Download presentation
Presentation is loading. Please wait.

1
Metro Community College Nancy Pares, RN, MSN
NURS Unit 5 Metro Community College Nancy Pares, RN, MSN

2
Informed Consent Healthcare provider must obtain
Must be obtained for invasive procedures and some medical treatments May be delayed in emergency situations

3
Objective 1 Discuss ethical, legal issues related to childhood period.

4
Nurse’s role in obtaining informed consent
Assess and document Review rights of minors Develop therapeutic relationship Verify prior consent Serve as witness

5
Minor Defined by Individual State Laws
Until the person reaches age of adult based on state law, parent or guardian must provide informed consent. Parent or guardians have ultimate decision, with some exceptions.

6
Minors May Give Informed Consent in Certain Circumstances
Emancipated minor Minor is parent of a child receiving treatment

7
Children Should Be Given Age-Appropriate Information
Assent and preference by child should be obtained

8
Advances in Medical Treatment
Ability to save lives of severely impaired infants Genetic testing Gene therapy

9
Ethical Guidelines Define Evaluate Identify Apply principles
Make decisions

10
Increase in Ethical Issues and Decisions
Nurses use four ethical principles Beneficence Nonmaleficence Autonomy Justice

11
Healthcare Institutions and Ethics Committees
Ethics committees resolve conflicts and make recommendations

13
Current Issues Causing Increasing Conflict for Nurses and Families
End of life-sustaining treatment Genetic testing of children Organ transplant Research on children

14
Communication Ongoing and cyclical
Exchange of thoughts, feelings, information Importance of trust and rapport Components—sender, message, channel, receiver, response

15
Objective 2 Discuss age appropriate assessment and therapeutic communication in the care of the child.

16
Components of Communication Cycle
Sender—generates the message Message—verbal, nonverbal, or abstract Channel—auditory, visual, kinesthetic Receiver—decodes the message Response—feedback to sender

17
Communication Forms Verbal Nonverbal Abstract

18
Verbal Communication Verbal and written words, vocalizations
Speaking to another Writing a letter Crying, laughing Influenced by development and cognitive level

19
Verbal Communication Influenced by culture
How does the nurse use verbal communication in nursing care?

20
Nonverbal Communication
Forms of Nonverbal Communication Paralanguage Gestures Touch Personal space Facial expression Body language Eye contact

21
Nonverbal Communication
Forms of Nonverbal Communication Physical appearance Facial Expression Ambiguity Influence of development and cognitive level Influence of context—what is the situation? Influence of culture Congruence between verbal and nonverbal message

22
Figure The nurse is sending a message to the older child, the receiver. Notice the nonverbal communication expressed by the young girl. What message is she communicating? How should the nurse respond?

23
Figure 6-2 Facial expressions are a powerful means of communication
Figure Facial expressions are a powerful means of communication. What does this child’s facial expression convey? What actions can the nurse take to reduce her distress?

24
Forms of Nonverbal Communication
How should nonverbal communication be applied to nursing care?

25
Considerations for Communication with Children
Developmental level Skills Language development Cognitive development Emotional/personality development

26
Newborns Primary mode of communication is nonverbal
Express self through crying Respond to human voice and presence Touch has a positive effect Nursing strategies include: encourage parent to touch infant

27
Infants Communication is still primarily nonverbal
Begin verbal communication with vocalizations Communicate through crying, facial expression Attentive to human voice and presence although no comprehension of words

28
Infants Respond to touch through patting, rocking, stroking
Nursing strategies include: speak in high- pitched voice, cuddle, pat, rub to calm

29
Toddlers and Preschoolers
Evolving verbal skills Use of language to express thoughts Greater receptive than expressive language Concrete and literal thinking,may misinterpret phrases Vocabulary depends on development and family’s use May ask many questions (preschooler)
")
30
Toddlers and Preschoolers
Short attention span Limited memory Cognitive development Egocentric Magical thinking Animism

31
Toddlers and Preschoolers
Nonverbal communication Express self through dramatic play and drawing Nursing strategies

33
School-Age Children Cognitive development now able to use logic
Begin to understand others’ viewpoints Begin to understand cause-effect Understanding of body functions

34
School-Age Children Verbal communication Nonverbal communication
Vocabulary is large Receptive and expressive language balanced Misinterpretations of phrases still common Nonverbal communication Can interpret nonverbal messages Expression of thoughts and feelings

35
Adolescents Abstract thinking without full adult comprehension
Interpretation of medical terminology is limited Drive for independence

36
Adolescents Trust and understanding build rapport Need for privacy
Nursing strategies include: straightforward approach, talk in private area

37
Communicating with Children Who Have Physical and Developmental Disabilities
If unable to communicate,may feel helplessness, fear, anxiety Family may become anxious Strategies Nonverbal—use gestures, picture boards, writing tablets Communication augmentation—system of head nods, eye blinks

38
Communicating with Children Who Have Altered Vision
Approach to child—identify self as you enter room, announce departure Orient child to objects in room Speak before touching Explain any unfamiliar sounds

39
Communicating with Children Who Have Altered Hearing
Approach to child—face child when speaking, enter room slowly Assess degree of impairment—may need interpreter

40
Communicating with Non-English-Speaking Children
Cultural implications—need to develop plan of care in respect of culture Use of interpreters Family—could result in errors and inconsistency Use professional translators trained for patient encounters Other strategies include: communication with pictures, speaking in normal tone

41
Communication Assessment for Child and Family
Development Language Physical skills Culture Barriers

42
Play Culture Journaling

43
Communication as a Cornerstone of History Taking
Importance of rapport What is rapport? How do you establish rapport? With parents? With children?

