Download presentation
Presentation is loading. Please wait.

1
ABDOMEN & PELVIS PATHOLOGY & SCANNING PROTOCOLS

2
PATHOLOGIES

3
ABDOMINAL MESENTERIC CYST

4
ABDOMINAL CYST An abdominal CT scan revealed a large right upper quadrant cyst measuring 14x17x21 cm ( lateral, anteroposterior and craniocaudal)There was mass effect upon the liver and duodenum. The cyst had a thin smooth wall with internal fluid and high density material consistent with a blood clot.
There was mass effect upon the liver and duodenum. The cyst had a thin smooth wall with internal fluid and high density material consistent with a blood clot.")
5
RENAL CYST NO CONTRAST CONTRAST
RENAL CYST NO CONTRAST CONTRAST They appear as well-defined, thin-walled, round or oval masses, with attenuation close or equal to that of water (0-20 HU).
.")
6
POLYCYSTIC KIDNEY DISEASE
In PKD fluid-filled cysts develop giving the kidneys a honeycomb appearance. It is one of the most common inherited disorders, and the fourth commonest cause of kidney failure. In polycystic kidney disease many fluid-filled cysts develop in the kidneys. Gradually these cysts replace the normal kidney tissue enlarging the kidneys but making them less and less able to function normally. Eventually the kidneys fail completely

7
HEPATOMEGALY

8
STEATOSIS

9
Hepatocellular carcinoma: The most common primary malignant neoplasm of the liver. HCC typically appears hypodense on non-contrast scans and hyperdense or hypervascular on arterial phase imaging

10
ASCITES Ascites is the abnormal collection of fluid in the abdominal cavity, most often as a result of chronic liver disease.

11
SPLENOMEGALY

12
SPLENIC INFARCTION

13
APPENDICITS An axial slice of a CT scan done with the use of intravenous and oral contrast is presented. The arrow points to an area of soft tissue induration within the retrocecal fat. There is a rim like area of higher attenuation within this area. The structure is fluid filled. These features are compatible with a diagnosis of acute appendicitis and the presence of rupture cannot be excluded.

14
DIVERTICULITS Diverticulitis is inflammation or infection of small pouches, called diverticula, that develop along the walls of your intestines. The formation of the pouches themselves is a relatively benign condition known as diverticulosis. The pouches can develop anywhere on the digestive tract, but they most commonly form at the end of the descending and sigmoid colons, and they also frequently occur on the first section of the small intestine (although they rarely cause problems there).
.")
15
DIVERTICULITS

16
ABDOMINAL ABSCESS Psoas abscess (blue arrow), and abscess dissecting anteriorly in transversalis fascia.
, and abscess dissecting anteriorly in transversalis fascia.")
17
BOWEL OBSTRUCTION

18
LIVER METS Lung cancer, small cell. Contrast-enhanced CT scan of the abdomen. Axial section through the liver shows multiple hypoattenuating areas in the liver. Poorly defined margins, attenuation greater than that of water, and scattered distribution in a patient with known lung cancer is most consistent with metastatic disease.

19
ESOPHAGEAL CANCER

20
WILMS TUMOR Wilms tumor, also called nephroblastoma, is a cancer that originates in the kidney. The disease gets its name from a German doctor, Max Wilms, who wrote one of the first medical articles about it in 1899. Ninety percent of all kidney cancers in children are Wilms tumor. The remaining ten percent are rare forms of childhood kidney cancers: clear cell sarcoma of the kidney, malignant rhabdoid tumor of the kidney, and occasionally renal cell carcinoma

21
WILMS TUMOR

22
ADRENAL METS

23
RENAL STONE

24
HYDRONEPHROSIS

25
BLADDER CANCER

26
KIDNEY CANCER Kidney cancer affects some 30,000 people in the United States each year, and close to 12,000 die from the disease. It is the eighth most common cancer in men and the tenth most common in women. Smoking is the major risk factor,

27
HORSESHOE KIDNEYS

28
PHEOCHROMOCYTOMA Pheochromocytoma is a tumor of the adrenal gland that causes excess release of epinephrine and norepinephrine, hormones that regulate heart rate and blood pressure

29
CIRRHOSIS

30
HEMANGIOMA

31
A cavernous hepatic hemangioma is the most common non-cancerous tumor of the liver. It is believed to be a congenital defect, and is usually not discovered until medical pictures are taken of the liver for some other reason.

