Download presentation
Presentation is loading. Please wait.

1
Pharmacologic Principles Chapter 2
Catherine Luksic BSN, RN Level I

2
Pharmacology DRUG PHARMACOLOGY
Any chemical that affects the physiologic processes of a living organism PHARMACOLOGY Study (science) of drugs Includes: Absorption Distribution Metabolism Excretion Mechanism of Action Therapeutic effects Adverse effects Metabolism of drug = biochemical modification
 of drugs. Includes: Absorption. Distribution. Metabolism. Excretion. Mechanism of Action. Therapeutic effects. Adverse effects. Metabolism of drug = biochemical modification.")
3
Pharmacology Subspecialty Areas of Pharmacology Pharmaceutics
Pharmacokinetics Pharmacodynamics Pharmacotherapeutics Pharmacognosy Toxicology NURSES MUST UNDERSTAND BASIC PRINCIPLES OF PHARMACOLOGY Therapeutic and Toxic SAFETY !

4
Pharmacology – Drug development
Drugs will acquire 3 names CHEMICAL (N-4 hydroxyphenyl acetamide) Drugs chemical composition, molecular structure GENERIC (acetaminophen) Shorter than chemical name Used as official listing of drugs TRADE (Tylenol) Registered trademark, “brand” name Name is restricted to “owner” (company, ie, Merck) **Patent lasts 17 years - 10 years for research and development - 7 years of marketability
 Drugs chemical composition, molecular structure. GENERIC (acetaminophen) Shorter than chemical name. Used as official listing of drugs. TRADE (Tylenol) Registered trademark, brand name. Name is restricted to owner (company, ie, Merck) **Patent lasts 17 years years for research and development. - 7 years of marketability.")
5
Pharmacology – Drug Development

6
Pharmaceutics Process of turning chemicals into safe medications
Science of dosage form & design ie – tablet, capsule, liquid, powder, etc. Study of how various dosage forms/designs influence a drugs metabolism and use in the body Design that will allow drug molecules to bind to a target site

7
pharmaceutics Drug routes Oral Enteral Rectal Parenteral Topical
Via mouth Includes sublingual, buccal Enteral Via intestine Via NG tube, feeding tube (or rectal) Rectal Parenteral Intramuscular, Subcutaneous, Intravenous, Topical Directly applied to skin Mucosal
 Rectal. Parenteral. Intramuscular, Subcutaneous, Intravenous, Topical. Directly applied to skin. Mucosal.")
8
Pharmaceutics **Forms/designs of drugs: Oral Enteral Rectal Parenteral
Tablets, capsules, powder, liquid, elixir, suspension EC, ER, SR Enteral Meds given via NG or feeding tube (solid or liquid) Crushed meds – must be dissolved Rectal Suppositories, creams, enema Also considered as ENTERAL route Parenteral Injections (solutions, powder)
 Crushed meds – must be dissolved. Rectal. Suppositories, creams, enema. Also considered as ENTERAL route. Parenteral. Injections (solutions, powder)")
9
Pharmaceutics Topical Mucosal Inhaled
Ointments, creams, pastes, powders, patches Mucosal eye, ear, nasal, vaginal Inhaled

10
Pharmaceutics Drug Dissolution & Absorption
**Drugs must dissolve 1st (before absorbed) Oral Preparations Liquids, elixirs, syrups Fastest Suspension solutions ê Powders ê Capsules ê Tablets ê Enteric coated tablets ê Extended release tablets Slowest *Extended Release (forms) = SR (slow release), CR (controlled release), XL (extended length) Pharmaceutics
 Oral Preparations. Liquids, elixirs, syrups Fastest Suspension solutions ê Powders ê Capsules ê Tablets ê Enteric coated tablets ê Extended release tablets Slowest. *Extended Release (forms) = SR (slow release), CR (controlled release), XL (extended length) Pharmaceutics.")
11
Pharmaceutics Drug Dissolution & Absorption Parenteral Preparations
Do NOT have to dissolve 1st Subcutaneous, Intramuscular Intravenous *directly into bloodstream *immediate absorption