44
Strategies to Facilitate Rapport and Data Collection
Introduction Purpose of interview Use of open- and closed-ended questions Timing of questions Nonverbal communication Observations Honesty Language

46
Physiological Data Past health and illness history/ages of occurrence
Birth history Communicable diseases and illnesses Hospitalizations and surgery Injuries

48
Physiological Data Current health status Family History
Health maintenance pattern and last visit Family History

49
Physiological Data Medications—prescribed and OTC Allergies
Immunization status—up to date? Safety Activity and exercise Nutrition Sleep

51
Physiological Data Review of systems

53
Psychosocial Data Family composition
Home environment, housing, neighborhood School or childcare Daily routines

54
Psychosocial Data Changes in family or family life since last healthcare encounter Separation, divorce, or death of a parent Who lives in the household? Age-specific issues Newborns Adolescents

55
Psychosocial Data Developmental status, history, and patterns Motor
Cognitive Language Social

56
Facilitating Examination of Infants
Praise parental presence and responses Promote physical comfort and relaxation Distract infant with colorful toys Auscultate when quiet or sleeping Do procedures that provoke crying at end of exam

57
Facilitating Examination of Toddlers
Parent’s lap Play Security object Instruments Control and choice

58
Facilitating Examination of Preschoolers
Sequence Games and activities Demonstrate and let them touch instruments Distraction

59
Facilitating Examination of Older Children and Adolescents
Ensure modesty and privacy Offer choices Explain body parts and functions Decide on parental presence or absence Consider need for nonparent chaperones Reassure adolescents of normalcy

60
Head Chest Abdomen Spine Skin imperfections
Physiologic differences in children may produce normal variations in physical assessment Head Chest Abdomen Spine Skin imperfections

61
Figure Mongolian spots are large patches of bluish skin often seen on the buttocks. They are a normal occurrence in a large majority of Native American, Asian, Black, and Hispanic infants, but are sometimes mistaken for bruises.

62
General Appraisal Appearance Behavior Interaction with parents
Interaction with examiner

63
Anthropometric Measurements
Length Birth to 24 months Measuring board

64
Figure 7-4 Measuring infant length
Figure Measuring infant length. Have an assistant hold the infant’s head in the midline while you gently push down on the knees until the legs are straight. Position the heels of the feet on the footboard, and record the length to the nearest 0.5 cm or 1/4 inch.

65
Anthropometric Measurements
Height After age 2 years Stadiometer

66
Anthropometric Measurements
Weight Infant scale Kilograms, grams, and pounds and ounces Standing scale Diapers and clothing

67
Figure 7-6 Measuring head circumference
Figure Measuring head circumference. Wrap the tape around the head at the supraorbital prominence, above the ears, and around the occipital prominence, the point of largest circumference of the head.

68
Anthropometric Measurements
Centimeters and inches Paper tape Measure twice Up to age 2 to 3 years Around supraorbital and occipital prominences

69
Anthropometric Measurements
Body mass index Less than 5th percentile Greater than 85th percentile Greater than 95th percentile Calculation: weight in kg/m2 of height

70
Skin and Hair Skin Hair Color, temperature, moisture Rashes, lesions
Skin turgor Hair Texture, amount, fullness Breaking off? Head lice

71
Head and Face Shape of head and face Symmetry

72
Figure Draw an imaginary line down the middle of the face over the nose and compare the features on each side. Significant asymmetry may be caused by paralysis of cranial nerve V or VII, in utero positioning, or swelling from infection, allergy, or trauma.

73
Head and Face Skull sutures Fontanels

74
Figure The sutures are fibrous connections between the bones of the skull that have not yet ossified. The fontanels are formed at the intersection of these sutures where bone has not yet formed. Fontanels are covered by tough membranous tissue that protects the brain. The posterior fontanel closes between 2 and 3 months after birth. The anterior fontanel and sutures are palpable up to the age of 18 months. The suture lines of the skull are seldom palpated after 2 years of age. After that time, the sutures rarely separate.

75
Eyes Inspection Hypertelorism Palpebral slant

76
Figure Draw an imaginary line across the medial canthi and extend it to each side of the face to identify the slant of the palpebral fissures. When the line crosses the lateral canthi, the palpebral fissures are horizontal and no slant is present. When the lateral canthi fall above the imaginary line, the eyes have an upward slant. A downward slant is present when the lateral canthi fall below the imaginary line. Epicanthal folds are present when an extra fold of skin partially or completely covers the caruncles in the medial canthi. What type of slant does this child have? Are epicanthal folds present?

