Download presentation
Presentation is loading. Please wait.

1
EUprimecare: Quality and Costs of Primary Care in Europe September 2012, Gothenburg (Sweden) European Forum Primary Care Grant Agreement no. 241595 Dr. Antonio Sarría-Santamera (ISCIII) Sonia García (ISCIII) Eleonora Corsalini (UB)
 Sonia García (ISCIII) Eleonora Corsalini (UB).")
2
The goals of any healthcare system: Deliver effective, safe, quality personal and non-personal health interventions to those that need them, when and where needed, with minimum waste of resources AccessCostsQuality Background

3
The Tallin Charter Strengthening of health systems to improve people's health but keeping equity. Primary Care Basic structure of health system Eliminating health disparities Background

4
Common framework to describe Primary Care models in the EU is not available Not yet developed a trans-national consensus on how to define quality of Primary Care Cost of Primary Care are not well identified in national accounting systems Background

5
Objectives

6
Institute of Health Carlos III. ISCIII. Spain Universität Bielefeld. UNIBI. Germany University of Tartu. UTartu. Estonia National Institute for Strategic Health Research. ESKI. Hungary Országos Alapellátási Intezet. OALI. Hungary Institute for health and Welfare. THL. Finland Kaunas University of Medicine. KMU. Lithuania Universitá Commerciale Luigi Bocconi. UB. Italy Partners

7
Conceptual structure Identify a methodology to measure the PC quality WP 5 & 6 Identify a methodology to measure costs in PC WP 3 & 4 WP 7 WP2 Evaluation of PC models COORDINATION WP 1 DISSMINATION WP 8 To measure the health quality in PC To measure costs in PC ORGANIZATION OF PRIMARY CARE IN EUROPE REGULATIONFINANCINGPAYMENTORGANIZATION ORGANIZATIONAL BEHAVIOUR

8
Approach

9
Work package 2: Evaluation of PC models in Europe Work package 2: Evaluation of PC models in Europe Methodological Approach of a Classification System of PC Models in Europe : Germany, Spain, Estonia, Finland, Hungary, Italia and Lithuania.

10
WP2: Methodology 1.Literature review Structure or process of PC in Europe Control knobs: financing, regulation, payment, organization, and organizational behavior 2.Selection of indicators => template design: 1.5 variables (Control knobs) to optimize healthcare systems results: 2.Range of services 3.Descriptive Analysis & Principal Component Analysis
 to optimize healthcare systems results: 2.Range of services 3.Descriptive Analysis & Principal Component Analysis")
11
FINANCING Mixed model (Hungary) BISMARCK SS (Estonia, Germany, Lithuania) BEVERIDGE NHS (Finland, Italy, Spain) 7% Uninsured 10,6% Private Insurance 18,8% Double coverage Expenditure in HC as GDP 10,5% 6,1%6,6% 24% Expenditure in PC 5,7% 16% Double coverage Descriptive analysis (I)
 BISMARCK SS (Estonia, Germany, Lithuania) BEVERIDGE NHS (Finland, Italy, Spain) 7% Uninsured 10,6% Private Insurance 18,8% Double coverage Expenditure in HC as GDP 10,5% 6,1%6,6% 24% Expenditure in PC 5,7% 16% Double coverage Descriptive analysis (I)")
12
Formal mechanisms to guarantee accessibility, equity and quality of healthcare Gate-keeping systems, except in Germany Facilities: Mostly public: Finland, Spain, Hungary and Lithuania Totally private: Germany, Estonia and Italy Clinical practice: Integrated network: Finland and Spain Solo and group practices: Germany, Estonia, Italy, Lithuania, Hungary REGULATION ORGANIZATION Descriptive analysis (II)
")
13
Process to monitoring and improving the quality of medical practice: Quality management systems measuring clinical and no clinical quality indicators Clinical practices guidelines Continuing education ORGANIZATIONAL BEHAVIOUR Descriptive analysis (III)
")
14
Provision of services through national/regional/local health systems (Yes/No) Private voluntary health insurance (Yes/No) Geographical distribution of PC services (Yes/No) Professional income (Capitation/Salary/Fee for service/Out of pocket) Gatekeeping for specialist (Yes/No) Type of facilities (Public/private) Type of clinical practice (Solo practice/Group practice/ Network) Improvement programs & Quality management systems (Yes/No) Continuing clinical education program (Yes/No) Local adaptation of clinical practice guideline (Yes/No) Financing Regulation Organization Payment Organizational behavior Quantitative analysis (PCA)
 Private voluntary health insurance (Yes/No) Geographical distribution of PC services (Yes/No) Professional income (Capitation/Salary/Fee for service/Out of pocket) Gatekeeping for specialist (Yes/No) Type of facilities (Public/private) Type of clinical practice (Solo practice/Group practice/ Network) Improvement programs & Quality management systems (Yes/No) Continuing clinical education program (Yes/No) Local adaptation of clinical practice guideline (Yes/No) Financing Regulation Organization Payment Organizational behavior Quantitative analysis (PCA)")
15
Range of services

