Download presentation
Presentation is loading. Please wait.

1
Important Highlights from The ACC Annual Meeting, March 29-31, 2014 Mohammed Fakhry AbdulMohsen, MD, MESC, FACC Professor of Medicine and Cardiology, At College of Medicine, UOD Consultant Internist/Cardiologist, King Fahd Hospital of the University April 21, 2014

2
1. Bariatric Surgery vs. Intensive Medical Therapy in Obese Diabetic Patients: 3-Year Outcomes Philip R Schauer, Deepak L Bhatt, John P Kirwan, Kathy Wolski, Stacy A Brethauer, Sankar D Navaneethan, Ali Aminian, Claire E Pothier, Ester SH Kim, Steve E Nissen, and Sangeeta R Kashyap STAMPEDE investigators Cleveland Clinic Bariatric and Metabolic Institute Endocrinology, Diabetes and Metabolism Results of the STAMPEDE Trial

3
STAMPEDE Trial 1. STAMPEDE Trial Background Background T2DM affects over 25 million individuals in the US, but < 50% of patients achieve adequate glycemic control on current pharmacotherapy.T2DM affects over 25 million individuals in the US, but < 50% of patients achieve adequate glycemic control on current pharmacotherapy. Observational studies show improvement in glycemic control and CV risk factors following bariatric surgery.Observational studies show improvement in glycemic control and CV risk factors following bariatric surgery. Short-term (1-2 yrs.) RCTs, including the 1 year data of the STAMPEDE trial demonstrated remission of T2DM following bariatric surgery*.Short-term (1-2 yrs.) RCTs, including the 1 year data of the STAMPEDE trial demonstrated remission of T2DM following bariatric surgery*. However, no long-term (>3 yrs) RCT data exist to compare the durability of bariatric surgery vs medical therapy for T2DM control.However, no long-term (>3 yrs) RCT data exist to compare the durability of bariatric surgery vs medical therapy for T2DM control.
 RCTs, including the 1 year data of the STAMPEDE trial demonstrated remission of T2DM following bariatric surgery*.Short-term (1-2 yrs.) RCTs, including the 1 year data of the STAMPEDE trial demonstrated remission of T2DM following bariatric surgery*. However, no long-term (>3 yrs) RCT data exist to compare the durability of bariatric surgery vs medical therapy for T2DM control.However, no long-term (>3 yrs) RCT data exist to compare the durability of bariatric surgery vs medical therapy for T2DM control..")
4
STAMPEDE Trial 1. STAMPEDE Trial Objectives Objectives 1)Compare the durability of bariatric surgery vs medical therapy with respect to: Achieving biochemical resolution of T2DM Achieving biochemical resolution of T2DM 2) Compare differences between types of surgery
Compare the durability of bariatric surgery vs medical therapy with respect to: Achieving biochemical resolution of T2DM Achieving biochemical resolution of T2DM 2) Compare differences between types of surgery.")
5
STAMPEDE Trial 1. STAMPEDE Trial Endpoints EndpointsPrimary: Success rate of achieving HbA1c ≤ 6% Secondary: Change in fasting plasma glucose (FPG) Change in fasting plasma glucose (FPG) Change in lipids, blood pressure, BMI Change in lipids, blood pressure, BMI Change in carotid intimal medial thickness Change in carotid intimal medial thickness Change in medications Change in medications Safety and adverse events Safety and adverse events Quality of Life Quality of Life
 Change in fasting plasma glucose (FPG) Change in lipids, blood pressure, BMI Change in lipids, blood pressure, BMI Change in carotid intimal medial thickness Change in carotid intimal medial thickness Change in medications Change in medications Safety and adverse events Safety and adverse events Quality of Life Quality of Life.")
6
STAMPEDE Trial 1. STAMPEDE Trial Intensive Medical Therapy: Wt. management with diet and lifestyle. Wt. management with diet and lifestyle. Antihyperglycemic agents and multiple insulin injections utilized to target HbA1c ≤6% Antihyperglycemic agents and multiple insulin injections utilized to target HbA1c ≤6% Scheduled visits with nutrition, psychology and endocrinology per protocol Scheduled visits with nutrition, psychology and endocrinology per protocol