77
Figure 7-17 The eyes of this boy with Down syndrome show an upward slant.

78
Eyes Inspection Extraocular movements (EOMs)
")
79
Figure 7-18 Inspection of the extraocular movements
Figure Inspection of the extraocular movements. Have the child sit at your eye level. Hold a toy or penlight about 30 cm (12 in.) from the child’s eyes and move it in all six directions indicated. Both eyes should move together, tracking the object.
 from the child’s eyes and move it in all six directions indicated. Both eyes should move together, tracking the object.")
80
Eyes Inspection Strabismus Light reflex Cover-uncover test

81
Figure 7-19 Cover–uncover test
Figure Cover–uncover test. With the child at your eye level, ask the child to look at a picture on the wall. A, As you cover one eye with an index card or paper cup, observe for any movement of the uncovered eye. If it jumps to fixate on the picture, the uncovered eye has a muscle weakness. B, As you remove the cover from the eye, observe the covered eye for any movement to fixate on the picture. If an eye has a muscle weakness, it will drift to a relaxed position when covered.

82
Eyes Vision Fundoscopy Infant tracking
Age-appropriate tests of visual acuity Fundoscopy Red reflex Internal structures
![]()
84
Ears Inspection Tympanic membrane Symmetry Shape of tragus
Position and alignment Ear canal Tympanic membrane

86
Ears Hearing assessment Newborn screening Audiometry
Noise and whisper tests Tympanometry Bone and air conduction tests Indicators of hearing loss

87
Nose and Sinuses Inspection Palpation Percussion Patency Smell

88
Mouth and Throat Lips Teeth Gums Mucosa Tongue Throat and tonsils

89
Neck and Lymph Nodes Inspection Palpation Swelling Webbing Nodes
Trachea Thyroid gland

90
Figure The neck is palpated for enlarged lymph nodes around the ears, under the jaw, in the occipital area, and in the cervical chains of the neck.

91
Neck and Lymph Nodes Range of motion Torticollis Meningismus

92
Chest Inspection Shape Chest deformities

93
Figure Measure the chest with a tape measure placed just under the axilla and at the nipple line. Record the circumference to the nearest 0.5 cm or 1/4 inch.

94
Figure 7-36 Two types of abnormal chest shape
Figure Two types of abnormal chest shape. A, Pectus excavatum (funnel chest). B, Pectus carinatum (pigeon chest).
. B, Pectus carinatum (pigeon chest).")
95
Chest Inspection Movement, excursion
Respiratory effort, retractions, respiratory rate Breasts

96
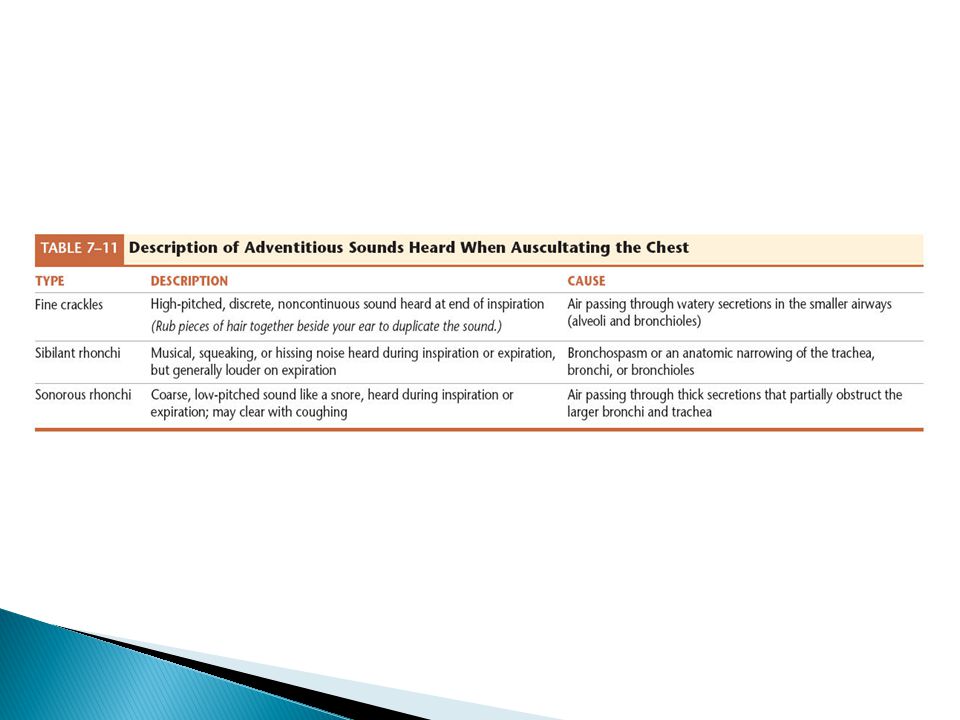
Chest Palpation Auscultation Percussion Crepitus Tactile fremitus
Hyperresonance Percussion

97
Figure 7-37 One example of a sequence for auscultation of the chest.

98
Heart Inspection Palpation Percussion Precordial activity PMI
Apical impulse Thrills Percussion

99
Heart Auscultation Rate and rhythm

101
Heart Auscultation Normal heart sounds S1 and S2 Splitting S3

103
Heart Auscultation Abnormal heart sounds Murmurs
Intensity, location, radiation, timing, quality Intensity grades Venous hum

105
Heart Pulse Related assessments Blood pressure

106
Abdomen Inspection Shape Umbilicus Rectus muscle Abdominal movements
Inguinal area

107
Figure 7-45 Sequence for indirect percussion of the abdomen.

108
Abdomen Auscultation Percussion Palpation

109
Genitalia and Perineal Areas
Positioning Timing in examination Females Males Anus and rectum

110
Genitalia and Perineal Areas
Puberty and sexual maturation Females Males Tanner Scale Sexual maturity rating (SMR)
")
111
Musculoskeletal System
Inspection Palpation Range of motion Muscle strength

112
Figure 7-54 Inspection of the spine for scoliosis
Figure Inspection of the spine for scoliosis. Ask the child to slowly bend forward at the waist, with arms extended toward the floor. Run your forefinger down the spinal processes, palpating each vertebra for a change in alignment. A lateral curve to the spine or a one-sided rib hump is an indication of scoliosis.

