Download presentation
Presentation is loading. Please wait.

1
Metabolic Factors / NAFLD on the Natural History of Chronic Hepatitis B or C in Asia Pei-Jer Chen National Taiwan University & Hospital

2
Insulin resistance Metabolic Factors HBV or HCV Hepatic steatosis

3
23820 cohort members (11973 males and 11847 females), recruited in 1991 4155 HBsAg sero-positive (2445 males and 1710 females ) 19665 HBsAg sero-negative (9528 males and 10137 females--- anti HCV assay Flow chart of the REVEAL cohort HBV DNA TG. Chole. HCV RNA DM

4
Cross-Section Study: CHB/CHC versus Control in terms of Metabolic Factors A study of base-line data in the REVEAL cohort A study of base-line data in the REVEAL cohort

5
Metabolic factors: Obesity Central obesity: waist circumferences >90 cm for men and >80 cm for women. and >80 cm for women. Body Mass Index: normal weight BMI< 23 kg/m 2 overweight 23 < BMI < 25 kg/m 2 overweight 23 < BMI < 25 kg/m 2 obese 25 < BMI < 30 kg/m 2 obese 25 < BMI < 30 kg/m 2 morbid obese BMI > 30 kg/m 2 morbid obese BMI > 30 kg/m 2 Hypercholesterolemia : total cholesterol > 240 mg/dL mg/dL Hypertriglyceridemia : TG > 150 mg/dL History of DM History of hypertension

6
Table. Multivariate-adjusted odds ratios of being HBsAg seropositive in relation to selected metabolic factors

7
HBV Infection does not Correlates with the Development of NAFL or IR (1) AuthorSetting Populatio n ResultsRemarks Moucari (2008) Cross- sectional 500 CHC, 100 CHB IR: 5% in CHB and 35% in CHC Not matched Wang (2007) Health examinatio n 50 CHB and 457 controls HBV carriers not associated with IR or FL Small sample size Mohamma d (2006) Case control 60 CHC and 40 CHB HOMA-IR associated with fibrosis in CHC, but not in CHB Selection bias, small size Tsochatzi s (2007) Case series 213 eAg- ve CHB Hepatic steatosis less frequent in CHB than in CHC; associated with metabolic factors Selection bias, not representative Cindoruk (2007) Treatment cohort 140 CHB Presence of steatosis not associated with HBV load Selection bias, not representative Demir (2007) Case series 49 eAg-ve CHB NAFLD: most common cause of elevated ALT in patients with CHB Selection bias, small size Moucari et al, Gastroenterology 2008; Wang et al, JGH 2007; Mohammad et al, Indian J Gastroenterol 2006; Tsochatzis et al, Dis Liver Dis 2007; Lin et al, WJG 2007; Cindoruk et al, J Clin Gastroenterol 2007; Demir et al, Ann Hepatol 2007
 AuthorSetting Populatio n ResultsRemarks Moucari (2008) Cross- sectional 500 CHC, 100 CHB IR: 5% in CHB and 35% in CHC Not matched Wang (2007) Health examinatio n 50 CHB and 457 controls HBV carriers not associated with IR or FL Small sample size Mohamma d (2006) Case control 60 CHC and 40 CHB HOMA-IR associated with fibrosis in CHC, but not in CHB Selection bias, small size Tsochatzi s (2007) Case series 213 eAg- ve CHB Hepatic steatosis less frequent in CHB than in CHC; associated with metabolic factors Selection bias, not representative Cindoruk (2007) Treatment cohort 140 CHB Presence of steatosis not associated with HBV load Selection bias, not representative Demir (2007) Case series 49 eAg-ve CHB NAFLD: most common cause of elevated ALT in patients with CHB Selection bias, small size Moucari et al, Gastroenterology 2008; Wang et al, JGH 2007; Mohammad et al, Indian J Gastroenterol 2006; Tsochatzis et al, Dis Liver Dis 2007; Lin et al, WJG 2007; Cindoruk et al, J Clin Gastroenterol 2007; Demir et al, Ann Hepatol 2007")
8
AuthorSetting Populatio n ResultsRemarks Persico (2009) Cohort 726 CHC, 126 CHB Age and BMI correlate with steatosis in CHB Selection bias Yun (2009) Liver biopsy series 86 young male CHB Steatosis associated with TG level and HOMA IR Small sample size Imazeki (2008) Case series 544 CHC, 286 CHB, 122 controls IR in CHB (36%) similar to controls (36%), but lower than in CHC (54%) Selection bias, not matched Kumar (2009) Case control 69 CHC and 50 healthy controls HOMA-IR associated with BMI, but not CHB itself Selection bias, small size Persico et al, World J Gastroenterol 2009; Yun et al, Liver Int 2009; Kumar et al, Am J Gastroenterol 2009; Imazeki et al, Liver Int 2008 HBV Infection does not Correlates with the Development of NAFL or IR (2)
 Cohort 726 CHC, 126 CHB Age and BMI correlate with steatosis in CHB Selection bias Yun (2009) Liver biopsy series 86 young male CHB Steatosis associated with TG level and HOMA IR Small sample size Imazeki (2008) Case series 544 CHC, 286 CHB, 122 controls IR in CHB (36%) similar to controls (36%), but lower than in CHC (54%) Selection bias, not matched Kumar (2009) Case control 69 CHC and 50 healthy controls HOMA-IR associated with BMI, but not CHB itself Selection bias, small size Persico et al, World J Gastroenterol 2009; Yun et al, Liver Int 2009; Kumar et al, Am J Gastroenterol 2009; Imazeki et al, Liver Int 2008 HBV Infection does not Correlates with the Development of NAFL or IR (2)")
9
Summary Obesity, history of diabetes : Prevalence not increase in HBsAg sero-positive subjects TG>150: in HBsAg sero-positive cases

