Download presentation
Presentation is loading. Please wait.

1
DEFINITION INTERRUPTION IN THE ABORAL PASSAGE OF INTESTINAL CONTENTS
אין מעבר של תוכן מעי- גזים צואה. זה יוכל להיות לאורך כל מערכת העיכול.

2
The common Scenario A 50 year old man presents with abdominal pain, distension, obstipation and constipation, with repeated episodes of vomiting. His vital sign were stable, abdomen distended with diffuse tenderness. Bowel Sounds are hyperactive. Scenario - דוגמא קלאסית של חולה בין 50, כאבי בטן, חוסר מעבר גזים ויציאות. לולאות מעיים מורחבות.

3
Clinical Picture Colicky abdominal pain Abdominal distension Vomiting
Decreased passage of stool or flatus Typical radiographic picture plain AXR, contrast CT, UGI/SBFT, enteroclysis בדרך כלל הבטן תפוחה. במידה והחסימה יותר פרוקסימלית יהיו הקאות. יכול להיות חסימת מעיים שתהיה בה מעבר של צואה. אך חוסר יציאות

4
Paralytic vs Mechanical Ileus Obstruction
Gas diffusely through intestine, incl. colon May have large diffuse Air/fluid levels Quiet abdomen No obvious transition point on contrast study Distended small bowel loops, no air in colon Laddered Air/fluid levels Active peristalsis, quiet= late Obvious transition point on contrast study יש איליום פאראליטי- יש חוסר מעבר גזים וכו'.. אך אין חסימה. חסימה מכנית מטפלים כירורגית בחסימה פאראליטית אין הטיפול ניתוחי. ויש להחליט האם מדובר האחד מהשניים. יש כמה רמזים: באיליום פאראליטי- יש שיתוק של המעיים וזה משפיע על הכל. חסימה מכנית תהיה באופן ספציפי- במקום תפוח ואחריו לא. בדרך כלל הבטן והפרסטלטיקה והאזנה לא נשמע גלים: באיליום פאראליטי – בשלב הראשון זה תומך באיליום פאראליטי. בחסימה מכנית תהיה נקודה של חסימה. אך בבאיליום פאראליטי זה יכול להגיע עד קצה מערכת עיכול.

5
Mechanical Obstruction

7
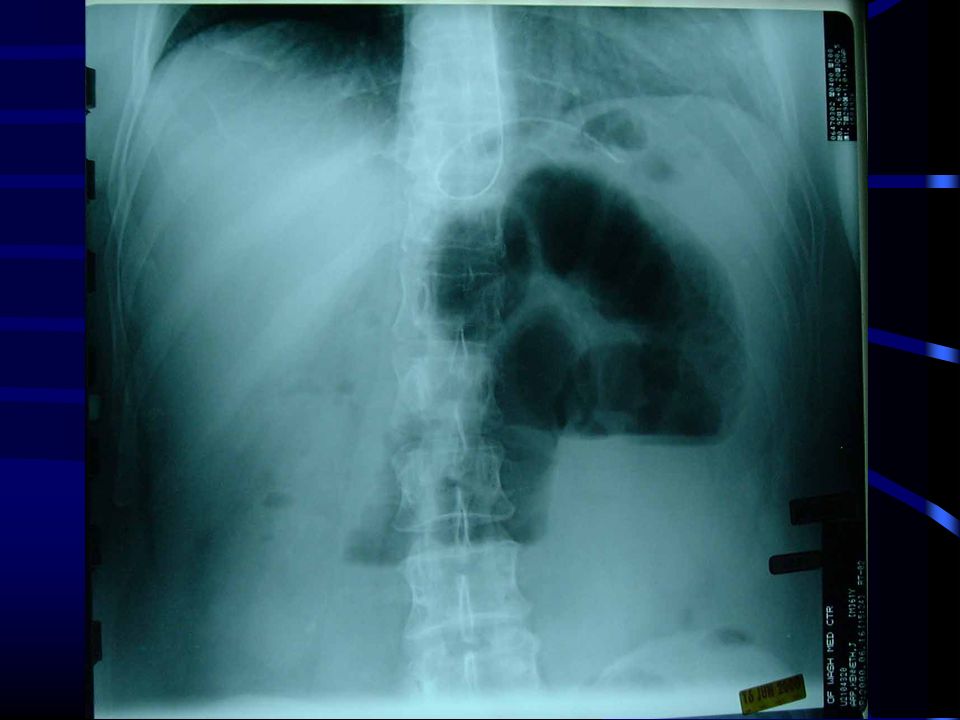
Upright Abdominal Film
Air - Fluid Levels Dilated Small Bowel פלסי אוויר נוזלים נובעים מכך שחסימת מעיים יש אוויר במעי דק בגלל שהאוויר לא נספג והגבול בין האוויר והנוזל נוצר בעמידה של חולה. זה אופייני לחסימת מעי דק. בדרך כלל יש אוויר במעי גס ובקיבה אך בחסימה גם במעי הדק.