32
CHOLELITHIASIS

33
CHOLECYSTITIS

34
PANCREATIC CANCER

35
PANCREATITIS

36
ABDOMINAL ANEURYSM

37
PROTOCOLS

38
Exam Preparation When possible, patients fast for 2 to 6 hours before the examination. Fasting results in an empty proximal GI tract, facilitating its evaluation and also limiting the potential hazard of aspiration of stomach contents in the event of GI upset due to IV administration of a contrast agent. 2. In most cases, an oral contrast agent is administered to distend the GI tract and clearly demonstrate the intestinal lumen. The agent used may be a dilute solution of an iodinated contrast medium, barium sulfate, or water. For general studies of the abdomen and pelvis, 750 to 1500 mL of oral contrast agent is administered 30 to 120 minutes before the exam. 3. Example protocol for oral contrast agent administration is: a. 450 mL given 90 to 120 minutes before the exam for opacification of the distal intestines. b. 300 to 450 mL given 30 minutes before the exam for opacification of the proximal intestines. c. An additional volume of 150 to 250 mL given just before scanning for opacification of the stomach and duodenum.

39
Administration of Intravenous Contrast Agents
1. When not contraindicated, the administration of an iodinated IV contrast agent improves the quality of abdominal and pelvic CT imaging by: a.Enhancing, or increasing the CT density of, abdominal organ parenchyma. b.Increasing the detectability of lesions from normal structures. c.Opacifying vascular structures. d.Providing assessment of organ perfusion and function. 2. There are also clinical indications for non-contrast or pre- and post-contrast imaging, including: a.Characterizing the enhancement pattern of a lesion. b.Evaluation of calcifications within organ parenchyma. c.Assessment of unenhanced parenchymal attenuation values. d.Identification of calculi within the bile ducts, gallbladder, urinary tract, and appendix

40
Contrast agent dose ranges from approximately 50 to 150 mL
Contrast agent dose ranges from approximately 50 to 150 mL. The total dose depends on the patient's condition and the clinical indication for the study. Injection rates vary between 2.0 and 5.0 mL/sec. The rate selected depends on the enhancement phase(s) to be acquired and the capacity of the venous access. The delay between the initiation of contrast agent administration and scanning is tailored to the required phase of enhancement and coordinated with the injection rate.
 to be acquired and the capacity of the venous access. The delay between the initiation of contrast agent administration and scanning is tailored to the required phase of enhancement and coordinated with the injection rate.")
41
FEET FIRST OR HEAD FIRST
SPONGE

42
ABDOMEN STANDARD ROUTINE SCOUT: AP LANDMARK: XIPHOID TIP
SCAN MODE: Spiral I.V. CONTRAST: ml/sec, ML SCAN DELAY: sec ORAL CONTRAST: 400 ml 45 MINUTES BEFORE SCAN, 200 ML JUST BEFORE SCAN BREATH HOLD: SUSPENDED EXPIRATION SLICE THICKNESS: MM START LOCATION: LUNG BASES END LOCATION: ILIAC CREST FILMING: STANDARD, LUNGS, LIVER + BONE FOR TRAUMA & CANCER ROUTINE

43
ABDOMEN-KIDNEY STONE SCOUT: AP LANDMARK: XIPHOID TIP SCAN MODE: Spiral
NO ORAL CONTRAST NO IV CONTRAST BREATH HOLD: SUSPENDED EXPIRATION SLICE THICKNESS: 5MM START LOCATION: ABOVE KIDNEYS END LOCATION: S. PUBIS FILMING: STANDARD

44
ABDOMEN LIVER MASS-3 PHASE
SCOUT: AP LANDMARK: XIPHOID TIP SCAN MODE: SPIRAL I.V. CONTRAST: 4-5 ml/sec, ML SCAN DELAY: 1. NON-CONTRAST, 2. ARTERIAL 30 SEC. 3. PORTAL 70 SEC. ORAL CONTRAST: 400 ml 45 MINUTES BEFORE SCAN, 200 ML JUST BEFORE SCAN BREATH HOLD: SUSPENDED EXPIRATION SLICE THICKNESS: 4-5 MM START LOCATION: LUNG BASES END LOCATION: ILIAC CREST FILMING: STANDARD + LIVER