16
Results of Qualitative analysis Based on a functional perspective, allowed to proposing 5 models: 1.Direct access to specialist 2.Referral required from GP, mainly solo-practices in PC 3.Referral required from GP, mainly group-practices in PC 4.Health care centers 5.Polyclinics Based on a functional perspective, allowed to proposing 5 functional models: Model 1: Direct access to any GP or specialist (Germany) Model 2: Referral required from GP, mainly solo-practices in PC (Hungary, Italy) Model 3: Referral required from GP, mainly group-practices in PC (Estonia, Lithuania) Model 4: GPs working mainly in health care centres (Finland, Spain) Model 5: Polyclinics (Shemasko). Not necessarily GPs at all Results

19
* *Predominance

22
Framework for classification of health systems based on PC Multidimensional => more complex => more realistic Healthcare services provision Basic coverage Gate-keeping Private insurances Professional payment Type of facilities Type of practice Conclusions

23
Work package 3&4: Costs of Primary Care Systems

24
Methodology Micro-costing

25
Methodology Macro-costing Actual costs: Real not estimated Usual accounting principles and practices Indicated in the estimated overall budget

26
Work package 5&6: Quality of Primary Care Systems

27
Focus Group Discussion : Patients (n= 53) Primary care professionals (n= 64) 7 countries: Estonia, Finland, Germany, Hungary, Italy, Lithuania, Spain. Helped to understand the views about quality in the different partner countries and to set a list of quality criteria. Non-clinical indicators for each criteria were identified from the literature review and prioritized by scoring according to importance and measurability. Methodology Quality Indicators

29
Methodology Quality at the Population Level

30
Methodology Quality at the Clinical Level

32
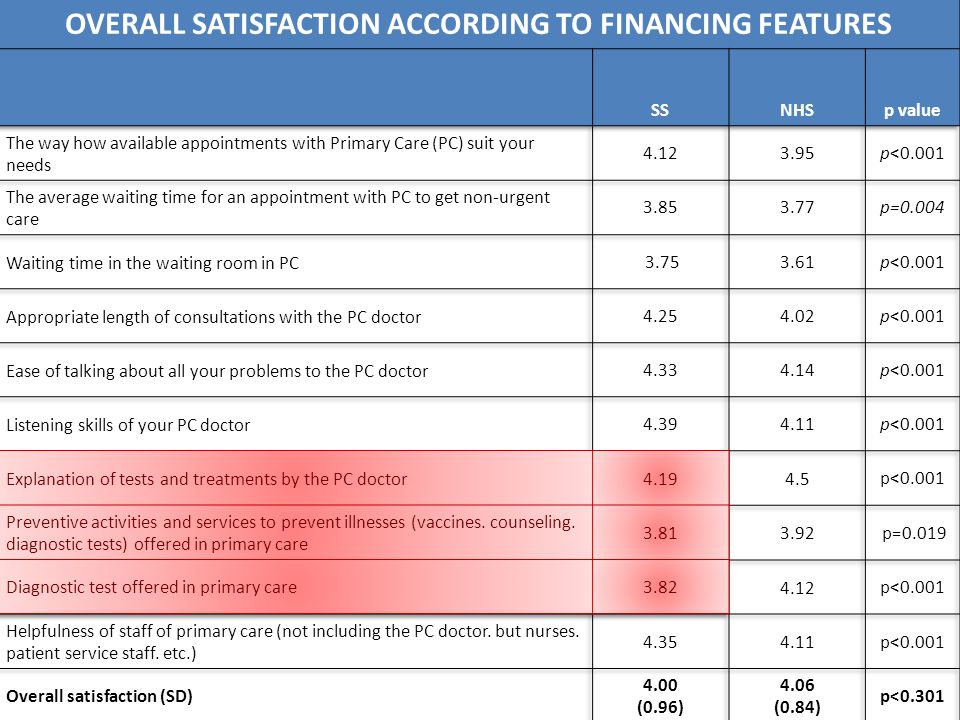
Work package 5&6: Quality Population survey- Satisfaction Results Work package 5&6: Quality Population survey- Satisfaction Results