7
Bariatric Surgery Roux-en-Y Gastric Bypass Sleeve Gastrectomy Roux-en-Y Gastric Bypass Sleeve Gastrectomy Kashyap S, Schauer P, Bhatt D; Diabetes Obesity Metabolism2010 Sep;12(9):833
:833")
8
218 patients screened 50 Intensive medical therapy alone 50 Medical therapy plus sleeve gastrectomy Population for 3-Year Analysis 40 48 49 150 randomized STAMPEDE Trial: Flow of Patients 50 Medical therapy plus gastric bypass 1 withdrew consent prior to surgery 8 withdrew consent 2 Lost to follow-up HbA1c >7.0%HbA1c >7.0% BMI 27- 43 kg/m 2 BMI 27- 43 kg/m 2 Age 20-60 years Age 20-60 years 91% retention 2 Lost to follow-up

9
Baseline Characteristics Parameter Medical Therapy (n=40) Bypass (n=48) Sleeve (n=49) Age (yrs) 50.348.047.8 Females67%58%78% Duration of diabetes (yrs) 8.88.08.3 HbA1c (%) 9.09.39.5 Body Mass Index (kg/m 2 ) 36.437.136.1 ≥ 3 diabetes medications 61%52%46.9% Insulin use 51.2%46%44.9% Depression32%37%46% Microvascular complications 20%42%29% Note: Based on analyzed population
 Bypass (n=48) Sleeve (n=49) Age (yrs) Females67%58%78% Duration of diabetes (yrs) HbA1c (%) Body Mass Index (kg/m 2 ) ≥ 3 diabetes medications 61%52%46.9% Insulin use 51.2%46%44.9% Depression32%37%46% Microvascular complications 20%42%29% Note: Based on analyzed population")
10
Primary and Secondary Endpoints at 36 Months Parameter Medical Therapy (n=40) Bypass (n=48) Sleeve (n=49) P Value 1 P Value 2 HbA1c ≤ 6% 5%37.5%24.5%<0.0010.012 (without DM meds) 0%35.4%20.4%<0.0010.002 HbA1c ≤ 7% 40%64.6%65.3%0.020.02 Change in FPG (mg/dL) -6-85.5-460.0010.006 Relapse of glycemic control 80%23.8%50%0.030.34 % change in HDL +4.6+34.7+35.0<0.001<0.001 % change in TG -21.5-45.9-31.50.010.01 % change in CIMT 0.0480.0130.0170.360.49 1 Gastric Bypass vs Medical Therapy; 2 Sleeve vs Medical Therapy
 Bypass (n=48) Sleeve (n=49) P Value 1 P Value 2 HbA1c ≤ 6% 5%37.5%24.5%< (without DM meds) 0%35.4%20.4%< HbA1c ≤ 7% 40%64.6%65.3% Change in FPG (mg/dL) Relapse of glycemic control 80%23.8%50% % change in HDL <0.001<0.001 % change in TG % change in CIMT Gastric Bypass vs Medical Therapy; 2 Sleeve vs Medical Therapy")
11
Change in HbA1c Change in HbA1c (%) P<0.001 Medical Sleeve Gastric Bypass Medical Sleeve Gastric Bypass
 P<0.001 Medical Sleeve Gastric Bypass Medical Sleeve Gastric Bypass")
12
Change in Body Mass Index Change in BMI (Kg/M 2 ) P=0.006 P<0.001 Medical Sleeve Gastric Bypass Medical Sleeve Gastric Bypass
 P=0.006 P<0.001 Medical Sleeve Gastric Bypass Medical Sleeve Gastric Bypass")
13
Percentage of Patients on Insulin % Patients Medical525444404755 Gastric Bypass462510476 Sleeve45166898 Medical525444404755 Gastric Bypass462510476 Sleeve45166898 Medical Sleeve Gastric Bypass Medical Sleeve Gastric Bypass