45
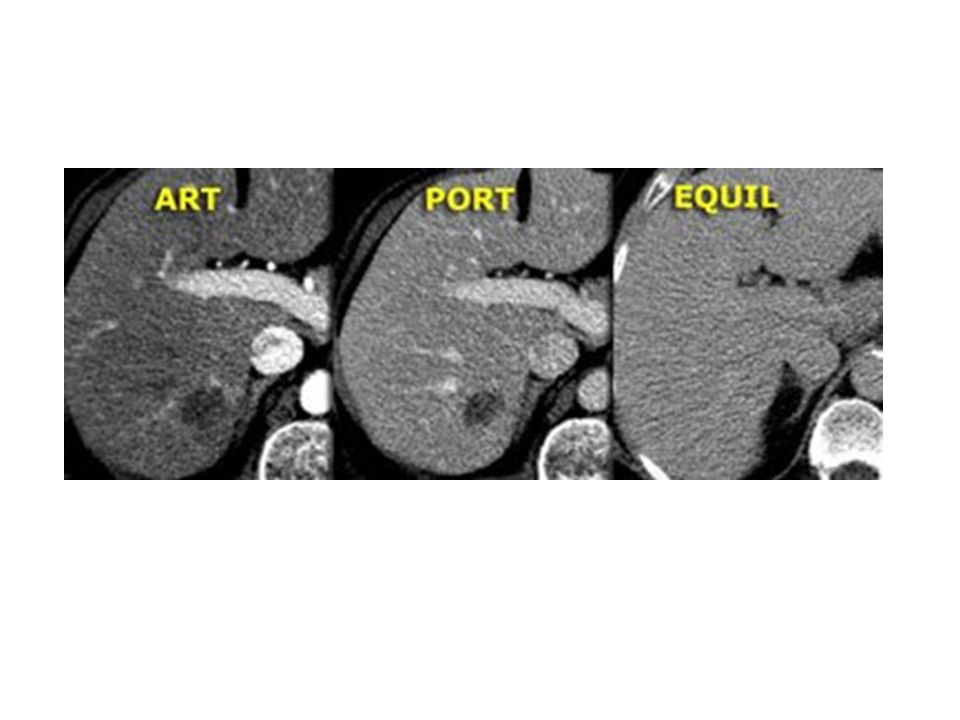
Arterial phase: The period of peak arterial enhancement typically occurs at 25 to 35 seconds after the initiation of contrast agent administration. During this phase, hypervascular tumors, or tumors supplied by the hepatic artery, undergo maximal enhancement. The lesions are made conspicuous by the relatively unenhanced hepatic parenchyma surrounding them. Portal (or hepatic) venous phase: The period of peak hepatic parenchymal enhancement during which contrast material redistributes from the blood into the extravascular spaces. Typically occurring at 60 to 70 seconds after the initiation of contrast agent administration, this is the phase during which hypovascular lesions are most conspicuous owing to their density difference from the enhancing hepatic parenchyma. Equilibrium phase: Usually occurs at 2 to 3 minutes after the initiation of contrast agent administration. During this phase, hepatic parenchymal enhancement dissipates, and there is minimal difference in contrast enhancement between the intravascular and extravascular spaces. Many hepatic lesions become indistinguishable from their surroundings. The rapid acquisition made possible by MDCT helps avoid scanning during this phase.
 venous phase: The period of peak hepatic parenchymal enhancement during which contrast material redistributes from the blood into the extravascular spaces. Typically occurring at 60 to 70 seconds after the initiation of contrast agent administration, this is the phase during which hypovascular lesions are most conspicuous owing to their density difference from the enhancing hepatic parenchyma. Equilibrium phase: Usually occurs at 2 to 3 minutes after the initiation of contrast agent administration. During this phase, hepatic parenchymal enhancement dissipates, and there is minimal difference in contrast enhancement between the intravascular and extravascular spaces. Many hepatic lesions become indistinguishable from their surroundings. The rapid acquisition made possible by MDCT helps avoid scanning during this phase.")
46
NON-CONTRAST ARTERIAL PORTAL

48
The delayed phase of hepatic data acquisition occurs approximately 5 to 20 minutes after contrast agent administration. This phase is used primarily to demonstrate the complete “fill-in” of a hemangioma as it becomes isodense with surrounding parenchyma.