113
Musculoskeletal System
Posture and spinal alignment

114
Figure 7-52 Normal development of posture and spinal curves
Figure Normal development of posture and spinal curves. A, Infant 2 to 3 months—Holds head erect when held upright; thoracic kyphosis when sitting.

115
Figure 7-52 (continued) Normal development of posture and spinal curves. B, 6 to 8 months—Sits without support; spine is straight.

116
Figure 7-52 (continued) Normal development of posture and spinal curves. C, 10 to 15 months— Walks independently; straight spine.

117
Figure 7-52 (continued) Normal development of posture and spinal curves. D, Toddler—Protuding abdomen; lumbar lordosis.

118
Figure 7-52 (continued) Normal development of posture and spinal curves. E, School-age child—Height of shoulders and hips is level; balanced thoracic convex and lumbar concave curves.

119
Figure Does this child have legs of different lengths or scoliosis? Look at the level of the iliac crests and shoulders to see if they are level. See the more prominent crease at the waist on the right side? This child could have scoliosis.

120
Musculoskeletal System
Upper extremities Shoulders Arms and elbows Hands and wrist

121
Figure 7-55 A, Normal palmar creases.

122
Figure 7-55 (continued) B, Transverse crease associated with Down syndrome. Source: Photo B from Zitelli, B. J., & Davis, H. W. (Eds.). (2002). Atlas of pediatric physical diagnosis (4th ed.). St. Louis, MO: Mosby-Year Book.
. (2002). Atlas of pediatric physical diagnosis (4th ed.). St. Louis, MO: Mosby-Year Book..")
123
Musculoskeletal System
Lower extremities Hips

124
Figure Flex the infant’s hips and knees so the heels are as close to the buttocks as possible. Place the feet flat on the examining table. The knees are usually the same height. A difference in knee height (Allis sign) is an indicator of hip dislocation (see also Chapter 35). Source: Courtesy of Dee Corbett, RN, Children’s National Medical Center, Washington, DC.
 is an indicator of hip dislocation (see also Chapter 35). Source: Courtesy of Dee Corbett, RN, Children’s National Medical Center, Washington, DC..")
125
Figure 7-57 Ortolani-Barlow maneuver
Figure Ortolani-Barlow maneuver. A, Place the infant on his or her back and flex the hips and knees at a 90-degree angle. Place a hand over each knee with the thumb over the inner thigh, and the first two fingers over the upper margin of the femur. Move the infant’s knees together until they touch, and then put downward pressure on one femur at a time to see if the hips easily slip out of their joints or dislocate.

126
Figure 7-57 (continued) Ortolani-Barlow maneuver
Figure 7-57 (continued) Ortolani-Barlow maneuver. B, Slowly abduct the hips, moving each knee toward the examining table. Keep pressure on the hip joints with the fingers in a lever-type motion. Equal hip abduction, with the knees nearly touching the examining table, is normal. Any resistance to abduction or a clunk felt on palpation can be an indication of a congenital hip dislocation.
 Ortolani-Barlow maneuver. B, Slowly abduct the hips, moving each knee toward the examining table. Keep pressure on the hip joints with the fingers in a lever-type motion. Equal hip abduction, with the knees nearly touching the examining table, is normal. Any resistance to abduction or a clunk felt on palpation can be an indication of a congenital hip dislocation.")
127
Musculoskeletal System
Lower extremities Legs and knees Feet and ankles

128
Figure To evaluate the child with knock-knees, have the child stand on a firm surface. Measure the distance between the ankles when the child stands with the knees together. The normal distance is not more than 5 cm (2 in.) between the ankles.
 between the ankles..")
129
Nervous System Cognitive functioning Behavior Communication skills
Memory Level of consciousness

130
Nervous System Cerebellar function Balance Coordination
Locomotion, gait

132
Nervous System Sensory functioning Primitive reflexes
Superficial and deep tendon reflexes

134
Table 7-20 (continued) Techniques for Assessing Selected Primitive Reflexes, with Normal Findings and Their Expected Age of Occurrence
 Techniques for Assessing Selected Primitive Reflexes, with Normal Findings and Their Expected Age of Occurrence")
136
Table 7-20 (continued) Techniques for Assessing Selected Primitive Reflexes, with Normal Findings and Their Expected Age of Occurrence
 Techniques for Assessing Selected Primitive Reflexes, with Normal Findings and Their Expected Age of Occurrence")
137
Secondary Sex Characteristics
Onset of secondary sex characteristics vary Sexual maturity rating (SMR) Females: average of breast and pubic hair development Males: average of genital and pubic hair development
 Females: average of breast and pubic hair development. Males: average of genital and pubic hair development.")
138
Secondary Sex Characteristics
Tanner stages: rating between 2–5, stage 1 is prepubertal Inspection and palpation to assign a tanner stage