14
Cardiovascular Medications at Baseline and Month 36 CV medications number (%) number (%) Medical Therapy (n=40) Bypass (n=48) Sleeve (n=49) Baseline None 0 (0) 3 (6.3) 2 (4.1) 1 - 2 19 (47.5) 17 (35.4) 28 (57.1) > 3> 3> 3> 3 21 (52.5) 28 (58.3) 19 (38.8) Month 36 None 1 (2.5) 33 (68.8) * 21 (42.9) * 1 - 2 18 (45) 14 (29.2) 25 (51) > 3> 3> 3> 3 21 (52.5) 1 (2.1) 3 (6.1) * P value <0.05 with Medical Therapy group as comparator
 number (%) Medical Therapy (n=40) Bypass (n=48) Sleeve (n=49) Baseline None 0 (0) 3 (6.3) 2 (4.1) (47.5) 17 (35.4) 28 (57.1) > 3> 3> 3> 3 21 (52.5) 28 (58.3) 19 (38.8) Month 36 None 1 (2.5) 33 (68.8) * 21 (42.9) * (45) 14 (29.2) 25 (51) > 3> 3> 3> 3 21 (52.5) 1 (2.1) 3 (6.1) * P value <0.05 with Medical Therapy group as comparator")
15
STAMPEDE Trial 1. STAMPEDE Trial Physical Functioning Role Limitations Quality of Life % Physical Health Components