8
Adynamic Ileus

9
Example of ileus

10
Pathophysiology I Hypercontractility--hypocontractility
Massive fluid losses: Vomiting sequestration of fluid into the lumen from the surrounding circulation Lymphatic and venous congestion resulting in oedematous tissues - oliguria, hypotension, hemoconcentration Electrolyte depletion פתופיזיולוגיה: יש מספר דברים שעוברים בו זמנית בחסימת מעיים. כל הנזולים צריכים להגיע לקולון ולהיספג שם. ברגע שמעי מפסיק להתגבר על החסימה ... אם החסימה גבוה- איבוד נוזלים- הקאות. אם יש תפיות יש עליה בלחץ יש פגם בהחזר לימפתי. יש בצקת. דופן מעיים מתחילה ליזול נוזל שנשפך לחלל הבטן. יש איבוד נוזלים מאסיבי. זה גורם לאי ספיקת כליות ולסמני הלם. בחסימת מעיים הולך לאיבוד נוזלים ואלקטרוליטים.

11
Pathophysiology II bowel distension--increased intraluminal pressure--impediment of venous return--arterial insufficiency--bowel wall ischemia --necrosis- -perforation--peritonitis and sepsis Bacterial over growth with translocation of bacteria and it’s toxins causing bacteraemia and septicaemia. מנגנון בעייתי שני: נגרם על ידי תפיחות מעי- יש עליה בלחץ זה פוגע בתת כלי דם – לימפה וורידים- יהיה גודש ורידי במעי. לחץ זה גורם לפגיעה באספקת דם ואז תהיה אסיכמיה. הקוטר מקסימלי שנשמר אספקת דם והוא 5 ס"מ. קולון ימני זה... יכול להיות נמק של הדופן, פרפורציה וזיהום וכו'... המעי הדק הוא בעל תוכן סטרילי אך שיש סטאזיס יש גדילה של חיידקים ואותם חיידקים מתחילים להתפתח במעי הדק והם חודרים לתוך חלל הפריטונאום ואז יש זיהום.

12
Important Questions Site Etiology Partial vs. complete
Simple vs. strangulated Fluid & electrolyte status Operative vs. non-operative management הטיפול צריך להיות מהיר: יש כמה נושאים קריטיים: מיקום החסימה והסביה. האם זה חלקי או מלא. נושא נוסף האם זו חסימה בלבד או גם מכנית וגם פגיעה באספקת דם. נושא חשוב נוסף מה מידת איבוד הנוזלים. לכן אם המצב קריטי נצטרך לטפל בנוזלים לפני ניתוח. ומה הטיפול האם טיפול שמרני או לא.

13
May occur at any point in length of small bowel
Site – Small Bowel מיקום: חסימת מעי דק ואו חסימת מעי גס. במעי הדק יש מספר תסמונות מסוג זה. הםא הז חסימה פרוקסימאלית או באמצע, או חסימה דיסטלית. חסימה פרוקסימאלית היא בעיקר הקאות אם היא פרוקסימלית. יש יצירה של 5 ליטר ואם אין מעבד בג'גונום יהיו הקאות. הבטן לא תהיה תפוחה והכלים לא יהיו בולטים. התמונה השולטת במעי הדק היא כאבי בטם- במיד גאט. כאב קרשנדו. הבטן תפוחה אך לא קיצוני. הקאות יהיו אך זה לא שולט. חסימה הקרובה לצקום- תהיה דומה לחסימת מעי גס. הקאות פחות בולטות ואם כן אז ההקאה תהיה בגוון צואתי. May occur at any point in length of small bowel