139
Analyzing Health Assessment Findings
Identify normal findings Identify abnormal findings Sort normal from abnormal findings Group normal and abnormal findings together Recognize patterns from normal and abnormal findings Identify health concerns, problems, conditions

140
Planning and Implementation
Appropriate referral for treatment Determination of nursing diagnoses based on health assessment findings Collaboration with child, family, other healthcare providers to develop goals Identification and implementation of appropriate interventions

141
Assessment of the Newly Born
Transition to extrauterine life Initiation of respirations Transition from fetal to adult circulation

142
Immediate Assessment After Birth
Physiologic condition and needs Resuscitation Apgar score Adaptation to extrauterine life 1 and 5 minute score Apgar criteria

144
Gestational Age Assessment
Ballard gestational age assessment tool Physical characteristics Skin Lanugo Plantar surfaces

145
Figure 7-75 Ballard scoring system to assess gestational maturity
Figure Ballard scoring system to assess gestational maturity. Source: Reprinted from Ballard, J. L., Khoury, J. C., Wang, L., Eilers-Walsmann, B. L., & Lipp, R. (1991). New Ballard score, expanded to include extremely premature infants. Journal of Pediatrics, 119 (3), 417–423. Used with permission from Elsevier. Copyright Elsevier, 1991.
. New Ballard score, expanded to include extremely premature infants. Journal of Pediatrics, 119 (3), 417–423. Used with permission from Elsevier. Copyright Elsevier,")
146
Figure Sole creases. A, At a gestational age of approximately 35 weeks, the newborn has few sole creases only on the anterior portion of the foot.

147
Figure 7-64 (continued) Sole creases
Figure 7-64 (continued) Sole creases. B, At term, the newborn has deep creases down to and including the heel as the skin loses fluid and dries after birth.
 Sole creases. B, At term, the newborn has deep creases down to and including the heel as the skin loses fluid and dries after birth.")
148
Gestational Age Assessment
Ballard gestational age assessment tool Physical characteristics Breasts

149
Figure Breast tissue. To assess breast tissue, gently compress the tissue between the middle and index fingers and measure the tissue in millimeters. A, At a gestational age of 38 weeks, the newborn has a visible raised area that is 4 mm in diameter on palpation.

150
Figure 7-65 (continued) Breast tissue
Figure 7-65 (continued) Breast tissue. To assess breast tissue, gently compress the tissue between the middle and index fingers and measure the tissue in millimeters. B, At a gestational age of 40 to 44 weeks, the newborn has 10 mm breast tissue.
 Breast tissue. To assess breast tissue, gently compress the tissue between the middle and index fingers and measure the tissue in millimeters. B, At a gestational age of 40 to 44 weeks, the newborn has 10 mm breast tissue.")
151
Gestational Age Assessment
Ballard gestational age assessment tool Physical characteristics Ear cartilage and eyelid fusion

152
Gestational Age Assessment
Ballard gestational age assessment tool Physical characteristics Genitals

153
Gestational Age Assessment
Ballard gestational age assessment tool Neuromuscular characteristics Posture

154
Figure 7-69 Resting posture
Figure Resting posture. A, At a gestational age of approximately 31 weeks, there is extension of the upper extremities and beginning flexion of the thighs.

155
Figure 7-69 (continued) Resting posture
Figure 7-69 (continued) Resting posture. B, At term, the newborn exhibits hypertonic flexion of all extremities.
 Resting posture. B, At term, the newborn exhibits hypertonic flexion of all extremities.")
156
Gestational Age Assessment
Ballard gestational age assessment tool Neuromuscular characteristics Square window

157
Figure 7-70 Square window sign
Figure Square window sign. A, At approximately 28 to 32 weeks’ gestation, the angle is 90 degrees.

158
Figure 7-70 (continued) Square window sign
Figure 7-70 (continued) Square window sign. B, At a gestational age of approximately 39 to 40 weeks, the angle is commonly 30 degrees.
 Square window sign. B, At a gestational age of approximately 39 to 40 weeks, the angle is commonly 30 degrees.")
159
Gestational Age Assessment
Ballard gestational age assessment tool Neuromuscular characteristics Arm recoil

160
Figure Elicit the arm recoil by flexing the arms at the elbows to the chest for 5 seconds. A, Then extend the arms at the elbows.

161
Figure 7-71 (continued) Elicit the arm recoil by flexing the arms at the elbows to the chest for 5 seconds. B, Release the arms to see the amount of recoil. In healthy newborns, the angle of flexion is usually less than 90 degrees followed by rapid recoil to the flexed position.

