Download presentation
Presentation is loading. Please wait.

1
High Risk TIA: Identification and Management Carolyn Walker RN. BN January 2011

2
High Risk TIA: Identification and Management Learning Objectives: Upon completion of this session, participants will be able to: 1. Identify clinical predictors of stroke following a transient ischemic attack 2. Describe how neurovascular imaging may assist to identify those patients at increased risk of stroke following a transient ischemic attack. 3. Describe the appropriate management of a high risk TIA patient

3
What is a TIA? Definition: Acute episode of neurologic symptoms lasting < 24 hr Proposed tissue based definition: Rapidly resolving neurologic symptoms, typically lasting <1 hour, with no evidence of infarction on MRI (DWI) (Albers et al. New Engl J Med; 2002; 347: 1713-1716) 40% - 60% of TIA patients have ischemic injury on DWI (Ay et al. Cerebrovasc Dis; 2002; 14: 177-186)
 (Albers et al. New Engl J Med; 2002; 347: ) 40% - 60% of TIA patients have ischemic injury on DWI (Ay et al. Cerebrovasc Dis; 2002; 14: ).")
4
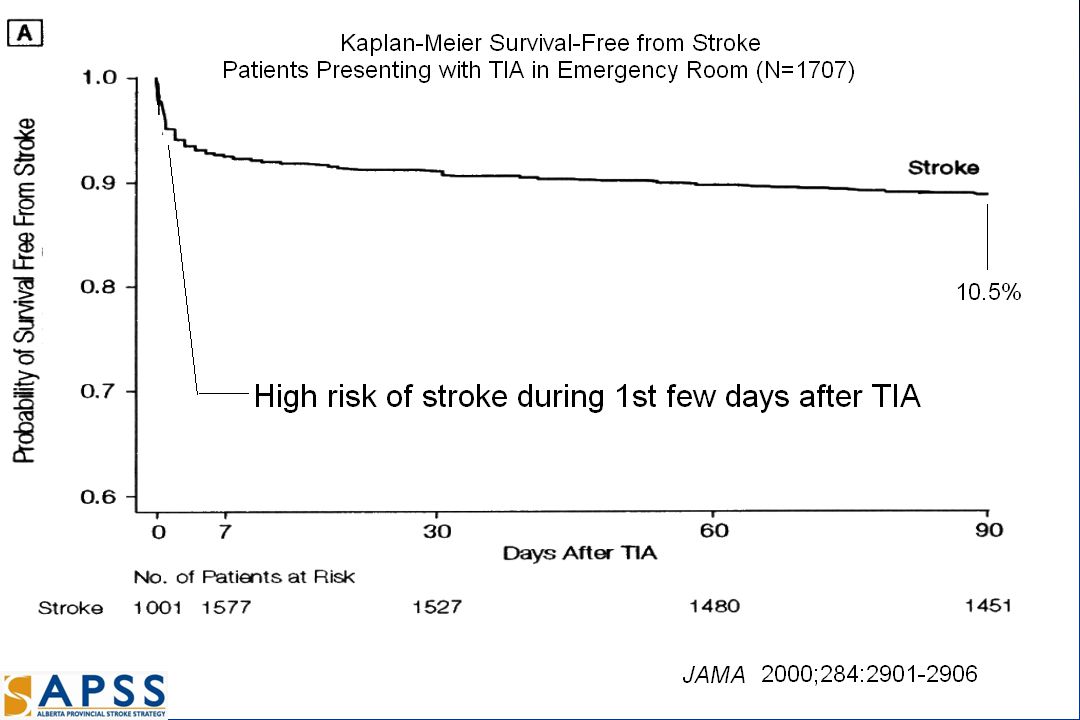
TIA Stroke Risk Risk of stroke following TIA is high: 10-20% within 90 days 10-20% within 90 days 50% of these within the first 2 days (48 hours) 50% of these within the first 2 days (48 hours) Johnston et al. JAMA 2000; 284: 2901-06 ~ 20%-40% of strokes are preceded by a TIA or non disabling stroke (Rothwell et al. Lancet Neurol 2006; 5: 323-331) Golden Opportunity for Stroke Prevention!
 Golden Opportunity for Stroke Prevention!.")
6
Speech, motor, >10 min, age >60, diabetes Outcomes after TIA Gladstone D et al. CMAJ. 2004 Mar 30;170(7):1099-104. 18% 3 month readmission rate after TIA
: % 3 month readmission rate after TIA.")
7
Are all TIA patients at risk of early stroke? Is it cost effective to admit all TIA patients to hospital?