14
Site? Small Bowel vs. Large Bowel
Scenario prior operations, in bowel habits Clinical picture scars, masses/ hernias, amount of distension/ vomiting Radiological studies gas in colon?, volvulus?, transition point, mass (Almost) always operate on LBO, often treat SBO non-operatively להבדיל בין חסימץת מעי דק לגס ובתוך מעי דק. שינוי בהרגלי יציאות- תומך בחיסמת מעי גס. הדבקויות או הצטלקויות בתוך הבטן זה הכי שכיח לסחימת מעי. לכן ניתוח בטן שמאבדים פריטונאום נוצרות הידבקויות שיכולות ליצור חסימות. נעשה הדמייה מכיוון שחסימת מעי גס דורשת תמיד כמעט ניתוח. חסימת מעי דק שמנסים להימנע מניתוח מכיוון שזה יצור הדבקויות וכו'...
 always operate on LBO, often treat SBO non-operatively. להבדיל בין חסימץת מעי דק לגס ובתוך מעי דק. שינוי בהרגלי יציאות- תומך בחיסמת מעי גס. הדבקויות או הצטלקויות בתוך הבטן זה הכי שכיח לסחימת מעי. לכן ניתוח בטן שמאבדים פריטונאום נוצרות הידבקויות שיכולות ליצור חסימות. נעשה הדמייה מכיוון שחסימת מעי גס דורשת תמיד כמעט ניתוח. חסימת מעי דק שמנסים להימנע מניתוח מכיוון שזה יצור הדבקויות וכו ...")
15
Etiology? Outside the wall Inside the wall Inside the lumen
אתיולוגיה: יש 3 קבוצות: חוץ מעי, בתוך דופן המעי, תוך חלל המעי

16
Causes- Small Bowel Extralumina Mural Luminal Postoperative adhesions
Congenital adhesions Hernia Volvulus Neoplastic Abscess (Diverticulitis) lipoma polyps leiyomayoma hematoma lymphoma carcimoid carinoma secondary Tumors Crohns TB Stricture Intussusception Congenital F. Body Bezoars Gall stone Food Particles החיצוני זה השכיח ביותר זה הדבקויות. רובם זה פגיעות משניות לניתוחים קודמיים אך יכול להיות שגם לא למשל דלקת באגן. יש הדבקויות מולדות. סיבה נוספת שכיחה היא בקעים עם תוכלת של מעי בתוכו. או בולבולוס - סיבוב של המעי. הקבוצה השנייה הנדירה יותר היא חסימה עקב פתולוגיה בדופן המעי – בדרך כלל גידולים – קריצינואיד, קרון או TB. והקבוצה השלישית- בתוך המעי- הכי פחות שכיחה זה בזואר- אפרסמון .
 lipoma. polyps. leiyomayoma. hematoma. lymphoma. carcimoid. carinoma. secondary Tumors. Crohns. TB. Stricture. Intussusception. Congenital. F. Body. Bezoars. Gall stone. Food Particles. החיצוני זה השכיח ביותר זה הדבקויות. רובם זה פגיעות משניות לניתוחים קודמיים אך יכול להיות שגם לא למשל דלקת באגן. יש הדבקויות מולדות. סיבה נוספת שכיחה היא בקעים עם תוכלת של מעי בתוכו. או בולבולוס - סיבוב של המעי. הקבוצה השנייה הנדירה יותר היא חסימה עקב פתולוגיה בדופן המעי – בדרך כלל גידולים – קריצינואיד, קרון או TB. והקבוצה השלישית- בתוך המעי- הכי פחות שכיחה זה בזואר- אפרסמון .")
17
Common Causes SBO הסיבה השכיחה ביותר זה הדבקויות. אחריה זה הרניות. גידולים.חולה ללא ניתוח קודם נחשוב על גידול וזה בדרך כלל אינדקציה של ניתוח.

