Download presentation
Presentation is loading. Please wait.

1
A review on bariatric surgery
Good morning, colleagues. Today my presentation will be a review on bariatric surgery. A review on bariatric surgery Dr Dennis CT Lam TKOH

2
Outline Introduction of morbid obesity Bariatric surgery
Comparisons of different surgical procedures Conclusions My presentation will start from the concept of obesity and then I will briefling introduce on different modalities of bariatric surgery. I will include a review on discussing on different aspect on bariatric surgery

3
Obesity Abnormal or excessive fat accumulation that impair health
Defined by body mass index (BMI) in kg/m2 International Asia-Pacific Normal Overweight Class I obesity Class II obesity ≥30 Class III obesity ≥40 Obesity is defined as an abnormal or excessive body fat accumulation, that may impair health or create adverse problem. As we all aware, the degree and classification of obesity is based on the body mass index, which is the BW in kg divided by height in meters square. BMI (body mass index) is a screening tool used to measure weight relative to height. While BMI does not measure body fat directly, it has been shown to correlate to measures of body fat, and is considered an accurate alternative for body fat measurement. With a simple formula, you can calculate your own BMI World Health Organization Asian-Pacific Bariatric Surgery Society 2010
 in kg/m2. International. Asia-Pacific. Normal Overweight Class I obesity Class II obesity ≥30. Class III obesity. ≥40. Obesity is defined as an abnormal or excessive body fat accumulation, that may impair health or create adverse problem. As we all aware, the degree and classification of obesity is based on the body mass index, which is the BW in kg divided by height in meters square. BMI (body mass index) is a screening tool used to measure weight relative to height. While BMI does not measure body fat directly, it has been shown to correlate to measures of body fat, and is considered an accurate alternative for body fat measurement. With a simple formula, you can calculate your own BMI. World Health Organization. Asian-Pacific Bariatric Surgery Society")
4
Morbid obesity International Asia-Pacific BMI ≥ 40 BMI ≥ 37
BMI ≥ 35 with severe obesity-related morbidities BMI ≥ 32 plus Type 2 Diabetes or two obesity-related co-morbidities When we talk about morbid obesity, WHO has defined morbid obesity into which patient had a BMI >40 or BMI >35 with severe obesity related co morbidities The same reason, a different situation is applied on asian pacific, for our population, morbid obesity is defined as BMI>37 or BMI >32 plus DM/ or two obesity related co morbidities When you are so fat that it causes major problems with your life and health, you are morbidly obese. The best and simplest measure of your weight, which tells if you are morbidly obese, is called Body Mass Index (BMI). Severely obese patients are more likely to suffer from major medical, physical or social problems. Moreover, Asian are more susceptible to adverse effect of obesity and the risk of developing obesity-related disease (diabetes, hypertension, hyperlipidemia) are much higher than Caucasian at the same BMI. For this reason, the definition of morbid obesity is different for Caucasian countries and Asia-pacific population. Traditional weight reduction method, include dieting and exercise, plus augmented by drug therapy and behavioral modification, often provide a transient weight loss, but the amount of weight loss is usually insufficient and unsustainable in morbidly obese patients. World Health Organization
. Severely obese patients are more likely to suffer from major medical, physical or social problems. Moreover, Asian are more susceptible to adverse effect of obesity and the risk of developing obesity-related disease (diabetes, hypertension, hyperlipidemia) are much higher than Caucasian at the same BMI. For this reason, the definition of morbid obesity is different for Caucasian countries and Asia-pacific population. Traditional weight reduction method, include dieting and exercise, plus augmented by drug therapy and behavioral modification, often provide a transient weight loss, but the amount of weight loss is usually insufficient and unsustainable in morbidly obese patients. World Health Organization.")
5
Health problems Obviously obesity can create a lot of health problem
Problem of being obese is not just a matter of external appearance. Obesity is a direct cause of a series of health related problem and it should be considered as a chronic disease rather than just a behavioral problem. According to international study, the life expectance of obese patient is just half of those who are not obese. Obesity is an important cause of a number of chronic diseases, such as diabetes, coronary heart disease, high blood pressure and stroke. Obesity increases the risk of developing colon cancer and prostate cancer in man, and breast cancer, cervix cancer and ovary cancer in woman. Other obesity related disease include gallbladder disease, joint disease (related to degeneration and injury due to overweight), gouty arthritis and obstructive sleep apnea (severe obese patient may temporary stop breathing during sleep). Social and psycological problems: Obese people are always being discriminated by the society and being less welcome as compare to slim and attractive ladies. In traditional Chinese population there is mis-conception and believed that obesity is simply as a behavioral problem, which is voluntary, and usually associated with some degree of moral deficiency, from want of self-control to unrestrained gluttony. This attitude posted additional stress to obese individual and may lead to depression, low self-esteem with social avoidance, and severely affect their social and interpersonal relation.