12
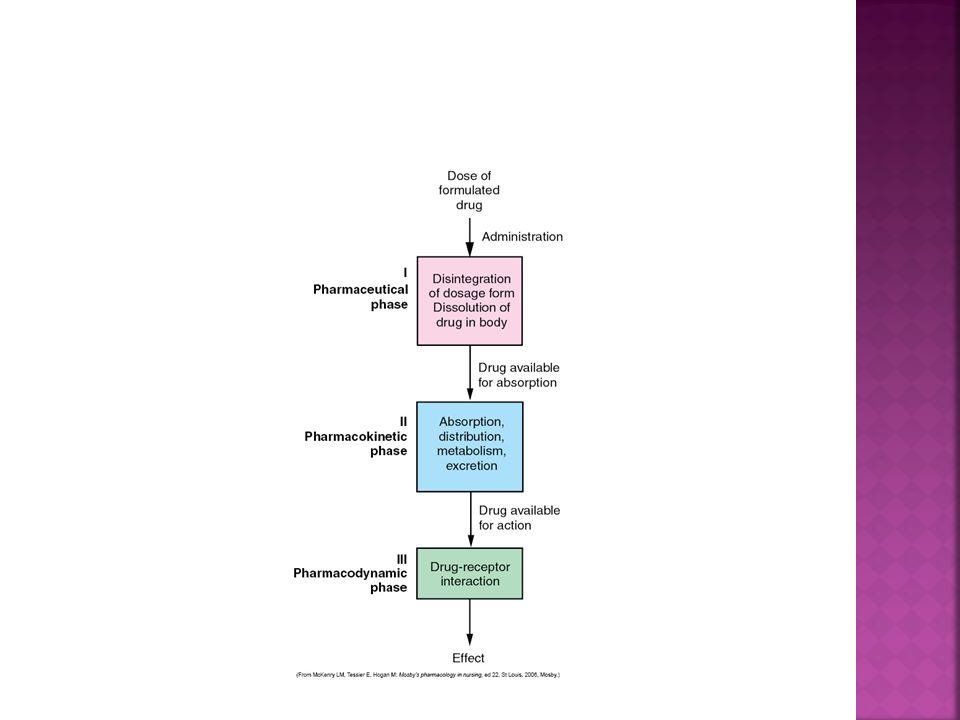
Pharmacokinetics Study of what happens to a drug from entrance into body until it leaves the body 4 phases Absorption Distribution Metabolism Excretion 4 phases

13
Pharmacokinetics - absorption
Occurs after dissolution of drug Drug → GI tract → blood/body fluids → tissue Affected by form of drug Affected by ROUTE of administration (oral, parenteral,etc.)
")
14
Pharmacokinetics—Absorption
Factors That Affect Absorption Administration route Dosage formulation Food or fluids administered with the drug Grapefruit, fruit juices, antacids, fat soluble vitamins, iron Rate of blood flow to the small intestine Acidity of the stomach Status of GI motility Empty stomach vs. “take with food” ie: Lasix ½ hr. before meals **certain meds can also decrease nut. Absorp. Grapefruit Antacids ie: 1 hour before or after meds, may bind Fat soluble vitamins – take with food, fat

15
Pharmacokinetics - Absorption
Bioavailability Extent of drug absorption Amount of drug actually available to circulation Depends upon “first pass effect” Example: Aspirin Has high “first pass effect” First pass reduces bioavailability Drugs must enter hepatic portal system, metabolized by liver, this reduces bioavailability of the drug

16
Pharmacokinetics - absorption
First Pass effect Drugs must dissolve & be absorbed by GI tract Must pass through LIVER before reaching circulation (bloodstream) Drug GI system Portal vein Liver Hepatic vein Circulation (distribution) Liver may metabolize drug into smaller metabolites Therefore, less amount of drug will pass into circulation Intravenous drugs = no “first pass” in liver Aspirin, inderal, labetolol have high first pass effect
 Drug GI system Portal vein Liver. Hepatic vein Circulation (distribution) Liver may metabolize drug into smaller metabolites. Therefore, less amount of drug will pass into circulation. Intravenous drugs = no first pass in liver. Aspirin, inderal, labetolol have high first pass effect.")
17
Pharmacokinetics—Absorption
Oral/Enteral Route Drug is absorbed into the systemic circulation through the oral or gastric mucosa, the small intestine, or rectum Oral – high “first pass” effect Sublingual – dissolve under tongue, highly vascular area, these drugs bypass liver, no “first pass” effect Buccal – same as sublingual Rectal (suppository or topical) – rectal drugs have SOME “first pass” effect
 – rectal drugs have SOME first pass effect.")
18
First-Pass Effect Illustration LASIX

19
Pharmacokinetics — Absorption
Routes that bypass the liver: Sublingual Transdermal Buccal Vaginal Rectal* Intramuscular Intravenous Subcutaneous Intranasal Inhalation *Rectal drugs may have some degree of first-pass effect

20
Pharmacokinetics—Absorption
Parenteral Route *No “first pass” effect Intravenous* Intramuscular Subcutaneous Intradermal Intraarticular (physician) *Fastest delivery into the blood circulation Intrathecal – within the spinal canal IM absorbed faster due to increased blood supply (when compared to SQ) Specially formulated IM’s: depo – 3 mos, methylprednisolone to joint/knee - weeks
 *Fastest delivery into the blood circulation. Intrathecal – within the spinal canal. IM absorbed faster due to increased blood supply (when compared to SQ) Specially formulated IM’s: depo – 3 mos, methylprednisolone to joint/knee - weeks.")
21
Pharmacokinetics— Absorption
Topical/Mucosal Route Skin Includes transdermal route, patches Eyes Ears Nose Vagina Topicals = slower onset, longer duration No “first pass” effect, bypass liver Exception = rectal Topicals: slower onset, delivers more uniform amt. of drug May have less chance for toxicity Transdermals: nicotine patch, fentanyl patch, NTG, estrogen, clonidine