18
Small Bowel Adhesions Account for 60-70% of All SBO
Result from peritoneal injury, platelet activation and fibrin formation. Associated with starch covered gloves, intraperitoneal sepsis, haemorrhage and foreign bodies. As early as 4 weeks post laparotomy. The majority of patients present between 1-5 years Colorectal Surgery 25% Gynaecological % Appendectomy % 70% of patients have a single band Patients with complex bands are more likely to be readmitted Readmission in surgically treated patients is 35% כל תהליך בחלל הבטן גורם להצטלקות – יש תהליך תגובתי של ייצור פצע. וכל חתך יכול לגרום להצטלקות. תהליך דלקתי בחלל הבטן. דימום אחרי טראומה עם שטף דם. הן נוצרות מהר (הדבקויות) נהפכות לפיברוטיות ובגיל מבוגר יכול להיות חסימה. ניתוחי מעי גס, גניקולוגים, כריתת תוספתן- הם הגורמים להדבקויות – שכיחים ביותר. יכול להיות ניתוח בודד שיגרום לכך- חסימה מעיים. ננסה לתת לזה להפתח ללא נתוח
 נהפכות לפיברוטיות ובגיל מבוגר יכול להיות חסימה. ניתוחי מעי גס, גניקולוגים, כריתת תוספתן- הם הגורמים להדבקויות – שכיחים ביותר. יכול להיות ניתוח בודד שיגרום לכך- חסימה מעיים. ננסה לתת לזה להפתח ללא נתוח.")
19
Hernia Accounts for 10% of SBO Commonest 1. Femoral hernia 2. Inguinal
3. Umbilical 4. Others: Incisional and Internal H. The site of obstruction is the neck of the hernia The compromised viscus is within the sac. Ischaemia occurs initially by venous occlusion, followed by oedema and arterial compromise. Strangulation is noted by: Persistent pain Discoloration Tenderness Systemic symptoms כשיש בקע, נכנסת לולאת מעי לשם- אינקרצניה. המעי הולך ותופח ואז כליאה של תוכן הבקע ואז יהיה בקע ופרפורציה. הנפוץ ביותר זה הרניה מפשעתית. אינקלוציה- זה כניסה של מעי. סטרגולציה- אין כניסה של דם והמעי כלוא. חסימה בצוואר השבר.

20
Other causes Intussusception Gall stone Ileus IBD Intussusception
יכול להיגרם לחסימה. אבן מרה יכולה לגרום לעבור למערכת העיכול ואז תהיה חסימה. Intussusception Gall stone Ileus IBD

21
Common Causes of LBO Colon cancer Diverticulitis Volvulus Hernia
Unlike SBO, adhesions very unlikely to produce LBO frequency במעי גס הסיבה השכיחה לחסימה זה גידול. יש גם שכיחות של דרטיקולי. ולולווס בסגמואיד יכול להיות הסתובבות. גם בקע יכול להיות. הדבקויות בדרך כלל לא גורמות לחסימה של המעי הגס בגלל שהוא מקובע.