10
Metabolic factors and Hepatitis C infection Relationship with anti-HCV status and HCV RNA levels cross-section Relationship with anti-HCV status and HCV RNA levels cross-section

11
Table. Multivariate-adjusted Odds Ratios of being anti-HCV seropositive relation to selected risk factors

12
Summary Obesity, Diabetes : Increased in anti-HCV seropositive cases. TG<150: anti-HCV seropositive Serum triglyceride level, total cholesterol level and body mass index are inversely correlated with HCVRNA viral load

13
NATURE CELL BIOLOGY 2007; 9:961-9 Huh-7 cells transfected with JFH1 RNA Core recruits NS proteins to LDs

14
HCV and Lipids Negro and Sanyal. Liver Int 2009;29:26

15
23820 cohort members (11973 males and 11847 females) 4155 HBsAg sero-positive (2445 males and 1710 females ) 19665 HBsAg sero-negative (9528 males and 10137 females) 18541 anti-HCV seronegative Flow chart of the REVEAL cohort 3931 anti-HCV seronegative 218 anti-HCV seropositive 1095 anti-HCV seropositive HCC n=187 LC n=429 LC death n=57 Liver death n=212 HCC n=51 LC death n=16 Liver death n=74 HCC n=53 LC death n=61 Liver death n=108 10 years follow-up
 4155 HBsAg sero-positive (2445 males and 1710 females ) HBsAg sero-negative (9528 males and females) anti-HCV seronegative Flow chart of the REVEAL cohort 3931 anti-HCV seronegative 218 anti-HCV seropositive 1095 anti-HCV seropositive HCC n=187 LC n=429 LC death n=57 Liver death n=212 HCC n=51 LC death n=16 Liver death n=74 HCC n=53 LC death n=61 Liver death n= years follow-up")
16
Metabolic factors and Incident Hepatocellular Carcinoma (HCC)
")
17
Table. Multivariate-adjusted relative risks of HCC in relation to selected risk factors stratified by HBV and HCV infection status

19
Table. Relative risks of HCC by HBsAg, anti-HCV serological status, obesity and history of diabetes mellitus (DM)
.")
20
BMI<30 DM (-) 15.7 (10.2– 24.1) HBsAg (-) anti-HCV (+) BMI>30 DM (-) 33.6 (12.0– 94.2) HBsAg (-) anti-HCV (+) BMI<30 DM (+) 63.6 (22.6– 179) HBsAg (-) anti-HCV (+) BMI>30 DM (+) 134.5 (17.5– 1035)
 15.7 (10.2– 24.1) HBsAg (-) anti-HCV (+) BMI>30 DM (-) 33.6 (12.0– 94.2) HBsAg (-) anti-HCV (+) BMI<30 DM (+) 63.6 (22.6– 179) HBsAg (-) anti-HCV (+) BMI>30 DM (+) (17.5– 1035)")
21
Summary I: Obesity: –Anti-HCV positive: Central obesity: 2-fold increased risk BMI > 30 kg/m 2 : 4-fold increased risk –HBsAg positive: Central obesity: 33% increased risk BMI: no association DM –Anti-HCV positive: 3 to 4 fold increased risk –HBsAg positive: 2-fold increased risk