22
Pharmacokinetics —Distribution
Transport of drug by bloodstream to site of action Areas of “rapid” distribution Heart Liver Kidneys Brain Areas of “slower” distribution Muscle Skin Fat Areas “difficult” to reach Bone Blood brain barrier ** Distribution aka: The transport of a drug in the body by the bloodstream to its site of action. Protein-binding Water soluble vs. fat soluble Blood-brain barrier (BBB)– does not allow passage of certain drugs – most drug books will have a notation citing a drugs affect on the BBB – NEXT SLIDE Areas of rapid distribution: heart, liver, kidneys, brain Areas of slow distribution: muscle, skin, fat A drug may be sub therapeutic or toxic. Many times blood levels are drawn to ensure adequate drug or not too much given.
– does not allow passage of certain drugs – most drug books will have a notation citing a drugs affect on the BBB – NEXT SLIDE. Areas of rapid distribution: heart, liver, kidneys, brain. Areas of slow distribution: muscle, skin, fat. A drug may be sub therapeutic or toxic. Many times blood levels are drawn to ensure adequate drug or not too much given.")
23
Pharmacokinetics - distribution
BLOOD BRAIN BARRIER Restricts passage of various chemicals between the bloodstream and the central nervous system CNS = brain, spinal cord BBB allows oxygen to pass may restrict certain bacteria & viruses Not all meds can pass through

24
Pharmacokinetics - distribution
Distribution depends upon protein-binding Albumin = most common blood protein, carries protein-bound drug molecules “bound” portion of drug = pharmacologically inactive “unbound” portion = pharmacologically active Easily distribute to body tissues (outside of blood vessels) and reach site of action Lasix, Coumadin, Aspirin, Digoxin Lasix, digoxin, dilatin, coumadin, asa - highly protein bound Bound portion may become “unbound” at a later time and circulate
 and reach site of action. Lasix, Coumadin, Aspirin, Digoxin. Lasix, digoxin, dilatin, coumadin, asa - highly protein bound. Bound portion may become unbound at a later time and circulate.")
26
Pharmacokinetics —Metabolism
aka “Biotransformation” Process by which a drug is biochemically altered inactive metabolite (compound) more potent, active metabolite Less potent, active metabolite LIVER – most responsible for metabolism of drugs Also involved = kidneys, lungs, skeletal muscle, intestines
 more potent, active metabolite. Less potent, active metabolite. LIVER – most responsible for metabolism of drugs. Also involved = kidneys, lungs, skeletal muscle, intestines.")
27
Pharmacokinetics — Metabolism
Factors that decrease metabolism: Cardiovascular dysfunction Kidney failure Liver failure Genetics Starvation Factors that increase metabolism: Certain drugs (dilantin, barbiturates, rifampin)
")
28
Pharmacokinetics —Metabolism
Delayed drug metabolism results in: Accumulation of drugs (toxicity) Prolonged action of the effects of drugs
 Prolonged action of the effects of drugs.")
29
Pharmacokinetics — Excretion
Elimination of drugs from the body All drugs must eventually be excreted Kidney = organ most responsible for excretion of drugs (urine) Also, liver (bile), bowel (feces), sweat glands Liver metabolizes most drugs, kidney excretes what is “left behind” Kidneys can also metabolize certain drugs insulin Pts with kidney dx, children (have immature kidney function), elderly may require dosage reduction and kidney function tests more frequently Drug metabolized by KIDNEY = INSULIN
 Also, liver (bile), bowel (feces), sweat glands. Liver metabolizes most drugs, kidney excretes what is left behind Kidneys can also metabolize certain drugs. insulin. Pts with kidney dx, children (have immature kidney function), elderly may require dosage reduction and kidney function tests more frequently. Drug metabolized by KIDNEY = INSULIN.")
30
Renal Drug Excretion: Glomerular filtration Free, unbound water-soluble drugs and metabolites go through passive glomerular filtration, which takes place between the blood vessels of the afferent arterioles and glomeruli Reabsorption Many substances present in the nephrons go through active tubular reabsorption. Reabsorption occurs at the level of the tubules, where substances are taken back up into the circulation and transported away from the kidney. This is an attempt by the body to retain substances that are necessary to the body’s functioning These substances are actively reabsorbed back into the systemic circulation Tubular secretion Some substances may also be secreted into the nephron from the vasculature surrounding it. Afferent – transporting towards a center – such as a sensory nerve that carries impulses toward the CNS; opposite or efferent.