8
Is it cost effective to admit all TIA patients to hospital? NO What is the cost of admitting Patients with Transient Ischemic Attack to hospital? Gordon Gubitz, Stephen Phillips, Victoria Dweyer The average cost of in-patient management of TIA was 328,000 Canadian dollars, of which 95% were accounted for by the cost of the hospital alone. The average cost of in-patient management of TIA was 328,000 Canadian dollars, of which 95% were accounted for by the cost of the hospital alone. If hospitalization of patients with TIA could be reduced, significant cost-savings could be realized. If hospitalization of patients with TIA could be reduced, significant cost-savings could be realized. Cerebrovascular Diseases 1999; 9: 210-214

9
We need a strategy to identify those TIA patients at Highest Risk

10
High Risk TIA: Clinical Predictors California Score: Predict 90 day stroke risk Identified 5 factors associated with high stroke risk Age > 60 Diabetes Duration > 10 min Weakness Speech impairment Risk: 0% if none of the above factors 34% if had all 5 factors Johnston et al. JAMA; 2000; 284: 2901-2906

11
Clinical Predictors of High Risk TIAs Johnston CS et al. JAMA 2000; 284: 2901-6 OR CI p value Age >60 1.8 1.3-4.2 0.005 DM 2.0 1.4-2.9 0.001 >10 min 2.3 1.3-4.2 0.005 Weakness 1.9 1.4-2.6 0.001 Speech 1.5 1.1-2.1 0.01

12
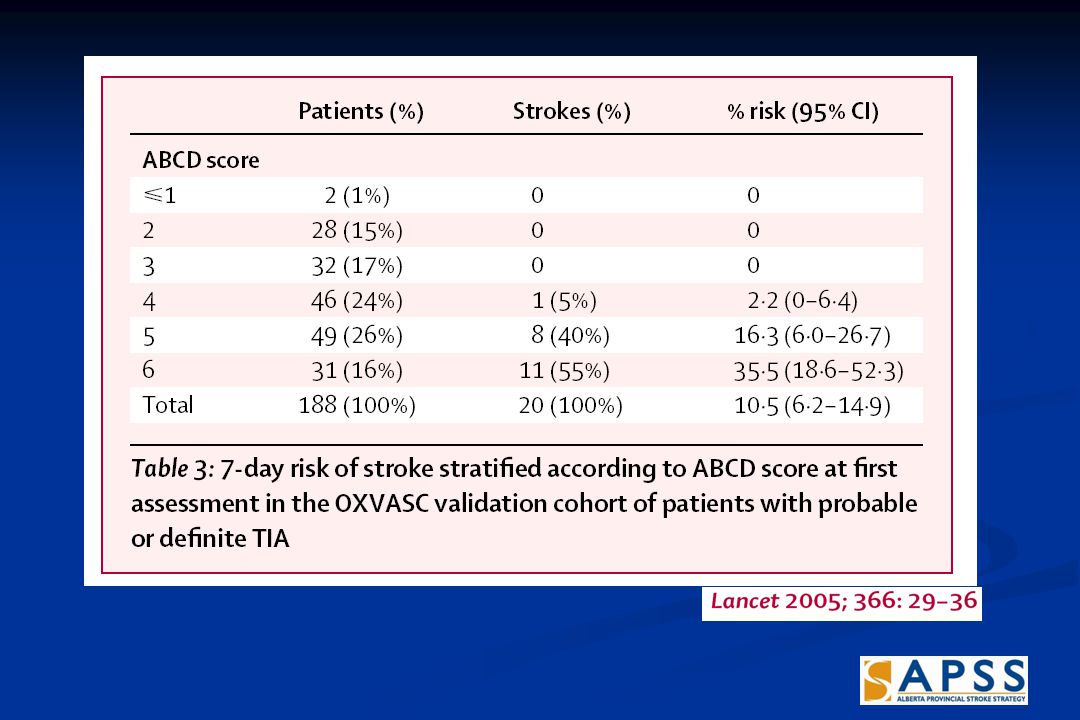
High Risk TIA: Clinical Predictors ABCD Score: Predict 7 day stroke risk; Identified 4 areas associated with high risk Points Age ≥ 60 1 Blood pressure ≥ 140/90 1 Clinical features Unilateral weakness 2 Speech disturbance without weakness 1 Duration of symptoms > 10 min < 59 min 1 ≥ 60 min 2 Risk: Score < 5 = 0.4% risk; Score of 5 = 16% risk; Score of 6 = 35% risk Rothwell et al. Lancet; 2005; 366: 29-36