22
Summary II: Combine HBV, HCV serological status with obesity and DM Compare to HBsAg (-) + anti-HCV (-) + DM (-) + BMI <30 kg/m 2 –HBsAg(+) + DM(+) + BMI >30 kg/m 2 RR=265 (95% CI = 35 – 1993) RR=265 (95% CI = 35 – 1993) –Anti-HCV(+) + DM(+) + BMI >30 kg/m 2 RR=135 (95% CI=18 – 1035) RR=135 (95% CI=18 – 1035) Synergistic effects of metabolic factors and hepatitis infections on HCC
 + anti-HCV (-) + DM (-) + BMI <30 kg/m 2 –HBsAg(+) + DM(+) + BMI >30 kg/m 2 RR=265 (95% CI = 35 – 1993) RR=265 (95% CI = 35 – 1993) –Anti-HCV(+) + DM(+) + BMI >30 kg/m 2 RR=135 (95% CI=18 – 1035) RR=135 (95% CI=18 – 1035) Synergistic effects of metabolic factors and hepatitis infections on HCC")
23
Fatty Liver and Incident Hepatocellular Carcinoma (HCC)
")
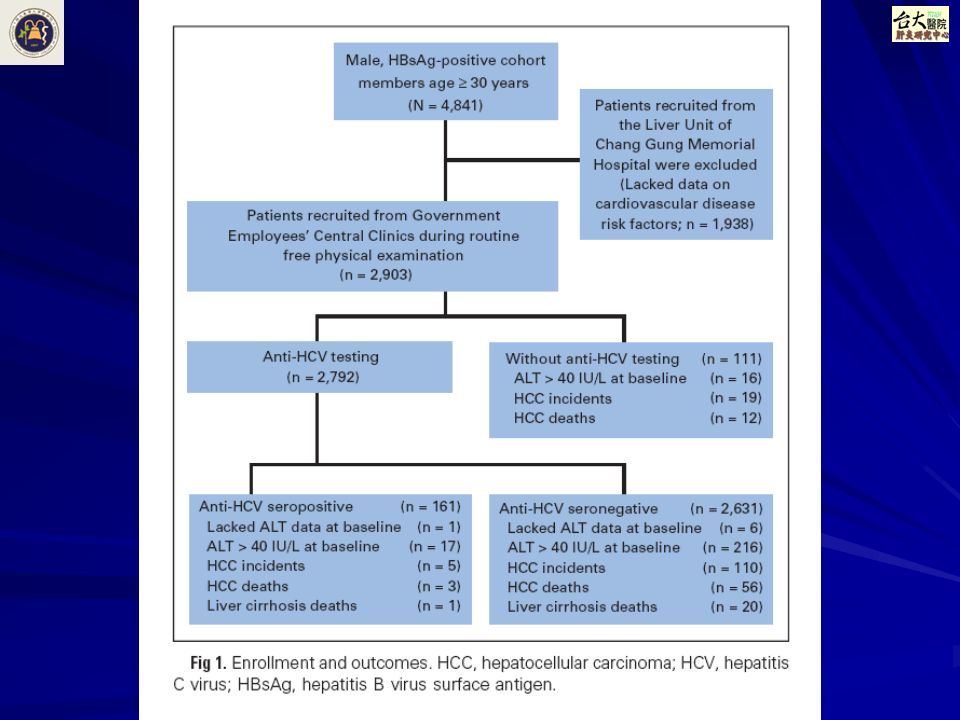
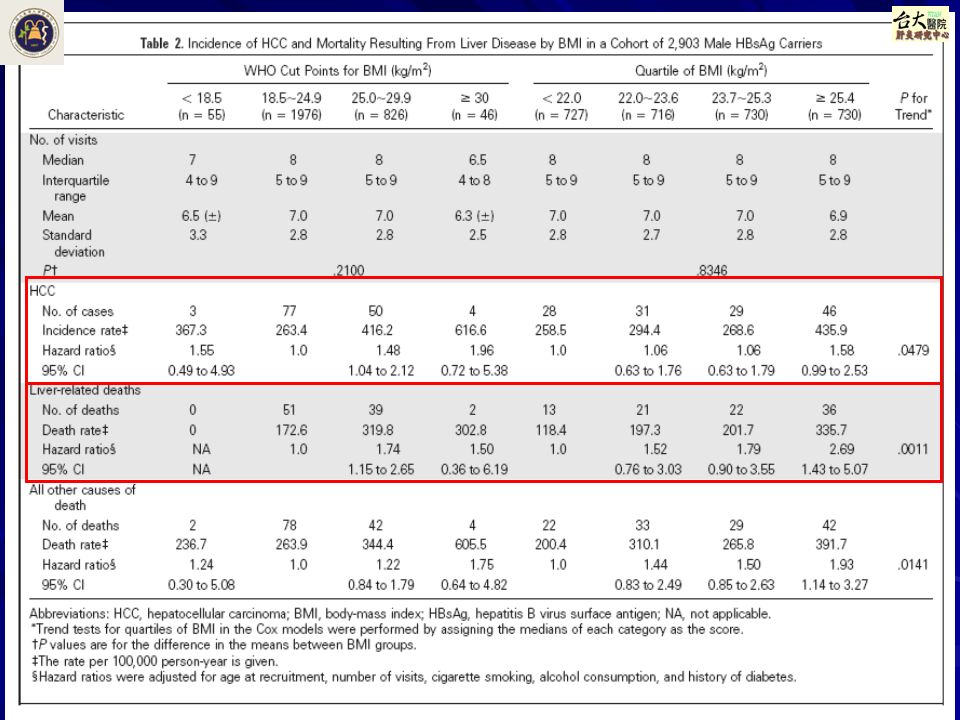
28
Results Hazard ratios for incident HCC –1.48 in overweight (BMI 25.0~29.9 kg/mm) –1.96 in obese (BMI≥30.0) –compared with normal-weight (BMI 18.5~24.9) men Liver-related mortality had –adjusted hazard ratios 1.74 in overweight and 1.50 in obese men Excess BMI associated with the occurrence of fatty liver and cirrhosis
 –1.96 in obese (BMI≥30.0) –compared with normal-weight (BMI 18.5~24.9) men Liver-related mortality had –adjusted hazard ratios 1.74 in overweight and 1.50 in obese men Excess BMI associated with the occurrence of fatty liver and cirrhosis")
30
Summary (I) In patients with CH-B, Prevalence of hepatic steatosis similar in pts with CHB vs. in general population HBsAg carriage not associated with IR Metabolic derangement rather than viral factors more closely associated with the development of steatosis Concurrent metabolic syndrome may accelerate the progression of CHB