162
Gestational Age Assessment
Ballard gestational age assessment tool Neuromuscular characteristics Popliteal angle

163
Figure To assess the popliteal angle, flex and hold the thigh to the abdomen while extending the leg at the knee.

164
Gestational Age Assessment
Ballard gestational age assessment tool Neuromuscular characteristics Scarf sign

165
Figure Scarf sign. A, Until approximately 30 weeks’ gestation, the elbow moves past midline with no resistance.

166
Figure 7-73 (continued) Scarf sign
Figure 7-73 (continued) Scarf sign. B, The elbow will not reach midline after 40 weeks’ gestation.
 Scarf sign. B, The elbow will not reach midline after 40 weeks’ gestation.")
167
Gestational Age Assessment
Ballard gestational age assessment tool Neuromuscular characteristics Heel-to-ear extension

168
Figure 7-74 Heel-to-ear scoring
Figure Heel-to-ear scoring. Move the infant’s foot as near to the head or ear as possible and determine the distance between the heel and head.

169
Size for Age Small for gestational age Appropriate for gestational age
Large for gestational age Growth curves Accuracy of anthropometric measures in newborns

170
Figure 7-76 Measuring the length of the newborn.

171
General Appearance and Behaviors
Head/body ratio Position Motor activity Cry

172
General Appearance and Behaviors
Vital signs Thermoregulation Respirations Pulse Blood pressure

173
Physical Assessment of Newborn
Skin Peeling Lanugo Normal color variations Jaundice Common alterations

175
Physical Assessment of Newborn
Head Molding Caput succedaneum

176
Figure 7-78 Caput succedaneum
Figure Caput succedaneum. Following vaginal birth, some newborns develop swelling and a collection of serous fluid in the scalp due to birth trauma. The swelling often crosses the suture lines.

177
Physical Assessment of Newborn
Head Cephalohematoma Sutures Fontanels Symmetry

178
Figure 7-79 Cephalhematoma
Figure Cephalhematoma. Following vaginal birth, some newborns develop a collection of blood between the surface of the cranial bone and the periosteal membrane due to birth trauma. The swelling is usually confined to one cranial bone and does not cross the suture lines. Source: Photo from Zitelli, B. J. & Davis, H. W. (Eds.). (2007). Atlas of pediatric physical diagnosis (5th ed., p. 42, Fig. 2-30). From: Anonymous (2006). Cephalhematoma, Consultant for pediatricians, 5(7), 444. Reprinted with permission. Copyright Elsevier, 2007.
. (2007). Atlas of pediatric physical diagnosis (5th ed., p. 42, Fig. 2-30). From: Anonymous (2006). Cephalhematoma, Consultant for pediatricians, 5(7), 444. Reprinted with permission. Copyright Elsevier,")
179
Physical Assessment of Newborn
Eyes Chemical conjunctivitis Blink reflex Red reflex vs. opacities Sclerae Tracking Doll’s eye phenomenon

180
Physical Assessment of Newborn
Ears Position Skin lesions or tags Hearing Nose Appearance Patency of nares Flaring

181
Physical Assessment of Newborn
Mouth Palate Tongue, frenulum Buccal mucosa Gums Gag, suck, swallow Epstein’s pearls, neonatal teeth, inclusion cysts

182
Physical Assessment of Newborn
Neck Position Appearance Torticollis Webbing, skin folds Clavicles Chest

183
Physical Assessment of Newborn
Chest and Lungs Appearance—Barrel chest? Breasts—Engorgement? Nipple discharge? Respirations—Periodic breathing? Retractions? Grunting? Breath sounds

184
Physical Assessment of Newborn
Heart Location of apical impulse Murmurs Pulses Abdomen Appearance Bowel sounds Umbilicus and umbilical cord

185
Physical Assessment of Newborn
Genitalia and anus Appearance and relation to gestational age Females—vaginal discharge Males—penis, urethra, testes Patency of anus Stooling pattern Anal wink

186
Physical Assessment of Newborn
Extremities Deformities Injuries Developmental hip dysplasia Symmetry of creases Allis sign Barlow-Ortolani maneuver

187
Physical Assessment of Newborn
Spine Muscle strength and position Head control Neurological system Alertness Posture Protective reflexes Primitive reflexes

189
Objective 3 Apply the nursing process to the care of the pediatric patient in various acute care settings Acute Isolation Emergency Intensive Care

190
Health/Illness Understanding: Infant
Unaware of illness and its effects Sense stress and anxiety in loved ones Awareness of self as separate from parents by 6 months Stranger anxiety

192
Health/Illness Understanding: Toddler/Preschooler
Sees illness as punishment Has incorrect cause-and-effect perceptions Begins to understand concept of germs Knows outside body-part names Has vague knowledge of internal organs

193
Health/Illness Understanding: School-age
Knows cause and effect of illness Beginning understanding of body functions Older school age can understand explanations

194
Health/Illness Understanding: Adolescents
Understands complex nature of illness Multiple causes and effects Knows location and function of major organs Concerned with Effects of illness on appearance Body image

195
Stages of Separation Anxiety
Protest Screaming, crying, clinging Resists attempts to comfort Despair Sad, withdrawn, quiet Cries when parents return

196
Stages of Separation Anxiety
Denial Protest subsides, shows interest in setting Appears happy and content

198
Illness/Hospitalization Effects
Separation All ages affected Fear of the unknown Injections, blood, being touched by strangers Pain, disfigurement, invasive procedures, death Loss of control Mobility, autonomy, privacy