16
Adverse Events through 36 Months Parameter Medical Therapy (n=43) Bypass (n=50) Sleeve (n=49) GI complications 2 (5) 13 (26) 5 (4) Re-op02(4)2(4) Stroke00 1 (2) Retinopathy0 2 (4) Nephropathy 4 (9) 7 (14) 5 (10) Foot ulcers 0 2 (4) 1 (2) Excessive weight gain 7 (16) 00
 Bypass (n=50) Sleeve (n=49) GI complications 2 (5) 13 (26) 5 (4) Re-op02(4)2(4) Stroke00 1 (2) Retinopathy0 2 (4) Nephropathy 4 (9) 7 (14) 5 (10) Foot ulcers 0 2 (4) 1 (2) Excessive weight gain 7 (16) 00")
17
STAMPEDE Trial 1. STAMPEDE Trial Summary Summary Bariatric surgery was more effective than intensive medical therapy in achieving glycemic control (HbA1c < 6.0%) with weight loss as the primary determinant of this outcome.Bariatric surgery was more effective than intensive medical therapy in achieving glycemic control (HbA1c < 6.0%) with weight loss as the primary determinant of this outcome. Many surgical patients achieved glycemic control without use of any diabetic medications (particularly insulin).Many surgical patients achieved glycemic control without use of any diabetic medications (particularly insulin). Metabolic syndrome components (HDL, triglycerides, glucose, BMI) showed greater improvement after surgery.Metabolic syndrome components (HDL, triglycerides, glucose, BMI) showed greater improvement after surgery. Marked improvement in quality of life.Marked improvement in quality of life.
 with weight loss as the primary determinant of this outcome.Bariatric surgery was more effective than intensive medical therapy in achieving glycemic control (HbA1c < 6.0%) with weight loss as the primary determinant of this outcome. Many surgical patients achieved glycemic control without use of any diabetic medications (particularly insulin).Many surgical patients achieved glycemic control without use of any diabetic medications (particularly insulin). Metabolic syndrome components (HDL, triglycerides, glucose, BMI) showed greater improvement after surgery.Metabolic syndrome components (HDL, triglycerides, glucose, BMI) showed greater improvement after surgery. Marked improvement in quality of life.Marked improvement in quality of life..")
18
STAMPEDE Trial 1. STAMPEDE Trial Conclusion Conclusion Bariatric surgery (gastric bypass or sleeve gastrectomy) should be considered as a treatment option for patients with uncontrolled T2DM and moderate to severe obesity (BMI > 30 Kg/M 2 ) with results durable through 3 years of follow up.
 should be considered as a treatment option for patients with uncontrolled T2DM and moderate to severe obesity (BMI > 30 Kg/M 2 ) with results durable through 3 years of follow up..")
19
Highlights from The ACC Annual Meeting, March 27, 2014 2. CoreValve US Pivotal Trial A Randomized Comparison of Self-expanding Transcatheter (TAVR) and Surgical Aortic Valve Replacement in Patients with Severe Aortic Stenosis Deemed High-Risk for Surgery. David H. Adams, MD On Behalf of the US CoreValve Investigators
 and Surgical Aortic Valve Replacement in Patients with Severe Aortic Stenosis Deemed High-Risk for Surgery. David H. Adams, MD On Behalf of the US CoreValve Investigators.")
20
2. CoreValve US Pivotal Trial Background: Many Patients with Symptomatic Severe Aortic Stenosis are not Ideal Candidates for Surgery due to Increased Risks TAVR (TAVI) with a balloon expandable valve improved survival compared to medical therapy in inoperable patients TAVR with a balloon expandable valve had similar survival compared to surgery in patients at high risk for surgery
 with a balloon expandable valve improved survival compared to medical therapy in inoperable patients TAVR with a balloon expandable valve had similar survival compared to surgery in patients at high risk for surgery.")
21
2. CoreValve US Pivotal Trial Study Purpose: To assess the safety and effectiveness of TAVR with the Core Valve ( Self-expanding) prosthesis compared to surgical valve replacement in symptomatic patients with severe aortic stenosis at increased surgical risk.
 prosthesis compared to surgical valve replacement in symptomatic patients with severe aortic stenosis at increased surgical risk..")
22
18Fr delivery system 4 valve sizes (18-29 mm annular range) Transfemoral Subclavian Direct Aortic Study Device and Access Routes 22
 Transfemoral Subclavian Direct Aortic Study Device and Access Routes 22")
23
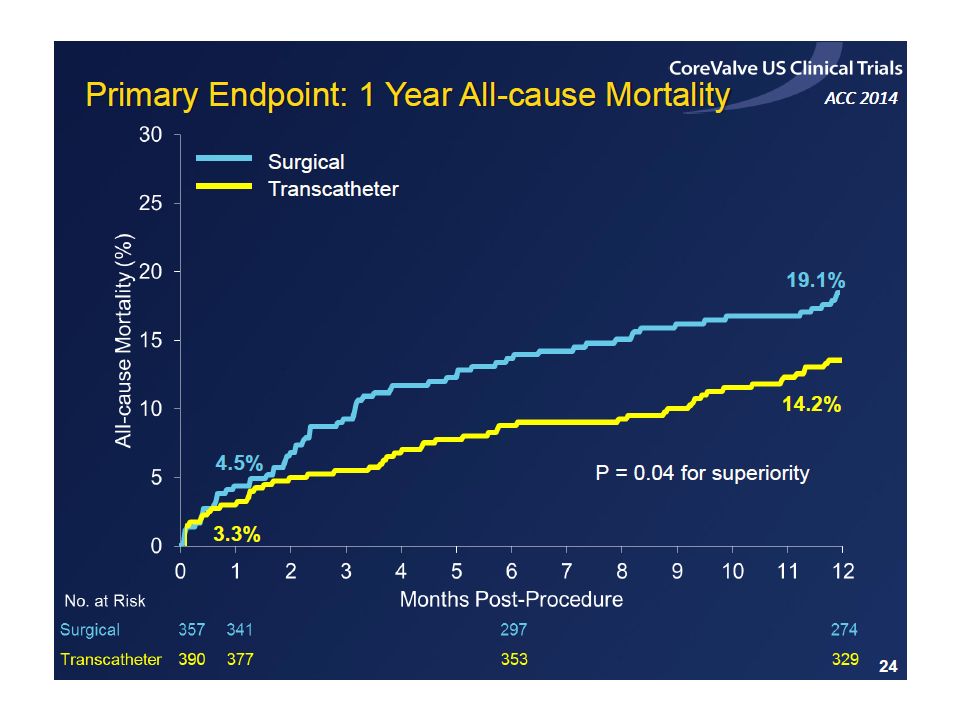
2. CoreValve US Pivotal Trial Primary Endpoint: All-cause mortality at 1 year Non-inferiority Testing: TAVR with the CoreValve prosthesis was non-inferior to SAVR after 1 year for all- cause mortality with a 7.5% non-inferiority margin.