49
The CT density of the unenhanced spleen is between +40 and +60 HU, which is approximately 10 HU less than that of the unenhanced liver. The spleen is optimally imaged after administration of a contrast agent. On arterial phase imaging, the spleen demonstrates a heterogeneous enhancement pattern. The preferred timing for CT acquisition of the spleen is the portal venous phase (60-70 seconds), when a more homogeneous pattern of enhancement is demonstrated.
, when a more homogeneous pattern of enhancement is demonstrated.")
50
Most pancreatic tumors appear hypodense in comparison with surrounding contrast-enhanced pancreatic parenchyma. Imaging the pancreas during the phase of peak parenchymal enhancement vastly increases the conspicuity of most pancreatic neoplasms. The pancreatic phase of contrast enhancement is a delayed arterial phase occurring approximately 35 to 45 seconds after the start of contrast agent administration, assuming that an adequate volume is injected at a rate of 3 mL/sec or higher.

51
ABDOMEN- PANCREAS SCOUT: AP LANDMARK: XIPHOID TIP
SCANNING MODE: SPIRAL I.V. CONTRAST: ml/sec SCAN DELAY: Arterial 25 sec, delayed arterial sec, venous sec ORAL CONTRAST: 400 ml 45 MINUTES BEFORE SCAN, 200 ml 15 MINUTES BEFORE SCAN BREATH HOLD: SUSPENDED EXPIRATION SLICE THICKNESS: 3-5 MM THROUGH PANCREAS START LOCATION: LUNG BASES END LOCATION: ILIAC CREST FILMING: STANDARD + LIVER + BONE FOR TRAUMA & CANCER

52
The primary goal of multiphasic CT evaluation of a pancreatic mass is the determination of tumor resectability.

53
BETTER VISUALIZATION OF PANCREAS- R. LAT. DECUB.

54
ABDOMEN- KIDNEYS SCOUT: AP LANDMARK: XIPHOID TIP SCANNING MODE: SPIRAL
I.V. CONTRAST: 2-4 ml/sec SCAN DELAY:1. NONCONTRAST: 2. ARTERIAL 30 SEC. 3. NEPHROGRAM 90 SEC.: 4. EXCRETORY 3-5 MIN. ORAL CONTRAST: 400 ml 45 MINUTES BEFORE SCAN, 200 ml JUST BEFORE SCAN BREATH HOLD: SUSPENDED EXPIRATION SLICE THICKNESS: MM , 5 MM THROUGH KIDNEYS START LOCATION: LUNG BASES END LOCATION: ILIAC CREST FILMING: STANDARD

55
Corticomedullary phase: A late arterial phase beginning 30 to 40 seconds after the initiation of contrast agent administration. Optimal enhancement of the renal cortex and renal veins occurs during this period. The renal medulla is minimally enhanced, allowing for its maximum differentiation from the renal cortex.

56
Nephrographic phase: Time between 70 and 90 seconds after the start of injection. Enhancement differences between renal cortex and medulla reach equilibrium, providing optimal sensitivity for parenchymal lesions. Imaging during the nephrographic phase also allows for portal opacification and optimal hepatic enhancement, which are important for the assessment of disease spread.

57
Excretory phase: A delayed imaging phase that begins approximately 3 minutes after the initiation of contrast agent administration. During this phase, the contrast agent has been excreted into the renal calyces, opacifying the renal pelvis and the remainder of the urinary collecting system (ureters, bladder). The excretory phase best demonstrates the filling defects and the potential lesions involving the urothelium.
. The excretory phase best demonstrates the filling defects and the potential lesions involving the urothelium..")
59
Simple cysts: Smooth, round, thin-walled masses with homogeneous near-water CT density (<20 HU).
An angiomyolipoma of the kidney is a benign mass of blood vessels (angio-), muscle tissue (myo-), and fat (lipoma). An ROI measurement of less than −10 HU characterizes a renal mass as an angiomyolipoma. Renal cell carcinoma (RCC): The most common primary renal malignancy. RCC is typically characterized by marked contrast enhancement (>20-25 HU).
, muscle tissue (myo-), and fat (lipoma). An ROI measurement of less than −10 HU characterizes a renal mass as an angiomyolipoma. Renal cell carcinoma (RCC): The most common primary renal malignancy. RCC is typically characterized by marked contrast enhancement (>20-25 HU).")
60
< -10