200
Table 16-2 (continued) Stressors of Hospitalization for Children at Various Developmental Stages
 Stressors of Hospitalization for Children at Various Developmental Stages")
201
Illness/Hospitalization Responses
Separation Withdrawal, abandonment, regression Fear of the unknown Sleep disruption, anxiety reactions Loss of control Aggression, regression, displacement

202
Family Responses to Hospitalization
Disruption of daily routine Role change Anxiety and fear Need support, encouragement, honest information Coping strategies Cultural views

204
Adaptation to Hospitalization
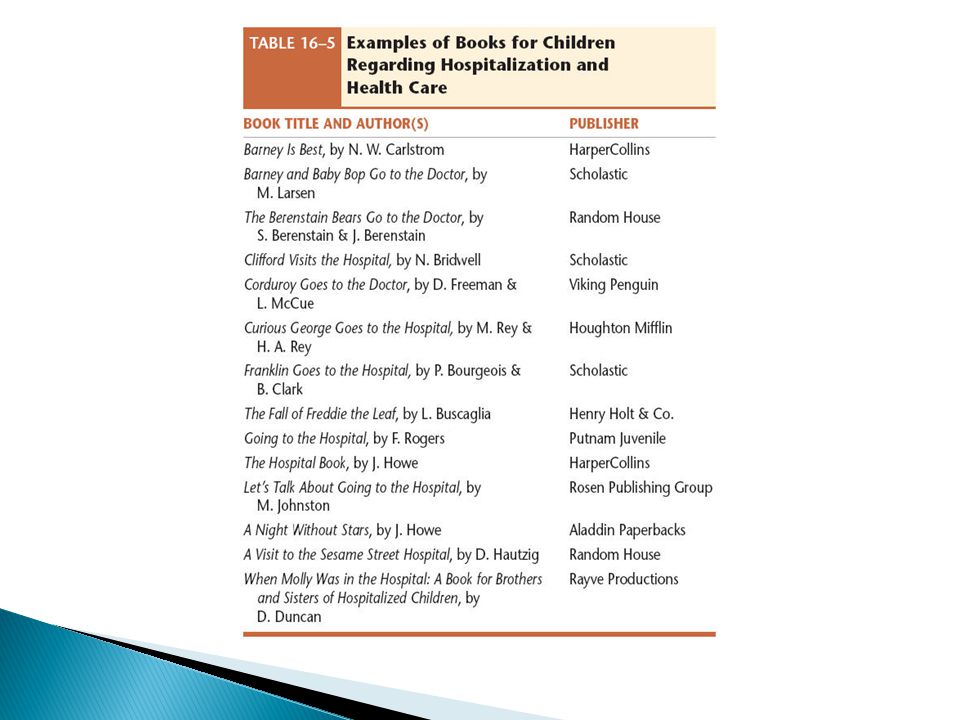
Assess family Roles, knowledge, support systems Planned hospitalization Tours, videos, books to prepare Unplanned hospitalization Great stress on child and family Siblings may feel guilt, fear, or neglect

206
Sibling Reactions Depend on Age Developmental level
Perception and severity of illness Prior experience and coping Knowledge and understanding of illness

207
Strategies for siblings
Honesty Reassurance: they did nothing wrong to cause the illness Allow questions and discussion of feelings Encourage visits: prepare patient and siblings to minimize adverse reactions

208
Stress Reduction: The 4 Rs
Recreation: toys, games, activities, physical activity Rest: calm, quiet; bedtime rituals Relationships: family members, siblings, peers, support groups Routines: follow normal routine, provide transition objects, provide consistent caregivers

209
Enhancing Hospitalization
Rooming in 24/7 parental visitation/family time Parental involvement with care Communication Phones, beepers, location of family members Contact for change in condition, procedures Education

210
Minimizing Stressors Maximize control Therapeutic play
Give choices Encourage independence Therapeutic play Address fears, concerns Therapeutic recreation Interactive activities

211
Nursing Care Focus Minimize fears and anxieties
Incorporate familiar routines into hospitalization Support family and loved ones Minimize loss of control; promote autonomy

212
Preparation for Procedures
Assessment Knowledge and previous experiences Developmental age Coping abilities Feelings: fears, concerns

213
Preparation for Procedures
Communication based on developmental level Clear Honest Age appropriate

214
Psychological Preparation
Assess: knowledge, perception, and feelings Purpose Past experience Will it be painful? Coping techniques Will parents be present?

215
Psychological Preparation
Communication Use understandable language Gear to cognitive level and past experience Share ways to cope during the procedure

216
Parental Presence Physical preparation Depends on age and procedure
NPO? Procedural checklist Pain management

217
Child Life Programs Focus on psychosocial needs Age-appropriate play
Medical play/acting out procedures Therapeutic play Dramatic play

218
Techniques for Therapeutic Play
Storytelling Drawings, body outlines Music, tape-recorded messages Puppetry Dramatic play Animal-assisted therapy

220
Special Units and Types of Care
General pediatric units Emergency department (ED) Neonatal intensive care unit (NICU), pediatric intensive care unit (PICU), or special care units Preoperative and postoperative units, post- anesthesia care units (PACU)
 Neonatal intensive care unit (NICU), pediatric intensive care unit (PICU), or special care units. Preoperative and postoperative units, post- anesthesia care units (PACU)")
221
Special Units and Types of Care
Short-stay, outpatient, or ambulatory surgical units Isolation Rehabilitation