14
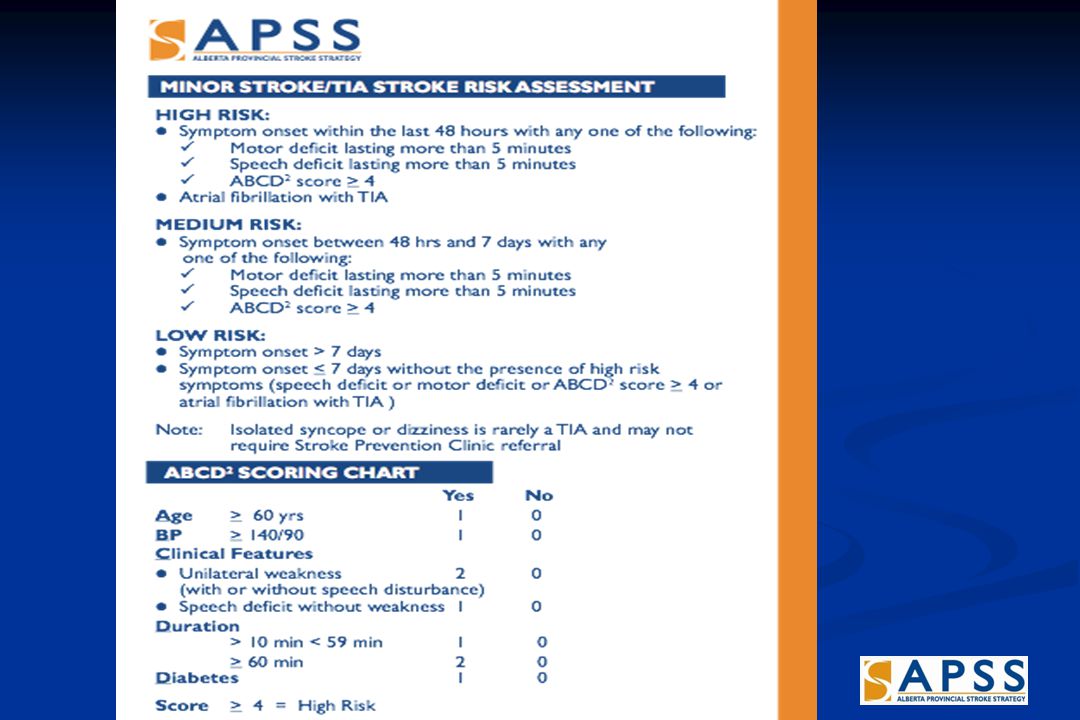
ABCD 2 Score Rothwell et al. Lancet; 2007; 369: 283-292 Yes No Age 60 yrs 1 0 Bp 140/90 1 0 Clinical Features Unilateral weakness 2 0 (with or without speech disturbance) Speech deficit without weakness 1 0 Duration > 10 min < 59 min 1 0 60 min 2 0 Diabetes 1 0 Score 4 = High Risk
 Speech deficit without weakness 1 0 Duration > 10 min < 59 min 1 0 60 min 2 0 Diabetes 1 0 Score 4 = High Risk.")
15
Predictive Value of the ABCD2 progostic score