36
Mean=4.03

37
OVERALL SATISFACTION WITH THE ATTENTION PROVIDED BY PC SERVICES (%)
")
39
Mean=4.03

46
Work package 7:Trade offs between PC Models, Quality and PC expenditure

47
PERCENTAGE OF PATIENTS DIAGNOSED BY THEIR PC DOCTORS ACCORDING TO FINANCING FEATURES

48
PERCENTAGE OF PATIENTS WHO ARE DIAGNOSED BY THEIR PC DOCTOR ACCORDING TO ORGANIZATIONAL FEATURES

49
FRECUENCY OF PREVENTION AND COUNSELING ACTIVITIES ACCORDING TO FINANCING FEATURES <1year <1-2year >2year

50
FRECUENCY OF PREVENTION AND COUNSELING ACTIVITIES ACCORDING TO ORGANIZATIONAL FEATURES <1year <1-2year >2year

51
SELF-PERCEIVED HEALTH STATUS ACCORDING TO FINANCING FEATURES

52
SELF-PERCEIVED HEALTH STATUS ACCORDING TO ORGANIZATIONAL FEATURES

53
UTILIZATION ACCORDING TO FINANCING FEATURES

54
UTILIZATION ACCORDING TO ORGANIZATIONAL FEATURES

55
PERCENTAGE OF PATIENTS WHO ARE DIAGNOSED BY THEIR PC DOCTOR ACCORDING TO LEVEL OF EXPENDITURE

56
FRECUENCY OF PREVENTION AND COUNSELING ACTIVITIES ACCORDING TO LEVEL OF EXPENDITURE <1year <1-2year >2year

57
SELF-PERCEIVED HEALTH STATUS ACCORDING TO LEVEL OF EXPENDITURE

58
UTILIZATION ACCORDING TO EXPENDITURE LEVEL

59
Final remarks

60
The use of clinical vignettes in costing primary care services in 7 EU countries 3 rd September 2012, EFPC Conference - Gothenburg E. Corsalini, G. Fattore, A. Compagni

61
Overall task To identify a methodology for cost measurement in primary care services and to apply it. Challenging goal: extreme variability in terms of professionals involved, payment mechanisms, services provided across countries impossible to develop a one-fits-all method, but need to provide a common and defined framework

62
Chosen Method Clinical Vignettes= description of a common clinical situation, followed by a synthetic questionnaire to be submitted to professionals solve the problem of the interpretation of identical questions are a common denominator in a context of extreme heterogeneity allow to describe how a certain clinical case is managed in primary care and to estimate all the resources consumed in the delivery

63
STEPS 1.To choose the vignettes 2.To translate the vignettes 3.To validate the vignettes 4.To submit the vignettes to primary care professionals 5.To collect questionnaires 6.To measure resources consumption in the delivery of services involved in the clinical vignettes

64
1. Choice of vignettes Criteria taken into account: Main areas of primary care systems: - Disease prevention area - Care of acute but common problems - Care of chronic conditions - Health promotion services Primary care activities/services common to all the partners of the consortium

65
Vignettes V1: A 70-year-old man in good health comes to the practice asking to be vaccinated against the seasonal influenza V2: A 2-year-old boy comes to the practice with his mother. The day before the boy had developed cough with nasal discharge and had fever up to 38,2°C. The parent has noted a rattling sound in the child's chest. […] He has mild expiratory dyspnea. His breathing rate is 36 times per minute. […] He has atopic dermatitis but otherwise has been healthy.