22
Sigmoid Volvulus Colonic Obstruction

23
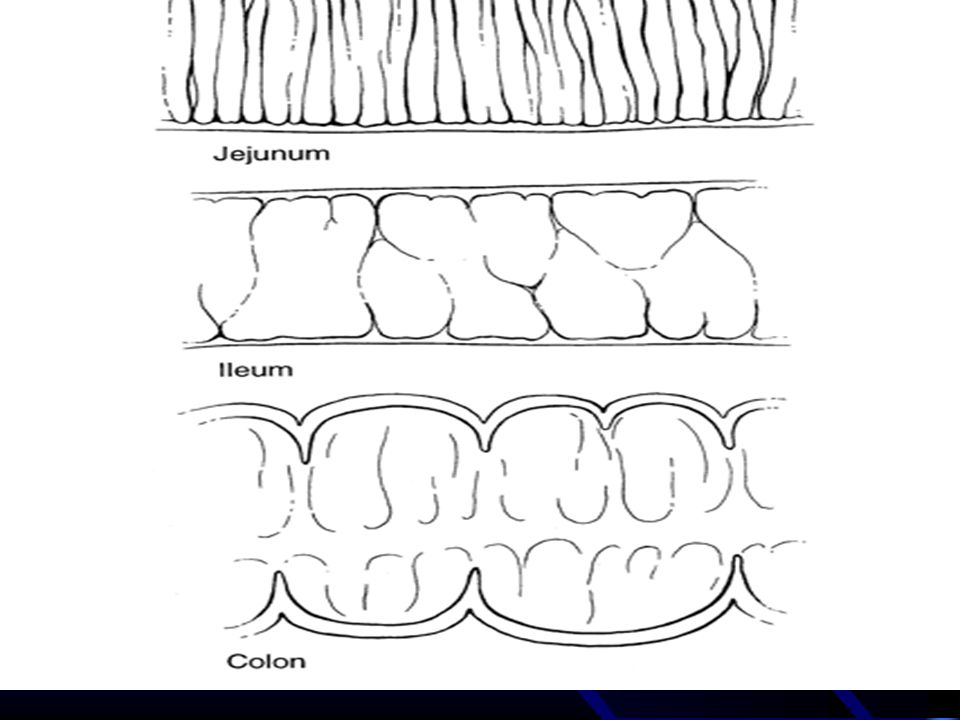
The Difference between small and large bowel obstruction
Small Bowel Large bowel Central ( diameter 5 cm max) Vulvulae coniventae Peripheral ( diameter 8 cm max) Presence of haustration יש הבדל הוא במיקום. לולאות מורחבות במרכז הבטן. במעי הגס זה בהיקף. ההבדל הוא באאוסטרות לעומת פסים צרים של המעי וזה לינאה קולבנטס.
 Vulvulae coniventae. Peripheral ( diameter 8 cm max) Presence of haustration. יש הבדל הוא במיקום. לולאות מורחבות במרכז הבטן. במעי הגס זה בהיקף. ההבדל הוא באאוסטרות לעומת פסים צרים של המעי וזה לינאה קולבנטס.")
25
Partial vs Complete Flatus
Residual colonic gas above peritoneal reflection Adhesions 60-80% resolve with non-operative Tx Must show objective improvement, if none by 48h consider OR Complete obstipation No residual colonic gas on AXR SBFT may differentiate early complete from high-grade partial Almost all should be operated on within 24h האם מדובר בחלקית או מלאה? חלקית זה יותר אופייני בהדבקויות התמונה פחות דרמטית רובם נית ןלטפל ללא ניתוח יש מעבר גזים בדרך כלל. בתמונה של חסימה מלאה. הטיפול יהיה יותר אגרסיבי ואם אין שיפור יהיה ניתוח.

26
Is there strangulation?
4 Cardinal Signs fever, tachycardia, localized abdominal tenderness, leukocytosis 0/4 0% strangulated bowel 1/4 7% “ “ 2-3/4 24% “ “ 4/4 67% “ “ process accelerated with closed-loop obstr. חשוב לדעת האם המעי חיוני או לא. התמותה של ניתוח בגלל חסימת מעיים עם נמק יכולה להיות 20% בניגוד למצב שיש מעי שאינו נמקי שאחוזי הסיכון נמוכים ביותר. ההחלטה הזו קריטית לטיפול. יש סמנים של ספסיס באיסכמיה של מעי אך אם אין איסכמיה לא יהיה סמנים אלו. אם יש אסיכמיה- טיפול אגרסיבי. סמנים: טכיקראדיםה, חום, לויקוציטוזיס, פריטוניטיס. זה מדדי ספסיס. אם אין את זה הסיכון נמוך מאוד.

27
Role of CT Used with IV contrast, oral and rectal contrast (triple contrast). Able to demonstrate abnormality in the bowel wall, mesentery, mesenteric vessels and peritoneum. It can define Level of obstruction Degree of obstruction Cause: volvulus, hernia, luminal and mural causes The degree of ischaemia Free fluid and gas Ensure: patient vitally stable with no renal failure and no previous allergy to iodine היום משתמשים באמצעי עזר כדי לדעת האם יש חסימת מעי. חסימה בשתי מקודות close loop obstruction. יש לולאת הרניה כשיש חסימה ולא רק בכניסה אין שסתום לחץ כמו בחסימה מצד אחד. זו חסימה סגורה. וזה גורם לעליית לחץ מהירה בחלל. והפגיעה יותרמהירה ולכן סטרוגלוציה היא מהירה יותר במצב זה. גם וולולוס נותן תמונה- יש סיבוב גם של כלי דם בנוסף למעי. הפגיעה הזאת כפולה גם חסימה גם איסכמיה וגם בעיה באספקת הדם. CT עוזר עושים – חומר ניגוד בוריד, חוקן ושתיה. ניתן לראות את גובה החסימה. דבר נוסף הוא פגיעה באספקת הדם- עוזר לנו CT. נראה הםא המעי חיוור ונוכל לראות זאת וזה חשד לנמק של המעיים.