31
Pharmacokinetics — Half-Life
Time required to eliminate (½) 50% of a drug Example: Digoxin hr. half-life Takes 7.5 (up to 9) days to clear Takes 5–6 half-lives to eliminate ~ 98% of a drug Liver or kidney disease Can prolong half-life Increases risk of toxicity Drugs with a shorter half-life need to be administered more frequently to maintain blood levels. Example: digoxin has a long half-life = 36 hours and only requires once daily dosing. ASA has a shorter half-life and is given more frequently. EXAMPLE: To clear a drug completely: Digoxin = 36 hours In 36 hours half drug cleared but will take 4 to 5 more 36 hours periods to clear 98% of drug 36 x 5 = 180 hours or 7 ½ days to clear 98% of digoxin
 50% of a drug. Example: Digoxin - 36 hr. half-life. Takes 7.5 (up to 9) days to clear. Takes 5–6 half-lives to eliminate ~ 98% of a drug. Liver or kidney disease. Can prolong half-life. Increases risk of toxicity. Drugs with a shorter half-life need to be administered more frequently to maintain blood levels. Example: digoxin has a long half-life = 36 hours and only requires once daily dosing. ASA has a shorter half-life and is given more frequently. EXAMPLE: To clear a drug completely: Digoxin = 36 hours. In 36 hours half drug cleared but will take 4 to 5 more 36 hours periods to clear 98% of drug. 36 x 5 = 180 hours or 7 ½ days to clear 98% of digoxin.")
32
# of half lives remainder of drug 1 50 % 2 25 % 3 12.5 % 4 6.25 % 5 3.125 %

33
Pharmacokinetics – Onset—Peak—Duration
The time it takes for the drug to elicit a therapeutic response Insulin: min Peak The time it takes for a drug to reach its maximum therapeutic response 30-60 min Duration The time a drug concentration is sufficient to elicit a therapeutic response 2-4 hours Insulin: Onset minutes Peak minutes Duration 2-4 hours

34
PHARMACOKINETICS – ONSET-PEAK-DURATION
Peak effect, maximum therapeutic response Highest blood level of the drug If too high = toxicity of drug Trough Lowest blood level of the drug If too low, then may not be therapeutic Peak, Trough - Vancomycin

35
Onset-Peak-Duration (Vancomycin example)
")
36
Pharmacokinetics: Example
Furosemide (LASIX) Pharmaceutics: Tablet, Oral solution, Injection Pharmacokinetics: Absorption: Bioavailability = 64% tablet, 60% oral soln, 100% IV Tablet, oral soln – 60 min. delay if taken w/ food Distribution: highly protein bound to albumin, 91-99% Metabolism: metabolized in liver Elimination: excreted by kidneys Onset: hr. (oral) minutes (IV) *store Peak: hr. (oral) ½ hr. (IV) room Duration: 6-8 hrs. (oral) 2 hrs. (IV) temp
 Pharmaceutics: Tablet, Oral solution, Injection. Pharmacokinetics: Absorption: Bioavailability = 64% tablet, 60% oral soln, 100% IV. Tablet, oral soln – 60 min. delay if taken w/ food. Distribution: highly protein bound to albumin, 91-99% Metabolism: metabolized in liver. Elimination: excreted by kidneys. Onset: 1 hr. (oral) 5 minutes (IV) *store. Peak: 1-2 hr. (oral) ½ hr. (IV) room. Duration: 6-8 hrs. (oral) 2 hrs. (IV) temp.")
37
Pharmacodynamics Mechanism of drug action - how drugs act at
sites of activity Involves receptors and enzymes Not all drugs have a known mechanism of action Most drugs produce more than one effect Therapeutic effect – desired or primary effect Secondary effect – may be desirable or not 1. Drug-receptor interaction: drug binds to a receptor site on cell surface, causes or blocks an action 2. Enzyme interaction: drug binds to enzyme molecule & either enhances or inhibits its action 3. Nonselective interactions: do not bind to enzyme or receptor, act on cell membrane or cell wall Wellbutrin – antidepressant, smoking Neurontin – sz and neuropathy, post-herpetic Glucophage – diabetes and PCOD Drug-receptor = PPI (prilosec) – blocks Beta blockers Enzyme interaction Nonselective = abx, change cell membrane/wall
 – blocks Beta blockers. Enzyme interaction. Nonselective = abx, change cell membrane/wall.")
38
Pharmacodynamics Drug-Receptor Interaction
Drug binds to specific receptor Alters cell function Produces desired effect Can bind completely or partially Agonists Drugs that bind and produce desired effect example, Morphine Antagonist Drugs that block agonist effect at binding site example, Narcan, reverses effect of narcotic Example, Toprol, beta-blocker, lowers HR **MSO4 – binds to opiod receptors, decrease pain = Agonist Most drugs alter cellular function. A drug usually does not completely change the function of the cell but alters part of the function. It can increase or decrease a physiologic function – ie, increase HR, decrease BP or increase urine output Drugs that bind completely will have a better effect. An antagonist will bind more tightly than the agonist – NARCAN – is a narcotic antagonist and blocks the effects of morphine-like drugs