24
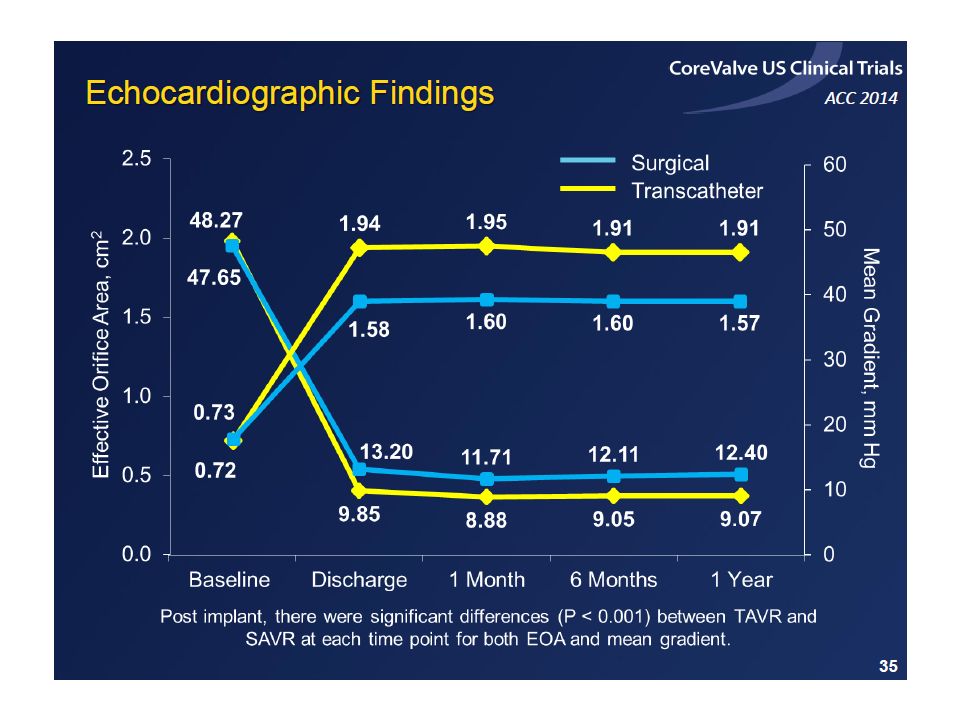
2. CoreValve US Pivotal Trial Secondary Endpoints: Hierarchical (Graded- Categorized) Testing of Secondary Endpoints: Δ mean gradient baseline to 1 year (non-inferior) Δ effective orifice area baseline to 1 year (non-inferior) Δ NYHA class baseline to 1 year (non-inferior)
 Testing of Secondary Endpoints: Δ mean gradient baseline to 1 year (non-inferior) Δ effective orifice area baseline to 1 year (non-inferior) Δ NYHA class baseline to 1 year (non-inferior).")
26
2. CoreValve US Pivotal Trial Inclusion Criteria: NYHA functional class II or greater Severe aortic stenosis: AVA ≤ 0.8 cm 2 or AVAI ≤ 0.5 cm 2 /m 2 AND mean gradient > 40 mm Hg. Risk of death at 30 days after surgery was ≥ 15% and the risk of death or irreversible complications within 30 days was < 50%

27
Study Disposition

28
Characteristic TAVR N=390 SAVR N=357 Age, years 83.1 ± 7.183.2 ± 6.4 Men, % 53.152.4 STS Predicted Risk of Mortality, % 7.3 ± 3.07.5 ± 3.4 Logistic EuroSCORE, % 17.7 ± 13.118.6 ± 13.0 NYHA Class III/IV, %85.686.8 Diabetes Mellitus, % 34.9*45.4* Insulin Requiring Diabetes, % 11.013.2 Prior Stroke, % 12.614.0 STS Severe Chronic Lung Disease, % 13.39.0 Baseline Demographics *P < 0.01 28