28
Pneumatosis Intestinalis Dilated Loops of SB Air in Wall of SB
No Air in Colon Pneumatosis Intestinalis פגיעה בדופק המעי בגלל נמק. יש כניסה של אוויר.

29
Role of barium& gastrografin studies
As: UGI with follow through, enema Gastrografin is used in acute abdomen but is diluted Useful in recurrent and chronic obstruction May be able to define the level and mural causes. Can be used to distinguish between adynamic and mechanical obstruction Barium should not be used in a patient with peritonitis ניתן להשתמש בחומר עם ניגוד. הבעיה עם הבריום שהוא יכול לעבור לתוכן הבטן והוא רעיל. ניתן להגדיר את מקום החסימה והאם היא מלאה או לא. ניתן להבדיל הםא מדובר האיליום פאראליטי לעומת חסימה מעיים מכנית.

30
Causes of Adynamic Ileus
Following celiotomy small bowel- 24h, stomach- 48h, colon- 3-5d Inflammation e.g. appendicitis, pancreatitis Retroperitoneal disorders e.g. ureter, spine, blood Thoracic conditions e.g. pneumonia, # ribs Systemic disorders e.g. sepsis, hyponatremia, hypokalemia, hypomagnesemia Drugs e.g opiates, Ca-channel blockers, psychotropics מצב שכיח לאחר פתיחת בטן איליוס פאראליטי. כל פתיחת בטן תגרום לשיתוק זמני של האיליום. מצב של איליוס פאראליטי זה פיזיולוגי לאחר כל ניתוח וזה המצב השכיח ביותר. גם מצב דלקתי או פתולוגיה בעמ"ש יכול להגרום לפגיעה עצבית ויהיה איליוס פאראליטי. יש גם בעיות סיסטמיות – היפוקלמיה , היפומגנזמיה. גם אופיטיים יכולים לגרום לכך.

31
Management of Bowel Obstruction
NEVER LET THE SUN RISE OR FALL ON A PATIENT WITH BOWEL OBSTRUCTION בגלל שיש חשש לנמק של המעי- נותנים טיפול שמרני ואם 24 שעות אין שיפור גישה ניתוחית.

32
Principles Fluid resuscitation Electrolyte, acid-base correction
Close monitoring foley, central line NGT decompression Antibiotics controversial TO OPERATE OR NOT TO OPERATE

33
Resuscitation Massive third space losses as fluid and electrolytes accumulate in bowel wall and lumen Depending on site and duration Proximal - vomiting early, with dehydration, hypochloremia, alkalosis distal- more distension, vomiting late, dehydration profound, fewer electrolyte abnormalities Requirements = DEFICIT + MAINTENANCE + ONGOING LOSSES

34
When is it safe NOT to operate?
SMALL bowel obstruction if adhesions suspected etiology i.e. CANNOT have a “virgin” abdomen No signs of strangulation Adynamic ileus

35
Operative Indications
Incarcerated or strangulated hernia Peritonitis Pneumopertioneum Suspected strangulation Closed loop obstruction Complete obstruction Virgin abdomen LARGE bowel obstruction

36
Case 1 82yo man /c CHF and Hairy Cell Leukemia. Presents to the ER /c dx of appendicitis. Taken to the OR for uncomplicated laparoscopic appendectomy. POD #2 - progressive abdominal distention with postop ileus POD#3 - bilious emesis - afeb, nontender abd, wcc 5000

38
Case 1 POD#5 - Abdomen distended - High NGT output
- No classic signs of strangulation

40
Outcome 1 Taken to OR for laparoscopic exploration evening of POD#5
Findings: Suture at umbilical Hasson trocar site had broken (knot intact) Richters hernia Proximal bowel viable but congested Peristalsis, doppler signal and Wood’s lamp all negative for ischemic injury
 Richters hernia. Proximal bowel viable but congested. Peristalsis, doppler signal and Wood’s lamp all negative for ischemic injury.")
41
Case 2 60yo M s/p R hemicolectomy 9/99 for cancer. Presents with 3d of intermittent crampy epigastric pain, distension, n/v. 3 “normal” BMs in 24 hours. PE: T / Absent BS, soft, distended abdomen with periumbilical tenderness. No rebound or guarding. No palpable hernias. Well healed scars. Labs: WBC 15.7, Hct 48, HCO3 28 nl LFTs and amylase Negative UA

44
Outcome 2 NGT placed, fluid resuscitated.
Given high grade obstruction on AXRs, and leukocytosis patient taken to OR within 24 hours. On laparotomy, multiple dense adhesions found with tight band in retroperitoneum causing internal hernia/obstruction with a transition point. Adhesiolysis performed.