31
Summary (II) HCV infection may induce IR and liver steatosis. HCV life cycle is closed linked to lipid metabolism Concurrent metabolic factors (increased BMI, DM) accelerate the progression of CHC In Patients with CHC:
 accelerate the progression of CHC In Patients with CHC:.")
32
Conclusions and Perspectives After controlling for the virus effect, obesity consistently shows to be associated with higher risk of different spectrum of liver diseases: from hepatitis to liver diseases related death. Hypertriglyceridemia: maybe an indication (biomarker) for better liver function? Mechanism remains unknown? The role of fatty liver in the relationship between metabolic factors and end stage liver diseases remains unknown Long term follow up of NAFLD patients without hepatitis is needed
 for better liver function. Mechanism remains unknown. The role of fatty liver in the relationship between metabolic factors and end stage liver diseases remains unknown Long term follow up of NAFLD patients without hepatitis is needed.")
33
Metabolic Factors NAFLD Cirrhosis HCC HBV, HCV ? HBV? HCV? Background HBV

Similar presentations
















 A NEW NON-INVASIVE BIOMARKER FOR ASSESSING LIVER FIBROSIS AND RISK OF PROGRESSION TO HEPATOCELLULAR CARCINOMA N.K. Gatselis,>")
, ABIM Gastoenterologist King Abdulaziz University Hospital.>")
, ABIM Gastoenterologist King Abdulaziz University Hospital.>")