222
Parental Involvement and Presence
Provides feelings of control Prepares family for care required at home Reduces emotional stress and anxiety Promotes feelings of value, worth, and competence to care for their child Promotes parents feeling fully informed, trust of nursing staff

224
Discharge Considerations
Family ability to provide care Equipment, training Financial burdens Educational needs Parent teaching Return to schoolwork

225
Preparation for Home Care
Plans for school, recovery, adaptation Individualized education plan (IEP) Individualized transition plan (ITP) Prepare the family Procedures, medications, emergencies Prepare parents to act as case managers
 Individualized transition plan (ITP) Prepare the family. Procedures, medications, emergencies. Prepare parents to act as case managers.")
226
Preparation for Surgery
Preoperative Teach purpose, sensations Allow transition objects: teddy bears, blankets Parental presence during anesthesia induction

229
Table 16-7 (continued) Assisting Children Through Procedures
 Assisting Children Through Procedures")
230
Preparation for Surgery
Postoperative Expectations during recovery Monitoring and assessment Nursing Care Plan:The Child Undergoing Surgery

231
Child and Family Teaching
Informal or structured For child and parents Consider timing and level of understanding Consider special health needs Translators if needed

232
Child and Family Teaching
Teaching plans: include all the domains Cognitive Psychomotor Affective

233
Teaching Steps Assess Set clear, measurable goal(s)
Knowledge, skills, feelings, expectations Cognitive level, ability, desire Set clear, measurable goal(s)
")
234
Teaching Steps Select method(s) Evaluate learning outcome
Audio, video, text, demonstration, or combination Evaluate learning outcome How well was goal met?

235
Developmental Stage Effect on understanding of death
Effect on behavioral response to death Effect on ability to communicate about death

236
Objective 4 Describe the nursing interventions and stages of grief associated with the chronically ill or dying child

238
Table 22-1 (continued) The Child’s Developmental Understanding of Death, Potential Behaviors, and Nursing Considerations
 The Child’s Developmental Understanding of Death, Potential Behaviors, and Nursing Considerations")
239
Sources of Loss for Children
Parent Grandparent Friend Pets or objects Loss of an aspect of self Loss of an object or pet Separation from an accustomed environment

240
Sources of Loss for Children
Losses not directly related to the child Crime Disasters Terror attacks

241
Factors Affecting a Child’s Response to Loss
Cultural traditions and practices Religion and spirituality Social support systems

242
Communicating with the Dying Child
Promote open communication Struggle with emotions is common Identify what is known, how much child wants to know Listen and give support

243
Withdrawing or Withholding Treatment
Decision is extremely difficult Parents or nurses may feel that aggressive therapies extend child’s suffering

244
Parental Refusal of Treatment
Parents and healthcare providers may disagree regarding interventions Refusal may be based on religious beliefs or desire to provide peaceful death Technical interventions may cause emotional stress to parents

245
Parental Refusal of Treatment
Court interventions may be used Consultation with hospital ethics committee

246
End-of-Life Decisions
Palliative care—an approach to improve QOL Hospice care—care focusing on ensuring comfort Do Not Resuscitate request Tissue and organ donation Autopsy

247
Informing Parents of a Child’s Prognosis or Death
Privacy Body language Social support Response to emotions Timing

248
Physiological Changes in the Dying Child
Illness- or injury-dependent changes

249
Physiological Changes in the Dying Child
Universal changes Cardiovascular system Respiratory system Neurological system Musculoskeletal system Renal system Altered nutrition Fluid and electrolyte imbalance

250
Assessment of the Dying Child and Family
Fears and concerns Coping skills Awareness Closed awareness Mutual pretense Open awareness Spiritual needs

251
Nursing Diagnosis for the Dying Child and Family
Fear Hopelessness Risk for caregiver role strain Interrupted family processes Anticipatory grieving

252
Planning and Implementation
Goal setting Competencies for high-quality end-of-life care

255
Planning and Implementation
Special concerns Pain management Trust Anger Education Desired religious or cultural practices

256
Arrange for Parents and Others to Say Good-bye
Allow as much time as needed for farewells Provide privacy

257
Provide Mementos Save clothing and personal items
Collect footprints, locks of hair, and so on Preserve the last clothes worn in a sealed bag to retain the child’s scent

258
Postmortem Care Identify and implement any religious or cultural practices desired by the family Clean and position the body

259
Psychosocial Support Help parents predict when they may expect increased grief Remind parents to care for themselves mentally and physically Tell parents that people progress through grief at different rates

260
Psychosocial Support Remind parents that grief puts a tremendous stress on relationships Encourage parents to provide for ongoing support of siblings Arrange for continued follow-up for families after the acute period of grief

261
Nurses Who Work with Dying Children May Feel:
Helpless That they failed the dying child Sad Grief

262
Stress Management Special preparation is required for the nurse
Mentorship with hospice nurse Debriefing sessions with mental health professional

Similar presentations









































) p. 201- 206 By : Mohammad Abuadas RN, MSN.>")




 Low Birth Weight (LBW) Cerebral Palsy (CP) Respiratory Distress Syndrome (RDS) Cyanosis Bluish color skin and lips Bronchopulmonary.>")