45
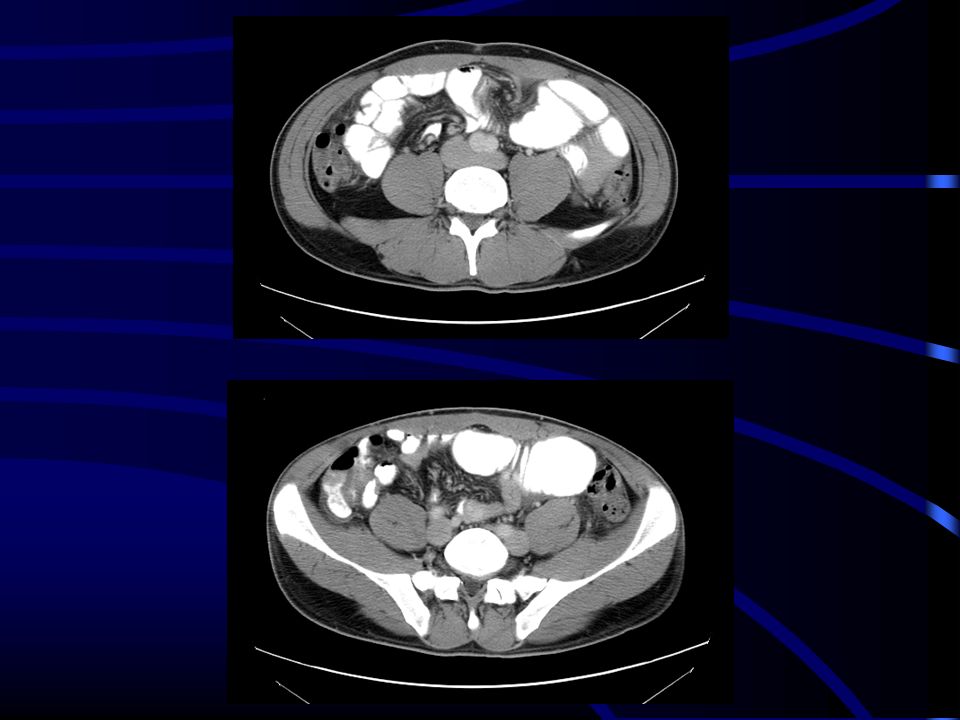
Case 3 79yo F with Parkinson’s disease and h/o breast cancer 20 yr ago presents to with 4d h/o n/v, distension. No abd pain. Reports recent bowel movement PE: Afebrile BP157/74 P89 Hard palpable mass in RUQ. Distended abdomen, high pitched BS, no tenderness. No palpable hernias. No scars. Black stool. Labs: WBC Hct Cr 0.7 LFT’s wnl

49
Outcome 3 Operative exploration given RUQ mass, abd CT demonstrating distended small bowel and decompressed colon, with multiple masses in the RUQ and pelvis. On laparotomy, large RUQ mass involving multiple loops of small and large bowel, and mass in R pelvis requiring small and large bowel partial resections. Pathology lobular adenocarcinoma. Regained bowel function POD 5.

50
Case 4 32 ym, former athlete Ex lap for ruptured appendix 1997
Non-operative management partial SBO 2002 Presents to ER four months later w/ diffuse abdominal pain and distension PE: T 36.5, HR 75, mild periumbilical tenderness, no peritonism, midline scar, reducible LIH Labs: WCC 13.5, HCO3 25, other labs WNL

53
Outcome 4 NGT placed Fluid resuscitated
Non-operative management for 3days Laparoscopic operative exploration with lysis of adhesions. No bowel compromise. Discharged POD #2

Similar presentations