36
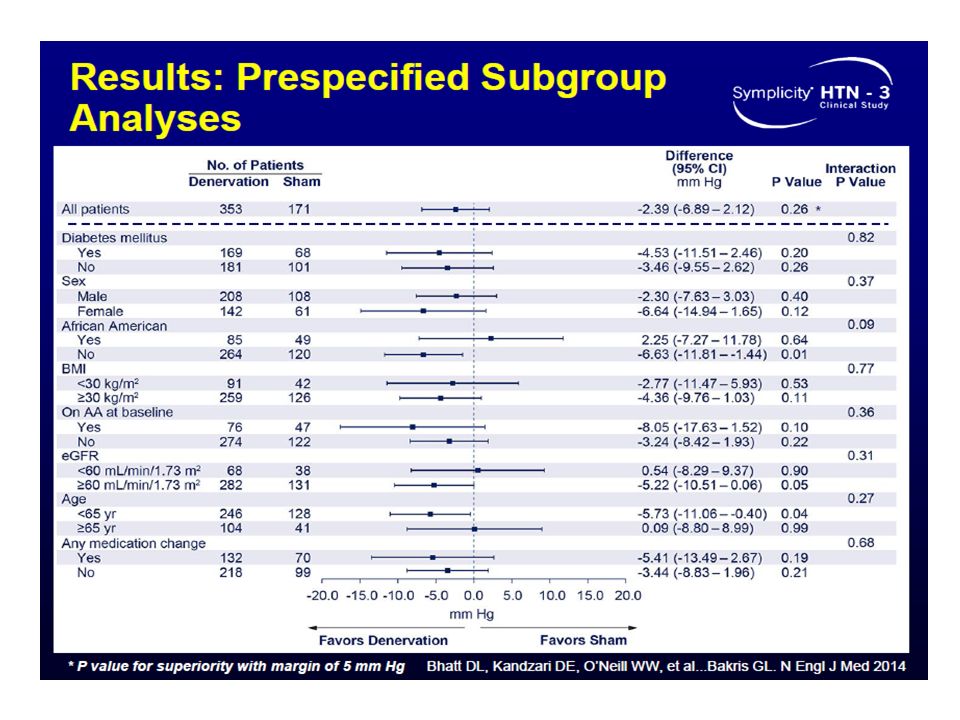
Highlights from The ACC Annual Meeting, March 27, 2014 3. Renal Denervation in Patients with Uncontrolled Hypertension: Results of the SYMPLICITY HTN 3 Trial Deepak L. Bhatt, M.D., M.P.H., David E. Kandzari, M.D., William W. O’Neill, M.D., Ralph D'Agostino, Ph.D., John M. Flack, M.D., M.P.H., Barry T. Katzen, M.D., Martin B. Leon, M.D., Minglei Liu, Ph.D., Laura Mauri, M.D., M.Sc., Manuela Negoita, M.D., Sidney A. Cohen, M.D., Ph.D., Suzanne Oparil, M.D., Krishna Rocha- Singh, M.D., Raymond R. Townsend, M.D., George L. Bakris, M.D., for the SYMPLICITY HTN-3 Investigators

37
SYMPLICITY HTN 3 Trial Background: Hypertension is growing in prevalence worldwide due to aging of the population and prevalence of obesity. Approximately 10% of patients with diagnosed hypertension have “resistant” hypertension. The sympathetic nervous system appears to play an important role in resistant hypertension. Prior non-blinded studies have suggested that catheter-based renal artery denervation reduces BP in resistant hypertension.