, gouty arthritis and obstructive sleep apnea (severe obese patient may temporary stop breathing during sleep). Social and psycological problems: Obese people are always being discriminated by the society and being less welcome as compare to slim and attractive ladies. In traditional Chinese population there is mis-conception and believed that obesity is simply as a behavioral problem, which is voluntary, and usually associated with some degree of moral deficiency, from want of self-control to unrestrained gluttony. This attitude posted additional stress to obese individual and may lead to depression, low self-esteem with social avoidance, and severely affect their social and interpersonal relation.")
6
Management of obesity Dieting Exercise Weight loss programs Medication
Surgery Conservative options such dieting combined with behavior therapy and exercise should be the first line of therapy. However, for severely obese patients, conservative approach results are disappointing. Among subjects whom successfully loss a substantial quantity of weight, only 5-10% maintain the loss for more than a few years. Pharmacotherapy Drug therapy, such as Orlistat (Xenical) and Sibutramine (Reductil), can also achieve a substantial weight loss of about 10% of the excessive body weight. However, the use of pharmacotherapy for obesity should considered as a short-term option, because patients who respond to drug therapy usually regain weight when therapy is stopped. Nonetheless, medical treatment of obesity may be successful when dealing with moderate obesity, overall results of medical treatment for clinically severe obese patients are poor. Bariatric surgery, also known as weight loss surgery, refers to the various surgical procedures performed to treat obesity by modification of the gastrointestinal tract to reduce nutrient intake and/or absorption. Bariatric surgery is a surgery designed to help patients with serious weight problems to achieve significant weight loss. It is designed for patients who have a history of failed dieting attempts and a BMI exceeding 37 or 32 with diabetes or severe co-morbidities according to Asia-pacific guideline. Patients who have bariatric surgery are usually between 18 and 60 years of age. Bariatric surgery is an option to alleviate debilitating diseases caused by morbid obesity. Patients who intend to undergo this surgery must be highly motivated and understand the risk and long-term change of life style associate with the procedure. They must be able to adhere to diet, exercise, and medical guidelines for the rest of their lives after surgery.
 and Sibutramine (Reductil), can also achieve a substantial weight loss of about 10% of the excessive body weight. However, the use of pharmacotherapy for obesity should considered as a short-term option, because patients who respond to drug therapy usually regain weight when therapy is stopped. Nonetheless, medical treatment of obesity may be successful when dealing with moderate obesity, overall results of medical treatment for clinically severe obese patients are poor. Bariatric surgery, also known as weight loss surgery, refers to the various surgical procedures performed to treat obesity by modification of the gastrointestinal tract to reduce nutrient intake and/or absorption. Bariatric surgery is a surgery designed to help patients with serious weight problems to achieve significant weight loss. It is designed for patients who have a history of failed dieting attempts and a BMI exceeding 37 or 32 with diabetes or severe co-morbidities according to Asia-pacific guideline. Patients who have bariatric surgery are usually between 18 and 60 years of age. Bariatric surgery is an option to alleviate debilitating diseases caused by morbid obesity. Patients who intend to undergo this surgery must be highly motivated and understand the risk and long-term change of life style associate with the procedure. They must be able to adhere to diet, exercise, and medical guidelines for the rest of their lives after surgery.")