16
Who is at risk? Scenario 1: Seventy year old right-handed man with a history of diabetes and smoking is seen in the Emergency department after an episode three hours previously of transient aphasia and right hemiparesis lasting 65 minutes. This is his second episode in a week. He denies other neurologic symptoms. His examination is now completely normal, aside from a blood pressure of 160/80.

17
Who is at risk? Age 70 (1) BP 160/80 (1) Weakness (2) 65 minutes (2) Diabetes (1) ABCD 2 score = 7 Risk = 6% (2 day) 11% (7 day) 17% (30 day) 22% (90 day)
 BP 160/80 (1) Weakness (2) 65 minutes (2) Diabetes (1) ABCD 2 score = 7 Risk = 6% (2 day) 11% (7 day) 17% (30 day) 22% (90 day).")
18
High Risk TIA: Neurovascular Imaging CT scan MRI

19
Neurovascular Imaging: CT Scan TIA population: 67% CT performed 4% (13/322) : had evidence of infarct on CT. Risk of stroke higher among those with a new infarct on head CT Stroke. 2003 Dec;34(12):2894-8. Stroke. 2003 Dec;34(12):2894-8.
: Stroke Dec;34(12):")
20
Kaplan-Meier life-table analysis of survival free from stroke for patients with (dotted line) and without (solid line) new infarct on head CT 10% 38% stroke 2003 Dec;34(12):2894-8
 and without (solid line) new infarct on head CT 10% 38% stroke 2003 Dec;34(12):2894-8")
21
Neurovascular Imaging: MRI Neurovascular Imaging: MRI Kidwell C et al. Stroke 1999; 6:1174-1180. Couttts SB et al. Annals of Neurology 2005;57:848-854 Krol A et al. Stroke 2005 40-60% of TIA pts have evidence of ischemic injury on DWI Factors predicting positive DWI: Symptoms lasting > 1 hour Symptoms lasting > 1 hour Motor deficits Motor deficits Aphasia Aphasia If TIA and DWI lesion - higher risk of subsequent stroke Even brief symptoms cause areas of permanent injury

22
22 Alberta Stroke Prevention in TIA’s and Mild StRokE (ASPIRE) TIA Triaging Consensus Urgent triage and assessment of TIA province- wide deserves evaluation within Alberta Urgent triage and assessment of TIA province- wide deserves evaluation within Alberta TIA Triaging algorithm created at Aug 2008 meeting TIA Triaging algorithm created at Aug 2008 meeting Facilitate urgent access using a TIA Hotline Facilitate urgent access using a TIA Hotline Backing of the APSS and the Educational Strategy of the APSS Backing of the APSS and the Educational Strategy of the APSS Pocket cards have been produced Pocket cards have been produced
 TIA Triaging Consensus Urgent triage and assessment of TIA province- wide deserves evaluation within Alberta Urgent triage and assessment of TIA province- wide deserves evaluation within Alberta TIA Triaging algorithm created at Aug 2008 meeting TIA Triaging algorithm created at Aug 2008 meeting Facilitate urgent access using a TIA Hotline Facilitate urgent access using a TIA Hotline Backing of the APSS and the Educational Strategy of the APSS Backing of the APSS and the Educational Strategy of the APSS Pocket cards have been produced Pocket cards have been produced")
24
Once High Risk TIA Identified… then what? TIA MANAGEMENT