66
Vignettes V3: There is a 65-year-old woman among your patients, who has been diagnosed with type 2 diabetes. She comes in for a follow-up visit: the tests from last week show that her HbA1c is 7%. She has no complications. She has been taking metformin 500 mg x2. You are her main primary care provider for the next 12 months. V4: A young woman, aged 35, comes to the practice to get a certificate of “good health” for practicing a sport. She is in good health, she does sports, she has a good and satisfying job, she does not drink, nor uses drugs. But, upon you enquiring, she reveals that she has been smoking 20 cigarettes per day for the last 10 years.

67
STEPS 1.To choose the vignettes 2.To translate the vignettes 3.To validate the vignettes 4.To submit the vignettes to primary care professionals 5.To collect questionnaires 6.To measure resources consumption in the delivery of services involved in the clinical vignettes

68
4. Submission of vignettes Vignettes have been submitted: personally, by interviewers from each country to a group of professionals of the same kind (e.g., a group of GPs, a group of paediatricians, a group of nurses): the number of the members for each group was 20-30 and different vignettes have been submitted to the same group through a written questionnaire: professionals of each group have been requested to answer the questions related to each vignette in writing
: the number of the members for each group was and different vignettes have been submitted to the same group through a written questionnaire: professionals of each group have been requested to answer the questions related to each vignette in writing.")
69
4. Submission of vignettes In total, more than 200 professionals have been interviewed.

70
STEPS 1.To choose the vignettes 2.To translate the vignettes 3.To validate the vignettes 4.To submit the vignettes to primary care professionals 5.To collect questionnaires 6.To measure resources consumption in the delivery of services involved in the clinical vignettes

71
6. To measure resources consumption Data collected through questionnaires by each partner have been put together and synthesized in four different databases, specific per each vignette/questionnaire, by the Bocconi University team This last part of the exercise had two different purposes: - to measure resources consumption in the delivery of certain primary care activities to which monetary values could be attributed; - to collect data/information useful to carry out an analysis of variation of how the same case is managed within and between countries

72
6. To measure resources consumption Measuring resource consumption Methodology: Time-Driven Activity-Based-Costing = it is a particular development of the better known Activity-Based Costing (ABC) that allows to design cost models in very complex contexts, such as service organizations The TDABC requires two parameters: the time required to provide/perform the activity the unit cost of supplying capacity
 that allows to design cost models in very complex contexts, such as service organizations The TDABC requires two parameters: the time required to provide/perform the activity the unit cost of supplying capacity.")
73
6. To measure resources consumption: data collected Each vignette was structured as to gather information about: 1.medical and administrative professionals directly involved in the service; 2.the amount of time spent in the activity by the professionals involved; 3.medical material directly used in the provision of the service; 4.medical material and other health care services consumed as a consequence of the service; 5.other medical professionals involved as a consequence of the service described in the vignette.

74
6. To measure resources consumption: data collected Moreover, for each vignette, partner countries have provided: cost of the professionals directly involved; cost of administrative staff involved; cost of the medical material directly used; cost of the medical material and other health care services consumed as a consequence of the service; cost of other medical professionals involved as a consequence of the service; direct cost paid by patients for the provision of the service; estimation of overheads costs.

