequence generation Item 8a - Method used to generate the random allocation sequence Randomization: type Item 8b - Type of randomisation; details of any restriction (such as blocking and block size) sequence generation Item 8a - Method used to generate the random allocation sequence Randomization: type Item 8b - Type of randomisation; details of any restriction (such as blocking and block size)
 sequence generation Item 8a - Method used to generate the random allocation sequence Randomization: type Item 8b - Type of randomisation; details of any restriction (such as blocking and block size)")
22
Item 9 - Mechanism used to implement the random allocation sequence (such as sequentially numbered containers), describing any steps taken to conceal the sequence until interventions were assigned Item 10 - Who generated the allocation sequence, who enrolled participants, and who assigned participants to interventions Item 9 - Mechanism used to implement the random allocation sequence (such as sequentially numbered containers), describing any steps taken to conceal the sequence until interventions were assigned Item 10 - Who generated the allocation sequence, who enrolled participants, and who assigned participants to interventions
, describing any steps taken to conceal the sequence until interventions were assigned Item 10 - Who generated the allocation sequence, who enrolled participants, and who assigned participants to interventions Item 9 - Mechanism used to implement the random allocation sequence (such as sequentially numbered containers), describing any steps taken to conceal the sequence until interventions were assigned Item 10 - Who generated the allocation sequence, who enrolled participants, and who assigned participants to interventions")
23
Item 11a - If done, who was blinded after assignment to interventions (for example, participants, care providers, those assessing outcomes) and how
 and how")
24
Participants Providers Raters/data collectors Data analysts

25
The term “blinding” or “masking” refers to withholding information about the assigned interventions from people involved in the trial who may potentially be influenced by this knowledge. Blinding is an important safeguard against bias, particularly when assessing subjective outcomes

26
Item 11b - If relevant, description of the similarity of interventions

27
Item 12a - Statistical methods used to compare groups for primary and secondary outcomes Additional analyses: Item 12b - Methods for additional analyses, such as subgroup analyses and adjusted analyses Item 12a - Statistical methods used to compare groups for primary and secondary outcomes Additional analyses: Item 12b - Methods for additional analyses, such as subgroup analyses and adjusted analyses

28
A diagram is strongly recommended. Item 13a - For each group, the numbers of participants who were randomly assigned, received intended treatment, and were analyzed for the primary outcome A diagram is strongly recommended. Item 13a - For each group, the numbers of participants who were randomly assigned, received intended treatment, and were analyzed for the primary outcome

32
Item 13b - For each group, losses and exclusions after randomisation, together with reasons

33
Item 14a - Dates defining the periods of recruitment and follow-up Reason for stopped trial : Item 14b - Why the trial ended or was stopped

34
Item 15 - A table showing baseline demographic and clinical characteristics for each group

35
Item 16 - For each group, number of participants (denominator) included in each analysis and whether the analysis was by original assigned groups
 included in each analysis and whether the analysis was by original assigned groups")
36
Item 17a - For each primary and secondary outcome, results for each group, and the estimated effect size and its precision (such as 95% confidence interval)
")
37
Item 17b - For binary outcomes, presentation of both absolute and relative effect sizes is recommended

38
Item 18 - Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing pre- specified from exploratory

39
Item 19 - All important harms or unintended effects in each group

40
Item 20 - Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of analyses

41
( 1 ) a brief synopsis of the key findings, ( 2 ) consideration of possible mechanisms and explanations, (3) comparison with relevant findings from other published studies
 a brief synopsis of the key findings, ( 2 ) consideration of possible mechanisms and explanations, (3) comparison with relevant findings from other published studies")
42
(4) limitations of the present study (and methods used to minimise and compensate for those limitations) (5) a brief section that summarises the clinical and research implications of the work, as appropriate
 limitations of the present study (and methods used to minimise and compensate for those limitations) (5) a brief section that summarises the clinical and research implications of the work, as appropriate")
43
Although discussion of limitations is frequently omitted from research reports, identification and discussion of the weaknesses of a study have particular importance

44
Item 21 - Generalisability (external validity, applicability) of the trial findings
 of the trial findings")
45
Is my patient similar to the study population? Is the treatment feasible in my clinical setting? Will potential benefits of treatment outweigh potential harms of treatment for my patient?

46
Item 22 - Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence

47
Item 23 - Registration number and name of trial registry

48
Item 24 - Where the full trial protocol can be accessed, if available

49
Item 25 - Sources of funding and other support (such as supply of drugs), role of funders
, role of funders")
50
همتم بدرقه راه کن ای طایر قدس که درازست ره مقصد و من نو سفرم ای نسیم سحری بندگی من برسان که فراموش مکن وقت دعای سحرم

Similar presentations











 www.ahrq.gov.>")