26
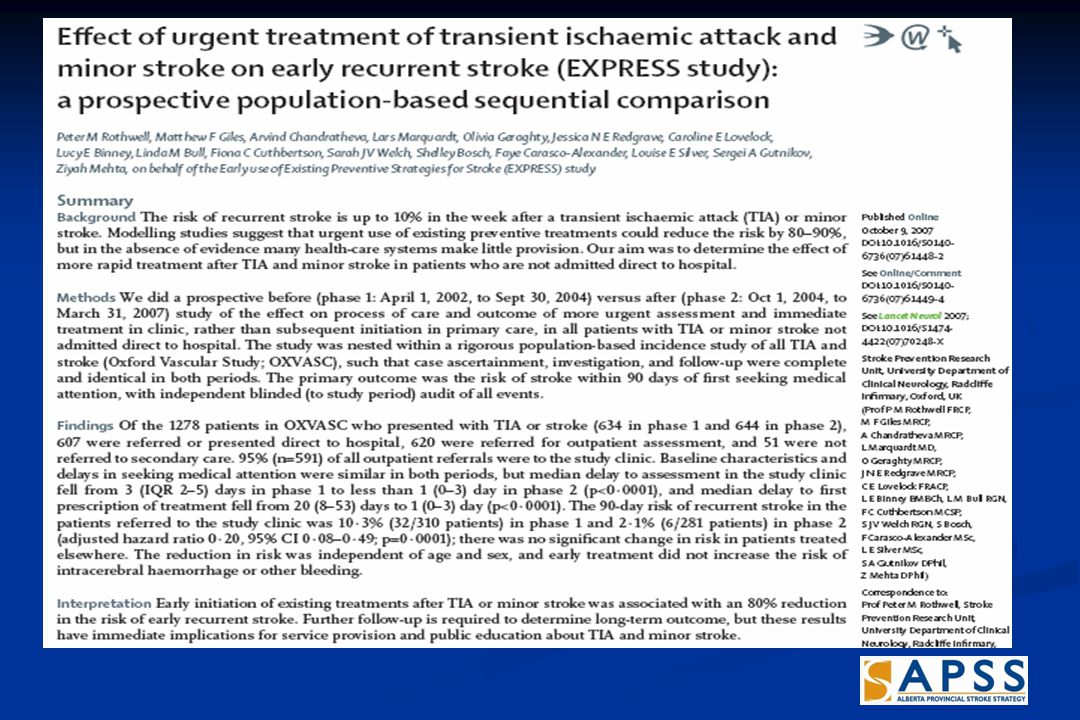
Express Study

28
SOS - TIA

29
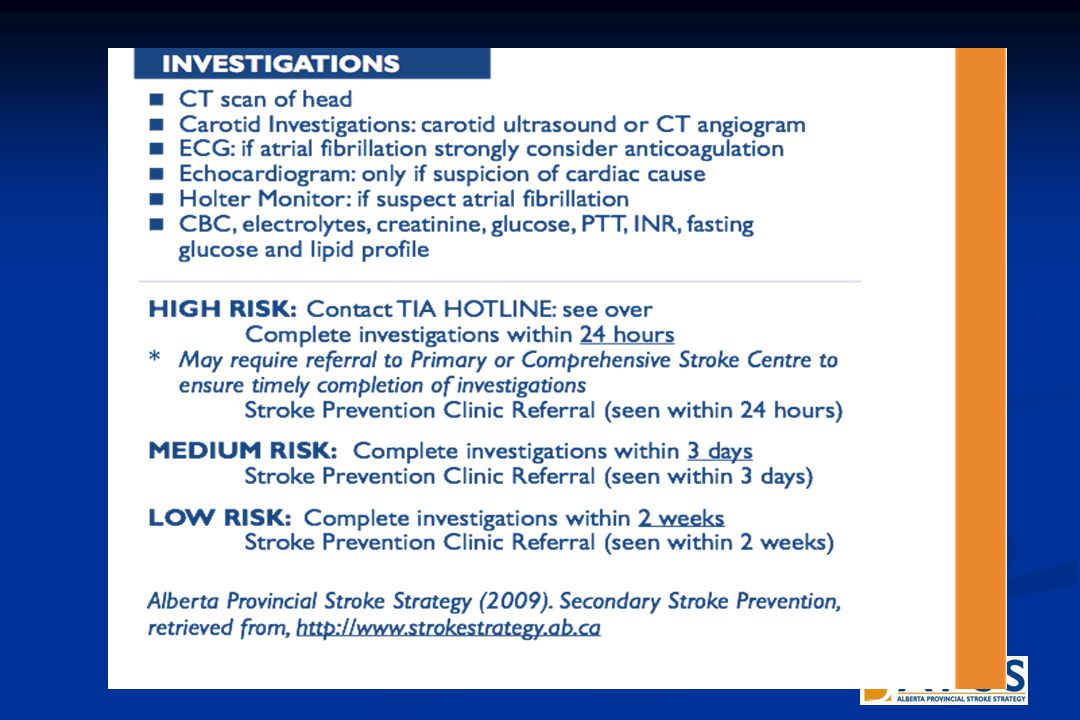
Evaluate the Event: Investigations CT or MRI CT or MRI Rule out mimics, identify stroke type Rule out mimics, identify stroke type Carotid Imaging (carotid duplex, CTA or MRA) Carotid Imaging (carotid duplex, CTA or MRA) Identify stenosis Identify stenosis ECG ECG ? Cardiac cause - afib ? Cardiac cause - afib Holter monitor Holter monitor Echocardiogram Echocardiogram If suspect cardiac cause If suspect cardiac cause Labs - CBC, lytes, Cr, gluc, PTT, INR, fasting lipids Labs - CBC, lytes, Cr, gluc, PTT, INR, fasting lipids

31
TIA Management There are 2 proven therapies to prevent the occurrence of stroke following TIA Antiplatelet / Anticoagulation therapy Antiplatelet / Anticoagulation therapy Carotid Endarterectomy Carotid Endarterectomy

32