39
Pharmacodynamics Enzyme Interaction Drug interacts with enzyme system
Inhibits the action of the enzyme The action of the cell is changed or altered Example: ACE inhibitor (Lisinopril) Inhibits conversion of angiotensin I to angiotensin II Enzymes are substances that catalyze nearly every biochemical reaction in a cell. Inhibits the action of the enzyme By “fooling” the enzyme into binding to the drug instead of its normal target cell. The target cell will not have the intended action Ie, ACE causes a enzymatic reaction that results in the production of angiotensin II, a potent vasoconstrictor. The drugs ACE inhibitors fools the ACE into binding to it rather than angiotensin I, preventing formation of angiotensin II. This results in vasodilatation and helps decrease BP
 Inhibits conversion of angiotensin I to angiotensin II. Enzymes are substances that catalyze nearly every biochemical reaction in a cell. Inhibits the action of the enzyme. By fooling the enzyme into binding to the drug instead of its normal target cell. The target cell will not have the intended action. Ie, ACE causes a enzymatic reaction that results in the production of angiotensin II, a potent vasoconstrictor. The drugs ACE inhibitors fools the ACE into binding to it rather than angiotensin I, preventing formation of angiotensin II. This results in vasodilatation and helps decrease BP.")
41
Pharmacotherapeutics
The treatment of pathologic conditions through the use of drugs “drug therapy” Desired therapeutic outcome Should be established before drug started What is expected ? Must be measurable and realistic Progress must be monitored (example = antibiotics) Examples of outcomes Curing disease Eliminating or reducing a existing symptom Arresting or slowing a disease process Preventing a disease or other unwanted condition Improving the quality of life Patient therapy assessment should be done prior to drug administration Current meds pt is on (OTC), prescription or illicit Pregnancy and breast-feeding status Co-morbidities Contraindication to specific drug use
 Examples of outcomes. Curing disease. Eliminating or reducing a existing symptom. Arresting or slowing a disease process. Preventing a disease or other unwanted condition. Improving the quality of life. Patient therapy assessment should be done prior to drug administration. Current meds pt is on (OTC), prescription or illicit. Pregnancy and breast-feeding status. Co-morbidities. Contraindication to specific drug use.")
42
Pharmacotherapeutics
Types of therapy Acute Maintenance Supplemental Palliative Supportive Prophylactic Empiric

43
Pharmacotherapeutics
Acute therapy Involves more intensive drug therapy Used in the acutely or critically ill Example: to maintain heart rate or BP Usually needed to maintain life ie – dopamine (vasopressor to maintain BP) Maintenance therapy May not cure but prevents progression of disease May prevent progression Used in chronic illnesses (example: hypertension, diabetes) ie – lisinopril, oral contraceptives Examples of acute; Vasopressors to maintain BP Volume expanders in shock Antibiotics in high risk trauma patients Maintenance May include birth control
 Maintenance therapy. May not cure but prevents progression of disease. May prevent progression. Used in chronic illnesses (example: hypertension, diabetes) ie – lisinopril, oral contraceptives. Examples of acute; Vasopressors to maintain BP. Volume expanders in shock. Antibiotics in high risk trauma patients. Maintenance. May include birth control.")
44
Pharmacotherapeutics
Supplemental therapy Replaces body substances needed to maintain normal functioning May not be produced by the body Produced in insufficient amounts Example: Insulin Palliative therapy Goal is to provide comfort Used in end stage illnesses Usually all other therapy has failed Example: Morphine for pain Examples of supplemental Insulin in diabetes Iron in iron-deficient patients Examples of palliative High dose opioid analgesics for cancer Oxygen for end stage COPDers

45
Pharmacotherapeutics
Supportive therapy Maintains integrity of body functions while patient recovering from illness Examples Providing fluids/electrolytes to prevent dehydration In vomiting or diarrhea Blood products or blood volume expanders Blood loss during surgery

46
Pharmacotherapeutics
Prophylactic therapy Used to prevent illness Example: pre-op antibiotics, vaccines Empiric therapy Use of a drug based on probability, certain illness/disease has likelihood of occurrence Example: Antibiotic for UTI before actual diagnosis Prophylactic therapy – example A surgeon knows, based on experience that when he makes an incision that there is a possibility of infection – thus he will give prophylactic antibiotics. Also used by dentists with patients that have valvular problems.

47
Adverse Effects - Monitoring
Adverse effects – unintended effects Side Effects Therapeutic index – ratio of toxic level to therapeutic level Low therapeutic index: difference between toxic and therapeutic dose is low – dangerous ! Example: coumadin (anticoagulant) Tolerance – Pts. decreasing response to repeated doses ie – valium, pain meds Dependence – Physiologic or psychologic need for drug addiction Must be familiar with both therapeutic action and side effects to be able to adequately monitor a drug All drugs potentially toxic and could have cumulative effects Adverse drug reactions (side effects) Undesirable drug effects May be common or rate Mild, severe or life threatening May occur with 1st dose or even many doses Often unpredictable
 Tolerance – Pts. decreasing response to repeated doses. ie – valium, pain meds. Dependence – Physiologic or psychologic need for drug. addiction. Must be familiar with both therapeutic action and side effects to be able to adequately monitor a drug. All drugs potentially toxic and could have cumulative effects. Adverse drug reactions (side effects) Undesirable drug effects. May be common or rate. Mild, severe or life threatening. May occur with 1st dose or even many doses. Often unpredictable.")
48
Adverse Effects – Monitoring
Patient’s condition - Physiological Age Infants & children need ↓ dose Immature organ function Elderly may require ↓ dose Decreased gastric acidity Dry mouth/decreased saliva Decreased liver blood flow/mass Increased body fat, decreased muscle mass Decreased kidney function Decreased gastric acidity = possible decreased or delayed absorption Dry mouth/decreased saliva = difficulty swallowing oral drugs Decreased liver blood flow/mass = delayed or decreased metabolism of certain drugs Decreased skin lipid content = possible decrease of absorption of transdermal meds Increased body fat, decrease body water = possible increase in toxicity of water-soluble drugs, more prolonged effects of fat-soluble drugs Decreased serum proteins = possible increased effect and toxicity of highly protein bound drugs Decreased kidney function= possible increased serum levels Changes in sensitivity to certain drug receptors -= increase or decrease in drug effect Polypharmacy is the taking of numerous drugs that can potentially react with one another. When practiced by the elderly, polypharmacy leads to an increase in the number of potential adverse reactions. Although multiple drug therapy is necessary to treat certain disease states, it always increases the possibility of adverse reactions. The nurse needs good assessment skills to detect any problems when monitoring the geriatric patient’s response to drug therapy.