75
SOME RESULTS FROM THE VIGNETTES

76
V2 – A sick 2-year-old boy: Professionals involved CountryTotal casesPaediatrician General PhysicianNurseSecretary Other PC professional Hungary52100,00% 50,00%28,85%30,77% Italy23100,00% 8,70%21,74%0,00% Finland39 100,00%66,67%33,33%10,26% Lithuania30 100,00%60,00%10,00% Estonia23 100,00%69,57%8,70%17,39% Spain21100,00% 47,62%9,52%0,00% Germany23100,00% 0,00%86,96%0,00% All countries211100,00%46,45%28,44%12,80%

77
V2 – A sick 2-year-old boy: Time spent in the visit HungaryItalyFinlandLithuaniaEstoniaSpainGermany Paediat./General Physician Average time per case 13,916,313,815,714,713,412,7 Nurse Average time per case 3,30,76,35,34,06,20,0 Other PC professional Average time per case 2,50,00,80,40,70,0 Total time per case 19,817,020,921,419,319,612,7

78
V2 – A sick 2-year-old boy: Time - variability within countries HungaryItalyFinlandLithuaniaEstoniaSpainGermany Paediat./General Physician Min51011165 Max303830 204030 ST.DEV.6,645,925,825,975,487,705,90 Average time per patient13,8816,3513,8515,6714,6513,3812,65

79
V2 – A sick 2-year-old boy: Clinical behaviors HungaryItalyFinlandLithuaniaEstoniaSpainGermany All countries Pharmacological Treatment94,23%95,65%87,18%76,67%65,22%100,00%95,65%88,15% Categories of drugs Fever reducer24,49%54,55%5,88%26,09%0,00%42,86%9,09%23,12% Bronchodilator81,63%50,00%97,06%73,91%80,00%85,71%100,00%82,26% Antibiotics18,37%36,36%2,94%21,74%20,00%4,76%0,00%14,52% Anti-inflammatory10,20%36,36%0,00%4,35%0,00% 7,53% HungaryItalyFinlandLithuaniaEstoniaSpainGermanyAll countries Diagnostic tests38,46%30,43%46,15%50,00%82,61%0,00%26,09%40,28% Specialist involved40,38%8,70%64,10%23,33%17,39%4,76%0,00%28,44%

80
V2 – A sick 2-year-old boy: Micro-costing HungaryItalyFinlandLithuaniaEstoniaSpainGermany Paediat./General Physician € 3,86 € 26,83 € 14,13 € 4,17 € 5,05 € 16,24 € 59,51 Nurse € 0,74 € 0,27 € 3,01 € 0,79 € 0,58 € 5,34 Secretary € 0,55 € 0,67 € 0,45 € 0,02 € 0,06 € 0,04 Assistant/Trainee € 0,70 € - € 0,61 € 0,03 € 0,09 € - TOTAL LABOUR COST € 5,86 € 27,78 € 18,20 € 5,01 € 5,78 € 21,62 € 59,51 DRUGS COST € 8,47 € 11,83 € 9,28 € 5,11 € 3,59 € 4,66 € 13,07 TESTS COST € 3,40 € 4,71 € 2,92 € 4,29 € 4,52 € - € 16,03 OUT-OF-POCKET € - TOTAL COST € 17,72 € 44,32 € 30,39 € 14,41 € 13,88 € 26,27 € 88,62 Hourly cost

81
Some costs data: Labour cost (in PPP) HungaryItalyFinlandLithuaniaEstoniaSpain General Physician average cost in PPP per year € 18.818 € 115.354 € 64.617 € 18.549 € 23.106 € 84.675 Paediatrician average cost in PPP per year € 18.818 € 129.910 N.A. € 72.148 Nurse average cost in PPP per year € 12.255 € 37.827 € 34.185 € 14.287 € 14.144 € 51.423 Secretary average cost in PPP per year € 4.821 € 29.098 € 27.676 € 7.811 € 7.180 € 22.972 Assistant/Trainee average cost in PPP per year € 9.720 € 92.601 N.A € 7.811 € 14.144 N.A

82
Thank you

Similar presentations




















 European Forum Primary Care Grant Agreement no. 241595 Dr.>")

 Dr. Erika.>")



 Stefan.>")