Antiplatelet/Anticoagulation Therapy Aspirin (50-325 mg/day) is first line treatment If aspirin naïve- load with 160mg then 81 mg OD If aspirin naïve- load with 160mg then 81 mg OD Options: Aspirin/extended release dypridamal (Aggrenox) 25mg/200mg OD 25mg/200mg OD Clopidogrel (Plavix) 75 mg OD, consider loading with 300 mg 75 mg OD, consider loading with 300 mg Aspirin + Clopidogrel ?????? ASA 81mg OD + Clopidogrel 75mg OD ASA 81mg OD + Clopidogrel 75mg OD Consider loading dose of each agent Consider loading dose of each agent No evidence to suggest any are superior or inferior to aspirin

33
Antiplatelet/Anticoagulation Therapy If cardioembolic source: Long-term anticoagulation - Warfarin Long-term anticoagulation - Warfarin INR acceptable range 2.0 – 3.0 (target 2.5) INR acceptable range 2.0 – 3.0 (target 2.5)
 INR acceptable range 2.0 – 3.0 (target 2.5)")
34
Antiplatelet/Anticoagulation Therapy If cardioembolic source: Long-term anticoagulation – Dabigatran Long-term anticoagulation – Dabigatran Dabigatran does not require dose adjustments or anticoagulation monitoring. Dabigatran does not require dose adjustments or anticoagulation monitoring.