61
Transitional cell carcinoma (TCC): A tumor originating in the urothelium. Most TCCs arise in the bladder, with the possibility of additional masses in the ureters, renal pelvis, or both. On pre-contrast imaging, TCC usually appears as a hypodense lesion within the renal collecting system that has a CT density greater than that of urine but less than that of renal parenchyma (<40 HU). TCC significantly enhances after administration of a contrast agent. Metastases: Lung, colon, and breast cancers are primary malignancies that commonly result in renal metastases.
. TCC significantly enhances after administration of a contrast agent. Metastases: Lung, colon, and breast cancers are primary malignancies that commonly result in renal metastases.")
62
The majority of focal adrenal masses are benign adenomas.
Differentiation between a metastatic lesion and a benign adenoma is an important goal of the CT evaluation of an adrenal mass: a.On pre-contrast imaging, ROI measurements of a mass that are less than 10 HU indicate a benign process. b.On delayed post-contrast imaging, metastatic lesions of the adrenal gland remain enhanced longer than adrenal adenomas. c.The extent of the dissipation of enhancement, or “washout” can be calculated during delayed (10-15 minutes) imaging of the adrenal glands.
 imaging of the adrenal glands.")
63
CTA OF THE ABDOMEN SCOUT: AP LANDMARK: XIPHOID TIP SCAN MODE: Spiral
I.V. CONTRAST: 4-5 ml/sec, ML SCAN DELAY: 25 sec BREATH HOLD: SUSPENDED EXPIRATION SLICE THICKNESS: 3 MM START LOCATION: ABOVE AORTIC ARCH END LOCATION: BELOW ILIAC CREST FILMING: STANDARD + 3D + MPR

64
ABDOMEN + PELVIS APPENDICITIS OR DIVERTICULITIS
SCOUT: AP LANDMARK: XIPHOID TIP SCAN MODE: Spiral I.V. CONTRAST: ml/sec, ML SCAN DELAY: sec ORAL CONTRAST: 500 cc MINUTES BEFORE SCAN, 200 ML JUST BEFORE SCAN BREATH HOLD: SUSPENDED EXPIRATION SLICE THICKNESS: 8 MM + 3-5MM LOWER START LOCATION: LUNG BASES END LOCATION: S.PUBIS FILMING: STANDARD SCOUT: AP LANDMARK: XIPHOID TIP SCAN MODE: Spiral I.V. CONTRAST: ml/sec, ML SCAN DELAY: sec ORAL CONTRAST: 400 ml 45 MINUTES BEFORE SCAN, 200 ML JUST BEFORE SCAN BREATH HOLD: SUSPENDED EXPIRATION SLICE THICKNESS: MM UPPER + 5 MM LOWER START LOCATION: LUNG BASES END LOCATION: S. PUBIS FILMING: STANDARD 8 MM 5 MM

65
CTA ABDOMEN

66
CT COLONOSCOPY 2 SCANS- PRONE + SUPINE

67
PELVIS SCOUT: AP LANDMARK: ILIAC CREST SLICE PLANE: AXIAL OR SPIRAL
I.V. CONTRAST: ml/sec, ml SCAN DELAY: sec (FULL BLADDER) ORAL CONTRAST: ml 1-2 HOURS BEFORE SCAN 500 cc NIGHT BEFORE BREATH HOLD: SUSPENDED EXPIRATION SLICE THICKNESS: MM, 3-5 MM IF AP OR DIVERTICULITIS START LOCATION: ILIAC CREST END LOCATION: SYMPHYSIS PUBIS FILMING: STANDARD
 ORAL CONTRAST: ml 1-2 HOURS BEFORE SCAN. 500 cc NIGHT BEFORE. BREATH HOLD: SUSPENDED EXPIRATION. SLICE THICKNESS: 8-10 MM, 3-5 MM IF AP OR DIVERTICULITIS. START LOCATION: ILIAC CREST. END LOCATION: SYMPHYSIS PUBIS. FILMING: STANDARD.")
68
DETECTION OF PROSTATE GLAND AND SEMINAL VESICLES ABNORMALITIES
BLADDER OPACIFIED + RECTOSIGMOID COLON AND RECTUM OPACIFIED

70
VISUALIZATION OF VAGINAL CANAL + CERVIX AND UTERUS
TAMPON INSERTED IN THE VAGINA DURING CT SCAN OF THE PELVIS

Similar presentations





 and the portal vein ( 75% of vascularization).>")


 می فرمایند : بسم الله الرحمن الرحیم.>")