38
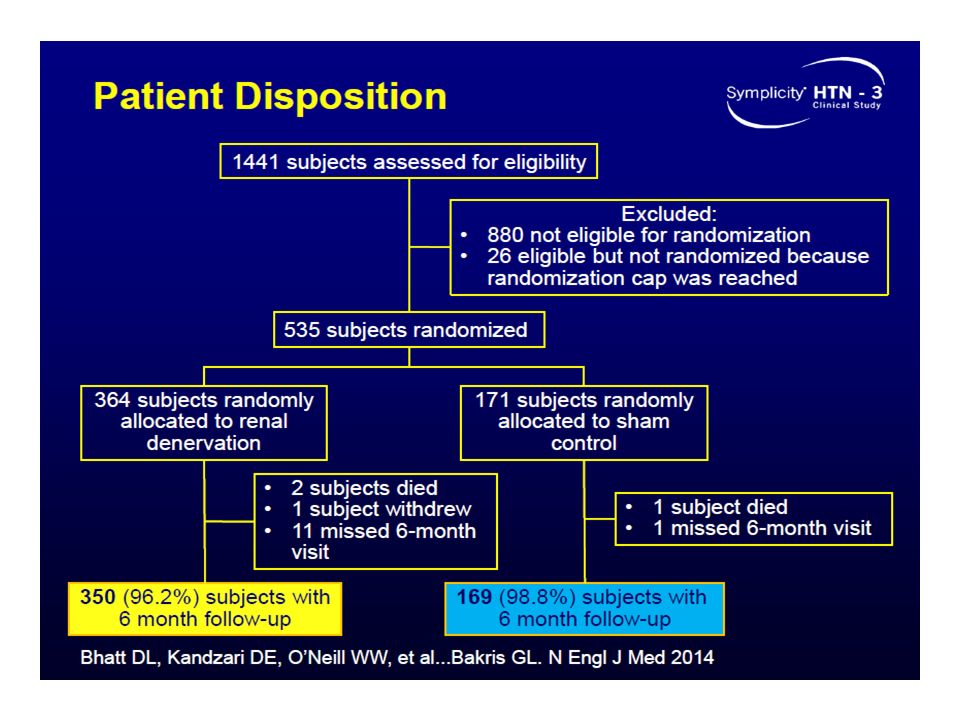
SYMPLICITY HTN 3 Trial Trial Objectives: SYMPLICITY HTN-3 is the first prospective, multi-center, randomized, blinded, sham controlled study to evaluate both the safety and efficacy of percutaneous renal artery denervation in patients with severe treatment-resistant hypertension. The trial included 535 patients enrolled by 88 participating US centers.

39
SYMPLICITY HTN 3 Trial

40
Inclusion Criteria: Age ≥18 and ≤80 years. Stable medication regimen including full tolerated doses of ≥3 antihypertensive medications of different classes, including a diuretic. Office SBP ≥160 mm Hg based on an average of 3 BP readings. Written informed consent

41
SYMPLICITY HTN 3 Trial Exclusion Criteria: ABPM 24 hour → average SBP <135 mm Hg eGFR of <45 mL/min Main renal arteries <4 mm diameter or <20 mm treatable length Renal artery stenosis >50% or aneurysm in either renal artery History of prior renal artery intervention

42
SYMPLICITY HTN 3 Trial Primary Endpoints: 1. The rate of the Major Adverse Events (MAE) in the treatment group compared with an Objective Performance Criterion (OPC=9.8%) 2. MAE was defined as all-cause mortality, end stage renal disease, embolic event resulting in end-organ damage, renal artery or other vascular complication, hypertensive crisis through 30 days, or new renal artery stenosis within 6 months.
 in the treatment group compared with an Objective Performance Criterion (OPC=9.8%) 2. MAE was defined as all-cause mortality, end stage renal disease, embolic event resulting in end-organ damage, renal artery or other vascular complication, hypertensive crisis through 30 days, or new renal artery stenosis within 6 months..")
52
“Our Lord, Let Not Our Hearts Deviate After You Have Guided Us, and grant us mercy from You. Truly, You are the Best Granter.” Surat A`L Imran; verse 8 « رَبَّنَا لاتُزِغْ قُلوبَنَا بعْدَ إذْ هَدَيْتَنَا وهَبْ لَنَا مِنْ لَّدُنْكَ رَحْمَةً إنَّكَ أنْتَ الوَهَّاب » سورة آل عمران : آية 8 صدق الله العظيم

Similar presentations









>")
