35
Dabigatran etexilate is a novel, small molecule, reversible, direct thrombin inhibitor For oral administration Dabigatran etexilate Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation Antiplatelet/Anticoagulation Therapy Stangier J et al British Journal of Clinical Pharmacology 2007, DOI:10.1111/j.1365- 2125.2007.02899. Sorbera LA et al Dabigatran/Dabigatran Etexilate Drugs of the Future 2005; 30 (9): 877-885. Belch S et al. DMB 2007; doi:10.1124/dmb.107.019083
: Belch S et al. DMB 2007; doi: /dmb")
36
RE-LY ® – study design Atrial fibrillation with ≥ 1 risk factor Absence of contraindications R Warfarin 1 mg, 3 mg, 5 mg (INR 2.0-3.0) N=6000 Dabigatran etexilate 110 mg bid N=6000 Dabigatran etexilate 150 mg bid N=6000 Primary objective: To establish the non-inferiority of dabigatran etexilate to warfarin Minimum 1 year follow-up, maximum of 3 years and mean of 2 years of follow-up Ezekowitz MD, et al. Am Heart J 2009;157:805-10. Connolly SJ., et al. NEJM published online on Aug 30th 2009. DOI 10.1056/NEJMoa0905561 Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation RE-LY ® : Randomised Evaluation of Long term anticoagulant therapy

37
Conclusions Dabigatran etexilate has shown to concurrently reduce both thrombotic and hemorrhagic events Both doses of dabigatran provide different and complimentary advantages over warfarin 150 mg BID has superior efficacy with similar bleeding 110 mg BID has significantly less bleedings with similar efficacy Similar net clinical benefit was seen between the two dabigatran doses Connolly SJ., et al. NEJM published online on Aug 30th 2009. DOI 10.1056/NEJMoa0905561 Dabigatran etexilate is in clinical development and not licensed for clinical use in stroke prevention for patients with atrial fibrillation

38
TIA Management Carotid Endarterectomy

39
Neurovascular Imaging: Carotid Imaging Imaging carotids is an important part of TIA evaluation Carotid doppler ultrasound Carotid doppler ultrasound CT angiography (CTA) CT angiography (CTA) Magnetic resonance angiography Magnetic resonance angiography There is an increased stroke risk with carotid artery disease
 CT angiography (CTA) Magnetic resonance angiography Magnetic resonance angiography There is an increased stroke risk with carotid artery disease")
40
Carotid Endarterectomy If TIA due to ≥ 50% stenosis in extracranial internal carotid artery consider CEA Greatest benefit if surgery within 2 weeks Rothwell et al. Lancet; 2004; 363: 915-25

41
Early Carotid Surgery Better in 50-69% stenosis Rothwell PM et al. Stroke 2004;35:2855-2861. NNT 7

42
Early Carotid Surgery Much Better >70% w/o near-occlusion Rothwell PM et al. Stroke 2004;35:2855-2861. NNT 3

43
Putting it all together High Risk TIA: Identification and Management

44
To order pocket card: there is a link on APSS webpage underneath Professional Education Resources: http://www.strokestrategy.ab.ca/health-care-providers-ed.html http://www.strokestrategy.ab.ca/health-care-providers-ed.html :

45
Case Scenarios #1 70 year old male Episode of right sided weakness and impaired speech lasting about 60 minutes yesterday Risk factors: hypertension, high cholesterol, ex- smoker Exam normal

46
Case Scenarios Time since onset? ABCD2 score? What is the risk? What are you going to do?

47
High Risk Antiplatelet?Investigations?Referrals?

48
Case Scenarios 70 year old male Episode of right sided weakness and impaired speech yesterday Risk factor s: Hypertension, high cholesterol, ex-smoker Exam normal Carotid dopplers: 88% L ICA stenosis

49
Case Scenarios #2 55 year old healthy right-handed female is seen in the clinic after an episode of speech difficulty three days ago lasting approximately 15 minutes. 15 minutes. She denies other neurological symptoms. Her examination is now completely normal aside for a blood pressure of 155/90.

50
Case Scenarios Time since onset? ABCD2 score? What is the risk? What are you going to do?

51
Medium Risk Antiplatelet?Investigations? Stroke Prevention Clinic referral?

52
Questions?

Similar presentations




 Section # 3 Hyperacute Stroke Management Canadian Best Practice Recommendations for.>")