49
Adverse Effects – Monitoring
Patient’s condition - Physiological Weight Average = 150lb Dosage adjustments Large weight differences Gender Women Smaller Different fat/water ratio May need dosage adjustments Weight In general, dosages are based on a weight of approximately 150 lb, which is calculated to be the “average” weight of men and women. A drug dose may sometimes be increased or decreased because the patient’s weight is significantly higher or lower than this average. With narcotics, for example, higher or lower than average dosages may be necessary to produce relief of pain, depending on the patient’s weight Gender: The gender of an individual may influence the action of some drugs. Women may require a smaller dose of some drugs than men. This is because many women are smaller than men and have a body fat-and-water ratio different from that of men.

50
Adverse Effects – Monitoring
Patient’s condition - Pathological Liver/kidney disease Inability to metabolize/excrete one normal dose before next drug given Leads to drug toxicity Lower doses are frequently given Liver disease Kidney disease Above description is know as Cumulative Drug Effect Disease The presence of disease may influence the action of some drugs. Sometimes disease is an indication for not prescribing a drug or for reducing the dose of a certain drug. Both hepatic (liver) and renal (kidney) disease can greatly affect drug response. The primary health care provider may then decide to prescribe a lower dose and lengthen the time between doses because liver function is abnormal. Patients with kidney disease may exhibit drug toxicity and a longer duration of drug action. The dosage of drugs may be reduced to prevent the accumulation of toxic levels in the blood or further injury to the kidney.
 and renal (kidney) disease. can greatly affect drug response. The primary health care provider may then decide to prescribe a lower dose. and lengthen the time between doses because liver function is abnormal. Patients with kidney disease may exhibit drug toxicity and a longer duration of drug action. The dosage of drugs may be reduced to prevent the accumulation of toxic levels in the blood or further injury to the kidney.")
51
Adverse Effects Allergic Reactions (hypersensitivity)
Usually begins after 2nd dose or more May occur within minutes or delay for hours or even days Immune system views “drug” as foreign substance Histamine is released S/S = skin rashes, hives, itching (urticaria or pruritis), facial swelling, difficulty breathing, sudden LOC, throat swelling (angioedema), wheezing Anaphylactic Shock Severe allergic rx, severe respiratory distress, life threatening Angioedema can be dangerous if occurs in area of airway – which usually does. Eyelids, lips, mouth and throat are most commonly affected. Your outline mentions immunological effects when talking about monitoring against toxic effects in relation to the patient's condition. I assume they are referring to the formation of antibodies in response to a certain drug, thereby sensitizing lymphocytes to produce antibodies when exposed to the drug again. This is referred to as an allergic reaction.
, facial swelling, difficulty breathing, sudden LOC, throat swelling (angioedema), wheezing. Anaphylactic Shock. Severe allergic rx, severe respiratory distress, life threatening. Angioedema can be dangerous if occurs in area of airway – which usually does. Eyelids, lips, mouth and throat are most commonly affected. Your outline mentions immunological effects when talking about monitoring against toxic effects in relation to the patient s condition. I assume they are referring to the formation of antibodies in response to a certain drug, thereby sensitizing lymphocytes to produce antibodies when exposed to the drug again. This is referred to as an allergic reaction.")
56
Mr. Carter has a rash and pruritis
Mr. Carter has a rash and pruritis. You suspect an allergic reaction and immediately assess him for other more serious symptoms. What question would be most imortant to ask Mr. Carter ?