7
Surgery versus non-surgical interventions

8
Surgery versus non-surgical interventions
Surgery results in greater weight loss than conventional treatment in severe obesity Reductions in co-morbidities also occured Improvements in health-related quality of life occurred Surgery is associated with complications and mortalities Dixon 2008, Mingrone 2002, O’Brien 2006

9
Indication of bariatric surgery
International Asia-pacific BMI >40 BMI >35 BMI >35 with co-morbidities BMI > 32 with co-morbidities Failed less invasive methods and at high risk for obesity-associated morbidity and mortality BMI > 30 and central obesity with at least two criteria for metabolic syndrome Co-morbidities: HT, IGT, DM, hyperlipidemia, OSA Metabolic syndrome: HT, DM, raised TG, reduced HDL cholesterol U.S. National Institutes of Health Asia-Pacific of Metabolic and Bariatric Surgery Society (APMBSS)
")
10
Classification of bariatric surgery
Restrictive Mal-absorptive Mixed Weight reduction surgery is the most effective method to achieve sustainable weight loss among patients with morbid obesity. These procedures are not for cosmesis but for prevention of the pathologic consequences of morbid obesity. After successful weight reduction, some of obesity-related medical conditions (e.g. hypertension, diabetes, obstructive sleep apnea) will expect to be improved. However, weight-reduction surgery carries potential operative risk and it should be consider as the last resort after failure of previous non-surgical weight reduction treatment. How it works? 1.Restrictive Procedures Restrictive procedures involve creating a small stomach pouch, which limits the amount of food patients can eat. The smaller stomach pouch fills quickly, which helps patients feel satisfied with less food. Examples of restrictive procedures include adjustable gastric banding and sleeve gastrectomy. 2.Maladsorptive Procedure For malabsortive procedures, the surgeon re-arranges the small intestine so that food skips a portion of it. The small intestine absorbs calories and nutrients from food, and avoiding part of it means that some calories and nutrients are not absorbed. However, malabsorptive procedures is associated with more nutritional problems afterwards and most surgeons will perform combined restriction with limited mal-absorption procedure to reduce these nutritional problem. Example of mal-absorptive procedure include Biliopancreatic Diversion (BPD) and BPD with Duodenal Switch operation. 3.Combined Procedures Certain procedures such as gastric bypass surgery use a combination of restriction and malabsorption. During this procedure, the surgeon creates a small stomach pouch first. The surgeon then attaches the small intestine directly to the stomach pouch. This allows food to bypass a large portion of the small intestine, which absorbs calories and nutrients. The smaller stomach pouch causes patients to feel fuller sooner and eat less food; bypassing a portion of the small intestine means the patient’s body absorbs fewer calories. Example of restrictive procedures include Roux-en Y gastric bypass and Mini-gastric bypass.
 will expect to be improved. However, weight-reduction surgery carries potential operative risk and it should be consider as the last resort after failure of previous non-surgical weight reduction treatment. How it works 1.Restrictive Procedures Restrictive procedures involve creating a small stomach pouch, which limits the amount of food patients can eat. The smaller stomach pouch fills quickly, which helps patients feel satisfied with less food. Examples of restrictive procedures include adjustable gastric banding and sleeve gastrectomy. 2.Maladsorptive Procedure For malabsortive procedures, the surgeon re-arranges the small intestine so that food skips a portion of it. The small intestine absorbs calories and nutrients from food, and avoiding part of it means that some calories and nutrients are not absorbed. However, malabsorptive procedures is associated with more nutritional problems afterwards and most surgeons will perform combined restriction with limited mal-absorption procedure to reduce these nutritional problem. Example of mal-absorptive procedure include Biliopancreatic Diversion (BPD) and BPD with Duodenal Switch operation. 3.Combined Procedures Certain procedures such as gastric bypass surgery use a combination of restriction and malabsorption. During this procedure, the surgeon creates a small stomach pouch first. The surgeon then attaches the small intestine directly to the stomach pouch. This allows food to bypass a large portion of the small intestine, which absorbs calories and nutrients. The smaller stomach pouch causes patients to feel fuller sooner and eat less food; bypassing a portion of the small intestine means the patient’s body absorbs fewer calories. Example of restrictive procedures include Roux-en Y gastric bypass and Mini-gastric bypass.")
11
Restrictive Procedures Mal-absorptive Procedures
Creation of a small gastric pouch To produce early satiety To reduce oral intake Re-construct the small intestine so that the food bypass it To prevent nutrient from being absorbed effectively before mixing with digestive juice 1.Restrictive Procedures Restrictive procedures involve creating a small stomach pouch, which limits the amount of food patients can eat. The smaller stomach pouch fills quickly, which helps patients feel satisfied with less food. Examples of restrictive procedures include adjustable gastric banding and sleeve gastrectomy. 2.Maladsorptive Procedure For malabsortive procedures, the surgeon re-arranges the small intestine so that food skips a portion of it. The small intestine absorbs calories and nutrients from food, and avoiding part of it means that some calories and nutrients are not absorbed. However, malabsorptive procedures is associated with more nutritional problems afterwards and most surgeons will perform combined restriction with limited mal-absorption procedure to reduce these nutritional problem. Example of mal-absorptive procedure include Biliopancreatic Diversion (BPD) and BPD with Duodenal Switch operation. 3.Combined Procedures Certain procedures such as gastric bypass surgery use a combination of restriction and malabsorption. During this procedure, the surgeon creates a small stomach pouch first. The surgeon then attaches the small intestine directly to the stomach pouch. This allows food to bypass a large portion of the small intestine, which absorbs calories and nutrients. The smaller stomach pouch causes patients to feel fuller sooner and eat less food; bypassing a portion of the small intestine means the patient’s body absorbs fewer calories. Example of restrictive procedures include Roux-en Y gastric bypass and Mini-gastric bypass.