57
A 78 y.o. man who has been diagnosed with a URI tells the nurse that he is allergic to Penicillin (PCN). Which is the most appropriate response by the nurse ? 1. “that’s to be expected, lots of people are allergic to penicillin” 2. “this allergy is not a big concern right now” 3. “what type of reaction did you have when you took penicillin ?” 4. “drug allergies don’t usually occur in older individuals”

58
Adverse Effects Idiosyncratic reaction: unexpected reaction in a particular patient, not common reaction Pharmacogenetics: study of genetic traits that result in abnormal metabolism of drugs ie: coumadin, codeine, psych drugs (chap. 5) Teratogenic effects: result in structural defects of in fetus FDA – 5 categories (A,B,C,D,X) of teratogens Category A – studies show NO risk (multivitamin) Category X – Completely contraindicated in pregnancy, HIGH fetal risk Idiosyncratic reaction – ie – sulfonamides – epidermal necrolysis (severe burn) Category A = levothyroxine
 Teratogenic effects: result in structural defects of in fetus. FDA – 5 categories (A,B,C,D,X) of teratogens. Category A – studies show NO risk (multivitamin) Category X – Completely contraindicated in pregnancy, HIGH fetal risk. Idiosyncratic reaction – ie – sulfonamides – epidermal necrolysis (severe burn) Category A = levothyroxine.")
59
Teratogens Category A No risk to fetus in first, second or third trimesters Category B Studies have not shown fetal risk in animals, but no controlled studies in pregnant women Considered safe in all trimesters (benadryl,tylenol,PCN) Category C Animal studies have revealed adverse effects on fetus Drugs should be given only if benefit outweighs risk Category D Positive evidence of harm to fetus Use may be acceptable absolutely necessary (life threatening situations) Category X Studies have shown fetal abnormalities, drug is completely contraindicated (acutane, coumadin)
 Category C. Animal studies have revealed adverse effects on fetus. Drugs should be given only if benefit outweighs risk. Category D. Positive evidence of harm to fetus. Use may be acceptable absolutely necessary (life threatening situations) Category X. Studies have shown fetal abnormalities, drug is completely contraindicated (acutane, coumadin)")
60
Pharmacognosy The study of natural drug sources
Plants Animals Four main sources of drugs Source of many hormone drugs (premarin – urine of pregnant mares; insulin – pigs & humans; heparin – pigs) Minerals (salicylic acid, sodium chloride) Laboratory synthesis The source of all early drugs was nature. Many new drugs are synthetically derived The principles of pharmacognosy have enabled isolation of the naturally occurring hormone insulin, determination of its exact genetic sequence, and synthesization of that exact sequence over and over again. This has enabled the production of synthetic human insulin Four main sources of drugs Plants Foxglove is an example – used to make cardiac glycosides – digoxin Also provide alkaloids – atropine, caffeine, nicotine Animals Hormone therapies Estrogen – urine of pregnant horses Insulin – beef, pork or human Human is either semi synthetic – converting pork to human by changing one amino acid – or is made by recombinant DNA techniques Heparing – derived from cows (bovine) or pigs (porcine) Minerals Salicylic acid, aluminum hydroxide, sodium chloride Laboratory synthesis Recombinant DNA techniques (segments of DNA from one organism artificially manipulated or inserted into DNA of another organism using gene splicing. Erythropoietin (Epogen and Procrit) Granulocyte-macrophage-colony stimulating factor (sargramostim) Granulocyte-colony stimulating factor (filgrastim) Human insulin (Humulin and Novulin)
 Minerals (salicylic acid, sodium chloride) Laboratory synthesis. The source of all early drugs was nature. Many new drugs are synthetically derived. The principles of pharmacognosy have enabled isolation of the naturally occurring hormone insulin, determination of its exact genetic sequence, and synthesization of that exact sequence over and over again. This has enabled the production of synthetic human insulin. Four main sources of drugs. Plants. Foxglove is an example – used to make cardiac glycosides – digoxin. Also provide alkaloids – atropine, caffeine, nicotine. Animals. Hormone therapies. Estrogen – urine of pregnant horses. Insulin – beef, pork or human. Human is either semi synthetic – converting pork to human by changing one amino acid – or is made by recombinant DNA techniques. Heparing – derived from cows (bovine) or pigs (porcine) Minerals. Salicylic acid, aluminum hydroxide, sodium chloride. Laboratory synthesis. Recombinant DNA techniques (segments of DNA from one organism artificially manipulated or inserted into DNA of another organism using gene splicing. Erythropoietin (Epogen and Procrit) Granulocyte-macrophage-colony stimulating factor (sargramostim) Granulocyte-colony stimulating factor (filgrastim) Human insulin (Humulin and Novulin)")
61
Drug Classifications Place drugs in similar categories
Similar general use Similar mechanisms of actions Similar contraindications Similar precautions Similar nursing implications If the student is familiar with the drug classification Will be familiar with every drug in that class Example Antihistamines – 1st generation If the student knows all the above about benadryl Looks up another drug classified as a 1st generation antihistamine – will know that drug as well