 and BPD with Duodenal Switch operation. 3.Combined Procedures Certain procedures such as gastric bypass surgery use a combination of restriction and malabsorption. During this procedure, the surgeon creates a small stomach pouch first. The surgeon then attaches the small intestine directly to the stomach pouch. This allows food to bypass a large portion of the small intestine, which absorbs calories and nutrients. The smaller stomach pouch causes patients to feel fuller sooner and eat less food; bypassing a portion of the small intestine means the patient’s body absorbs fewer calories. Example of restrictive procedures include Roux-en Y gastric bypass and Mini-gastric bypass.")
12
Restrictive procedure
Intra-gastric balloon Vertical band gastroplasty Adjustable gastric banding Sleeve gastrectomy Mal-absorptive procedure Bilio-pancreatic diversion Duodenal switch Mixed procedure Roux-en-Y gastric bypass

13
Restrictive procedure
Intra-gastric balloon Vertical band gastroplasty Adjustable gastric banding Sleeve gastrectomy Mal-absorptive procedure Bilio-pancreatic diversion Duodenal switch Mixed procedure Roux-en-Y gastric bypass

14
Restrictive procedures
Intra-gastric balloon Adjustable gastric banding Sleeve gastrectomy

15
Intra-gastric balloon
What is Intra-gastric Balloon The use of an intragastric balloon in the treatment of obesity and morbid obesity has been a well-known practice. The idea of using a gastric space-occupying volume device, giving a sensation of satiety, for the control of obesity was first described in However, in the mid 1980's, poorly designed balloons had numerous complications leading to spontaneous and early deflations, balloon displacement, and intestinal obstruction. Not until 1990's, a new type of intragastric balloon with improved design which offers numerous advantages and has become a clinically accepted method of treatment of obesity in Europe and south America. IGB treatment program aims at behavioral modification of poor eating habit through sense of satiety created by IGB, together with dietetic supervision of low calorie meal during the 6 months treatment period. The use of the intragastric balloon in the treatment and management of morbid obesity is not a panacea; correct patient selection and respect of the dietetic and behavioral program are key factors in obtaining successful results. Experience in Hong Kong reviewed in average kg of weight can be lost by IGB program. Nevertheless, after the removal of the balloon, weight-regain is possible. It is thus not a long-term solution of obesity and can never replace surgery in morbidly obese individuals. However, in selective group of patient who is not suitable for surgery, IGB program is a valid alternative in controlling the body weight. How Is the Intragastric Balloon Placed in the Stomach? The balloon is introduced into the stomach through the mouth without the need for surgery. The physician conducts an initial examination of the stomach using an endoscopic camera. If no abnormalities are observed, the physician proceeds with placement of the balloon through the mouth and down the oesophagus into the stomach. The balloon is made of a soft and pliable silicone material and is inserted while in its smallest, deflated form. The swallowing process is made easier with the help of anaesthetics applied topically to numb the throat area. When the balloon is well within the stomach, it is filled with approximately 500cc of saline fluid. The procedure lasts approximately twenty minutes and is performed on an out-patient basis. Who Can Join the IGB program? In 2004, we established a new IGB program for those patents who is not suitable or do not consent for operative bariatric surgery. In this program, IGB therapy is used as a temporary weight control measure in three groups of patients: 1.Patients who are surgical candidates and willing to receive bariatric surgery, but preoperative weight reduction is considered beneficial, especially in super-obese (e.g. BMI>60) individual. 2.Patients who are candidates for bariatric surgery but unwilling to undergo major surgical procedure. 3.Patients with BMI who are not candidate for surgery but suffered from obese-related co-morbidities and had failed conservative weight reduction therapy in the past. How Long Is the IGB Used? The balloon currently can be used for six months. Longer periods of use are not recommended. Over time the acidic content of the stomach will weaken the balloon material and cause the balloon to deflate. After 6 months, the balloon is removed in the same way it was placed, via the oesophagus and mouth. What Unpleasant Effects Are Possible with the IGB program? 1.Severe nausea & vomiting - may occur immediate after placement of IGB. Some patients may require anti-emetic treatment during the first few days but it usually disappear within 1 week after placement. 2.Dehydration - may result from stomach upset and reduce fluid intake. Some patients may require hospitalization for fluid replacement. 3.Balloon deflation - spontaneous balloon deflation is uncommon (<5%) if it is remove within 6 months time. However, un-noticed deflation may lead to bowel obstruction and some patient may require operative treatment to removed the balloon and relief obstruction. Will I Regain My Weight after the Intragastric Balloon Is Removed? Because the balloon in the stomach creates a feeling of fullness, it acts as an aid to weight reduction and may help you to adhere to a prescribed diet. You will have a much greater chance of maintaining your weight loss after balloon removal if you maintain and improve the diet and behavior changes you made while using the balloon. In our experience, 30% of patients can maintain more than 10% of their lost weight in average of 12 months after balloon removal. Intra-gastric balloon Endoscopic method Placing a balloon into the stomach to decrease the gastric space Create a sense of fullness Can be left for a maximum of 6 months May be used prior to another bariatric surgery