62
Drug Classifications Examples: Antibiotics Antihypertensives
Antiepileptics Sedatives Anesthetics Decongestants Antineoplastics Etc. Antidiarrheals For control and symptomatic relief of acute and chronic nonspecific diarrhea Antiepileptics (anticonvulsants) Used to decrease the incidence and severity of seizures due to various etiologies. Sedatives Used to provide sedation, usually prior to procedures Anesthetics Provide anesthesia Decongestants Used to decrease nasal and sinus stuffiness Antineoplastics Used to treat cancer
 Used to decrease the incidence and severity of seizures due to various etiologies. Sedatives. Used to provide sedation, usually prior to procedures. Anesthetics. Provide anesthesia. Decongestants. Used to decrease nasal and sinus stuffiness. Antineoplastics. Used to treat cancer.")
63
Drug References Physicians Desk Reference (PDR) U.S. Pharmacopia
National Formulary Various Nursing Drug Handbooks/References Davis Drug Guide Drug resources maintain currency of the nurse’s knowledge: PDR – drug reference utilized by physicians and other medical personal Annually published Detailed info – prescribing issues 6.2 United States Pharmacopeia/ National Formulary – From the US Food & Drug Administration Website THE UNITED STATES PHARMACOPEIA/NATIONAL FORMULARY Edited and Published by, and Available from: United States Pharmacopeial Convention, Inc., Twinbrook Parkway, Rockville, MD 20852 The USP/NF enjoys official status through recognition by statute [Food Drug,Formulary Cosmetic Act (FD&C Act), 201(g)(1), 201(j), and 501(b)]. The methods and tests described in this compendium are accepted as official methods, and any drug or preparation bearing a name recognized in this compendium will have its strength, quality, and purity defined by the test and assays in the compendium.Format and Purpose: The hardbound volume is a compilation of individual monographs arranged alphabetically by principal drug entity, for the application and interpretation of standards, tests, assays, and other specifications for drug substances, dosage forms, and pharmaceutical ingredients. The combination of tests and assays provided in each monograph are intended to measure the strength, quality, and purity of that product/entity. The methodology in the USP/NF is recognized as official in the Food, Drug, and Cosmetic Act. Format and Purpose: The hardbound volume consists of general information and individual monographs arranged in alphabetical order, which set specifications for quality and purity of the food additive substance and tests to measure those specifications. This compendium is recognized by regulation as setting the standards for quality and purity of those food additive substances listed as GRAS in 21 CFR 18, or affirmed as GRAS in part 184 or section [See 21 CFR (h)(1)]. Updates: The USP/NF is under continual revision. A new compendium is published every five years with supplements on an annual basis and interim revisions as applicable. The supplements and interim revisions are not included in the compendium purchase price and must be ordered by separate subscription. An ancillary publication, "Pharmaceutical Forum," is distributed bimonthly and presents proposed USP and NF text for public review and comment; occasional articles and commentary relating to USP and NF analytical methods; and the review process in general. It is also available on subscription from the U.S. Pharmacopeial Convention. lt is a valuable adjunct to the USP/NF for those laboratories that perform a moderate number of drug analyses and provides them with the means to keep updated on progress of the U.S. Pharmacopeial Convention. Other related publications available from USP include USAN ("United States Adopted Names and the USP Dictionary of Drug Names") and the USP DI ("United States Pharmacopeia Dispensing Information"), which includes dispensing information for pharmacists, such as dosage form, warnings, and drug incompatibility or known interactions. Some analysts will find these volumes useful, particularly those persons involved in drug research projects.
, 201(g)(1), 201(j), and 501(b)]. The methods and tests described in this compendium are accepted as official methods, and any drug or preparation bearing a name recognized in this compendium will have its strength, quality, and purity defined by the test and assays in the compendium.Format and Purpose: The hardbound volume is a compilation of individual monographs arranged alphabetically by principal drug entity, for the application and interpretation of standards, tests, assays, and other specifications for drug substances, dosage forms, and pharmaceutical ingredients. The combination of tests and assays provided in each monograph are intended to measure the strength, quality, and purity of that product/entity. The methodology in the USP/NF is recognized as official in the Food, Drug, and Cosmetic Act. Format and Purpose: The hardbound volume consists of general information and individual monographs arranged in alphabetical order, which set specifications for quality and purity of the food additive substance and tests to measure those specifications. This compendium is recognized by regulation as setting the standards for quality and purity of those food additive substances listed as GRAS in 21 CFR 18, or affirmed as GRAS in part 184 or section [See 21 CFR (h)(1)]. Updates: The USP/NF is under continual revision. A new compendium is published every five years with supplements on an annual basis and interim revisions as applicable. The supplements and interim revisions are not included in the compendium purchase price and must be ordered by separate subscription. An ancillary publication, Pharmaceutical Forum, is distributed bimonthly and presents proposed USP and NF text for public review and comment; occasional articles and commentary relating to USP and NF analytical methods; and the review process in general. It is also available on subscription from the U.S. Pharmacopeial Convention. lt is a valuable adjunct to the USP/NF for those laboratories that perform a moderate number of drug analyses and provides them with the means to keep updated on progress of the U.S. Pharmacopeial Convention. Other related publications available from USP include USAN ( United States Adopted Names and the USP Dictionary of Drug Names ) and the USP DI ( United States Pharmacopeia Dispensing Information ), which includes dispensing information for pharmacists, such as dosage form, warnings, and drug incompatibility or known interactions. Some analysts will find these volumes useful, particularly those persons involved in drug research projects.")
Similar presentations