 individual. 2.Patients who are candidates for bariatric surgery but unwilling to undergo major surgical procedure. 3.Patients with BMI who are not candidate for surgery but suffered from obese-related co-morbidities and had failed conservative weight reduction therapy in the past. How Long Is the IGB Used The balloon currently can be used for six months. Longer periods of use are not recommended. Over time the acidic content of the stomach will weaken the balloon material and cause the balloon to deflate. After 6 months, the balloon is removed in the same way it was placed, via the oesophagus and mouth. What Unpleasant Effects Are Possible with the IGB program 1.Severe nausea & vomiting - may occur immediate after placement of IGB. Some patients may require anti-emetic treatment during the first few days but it usually disappear within 1 week after placement. 2.Dehydration - may result from stomach upset and reduce fluid intake. Some patients may require hospitalization for fluid replacement. 3.Balloon deflation - spontaneous balloon deflation is uncommon (<5%) if it is remove within 6 months time. However, un-noticed deflation may lead to bowel obstruction and some patient may require operative treatment to removed the balloon and relief obstruction. Will I Regain My Weight after the Intragastric Balloon Is Removed Because the balloon in the stomach creates a feeling of fullness, it acts as an aid to weight reduction and may help you to adhere to a prescribed diet. You will have a much greater chance of maintaining your weight loss after balloon removal if you maintain and improve the diet and behavior changes you made while using the balloon. In our experience, 30% of patients can maintain more than 10% of their lost weight in average of 12 months after balloon removal. Intra-gastric balloon. Endoscopic method. Placing a balloon into the stomach to decrease the gastric space. Create a sense of fullness. Can be left for a maximum of 6 months. May be used prior to another bariatric surgery.")
16
Adjustable gastric banding
It is a purely gastric restrictive procedure that involves the use of an adjustable silicone band placed around the upper part of the stomach by laparoscopic approach, which creates a small gastric pouch (15 ml) with a narrow outlet. In addition to the gastric band, an injection port is attached to the abdominal wall, underneath the skin. The port is connected to the band with soft, thin tubing. These bands will be adjusted after operation by injection or withdrawal of saline from the reservoir, which is accessed through puncturing the skin Expected weight loss: Usually loss ~40-50% of the excessive body weight in 2 years. (Excessive Body Weight = current body weight – body weight at BMI 25) Advantages of LAGB: 1.Safest procedure among all bariatric surgery; no cutting on stomach. 2.Degree of restriction is adjustable after initial surgery; no need additional surgery for adjustment if restriction is too tight or too loose. 3.Procedure is completely reversible; gastric band can be removed by another operation without alter the normal structure and function if the gastrointestinal tract. 4.Faster recovery with short hospital stay; usually discharge home 2 days after surgery. Disadvantages: 1.Placement of foreign body inside the body; potential risk of infection, leakage , gastric erosion and displacement, may require removal if problem happens (~10%). 2.Require frequent follow up for adjustment, need good compliance of new eating habit; may develop enlargement of stomach or oesophagus above the band if not complies. 3.Slower rate of weight loss; among of weight loss may be less in super-obese patients or patients with poor compliance. Adjustable gastric banding Placing a constricting ring around the fundus Adjust the size of the pouch through a subcutaneous access port Least invasive, reversible, adjustable Slower weight loss, less effective in super-obese patient Risk of gastric erosion and band displacement
 with a narrow outlet. In addition to the gastric band, an injection port is attached to the abdominal wall, underneath the skin. The port is connected to the band with soft, thin tubing. These bands will be adjusted after operation by injection or withdrawal of saline from the reservoir, which is accessed through puncturing the skin. Expected weight loss: Usually loss ~40-50% of the excessive body weight in 2 years. (Excessive Body Weight = current body weight – body weight at BMI 25) Advantages of LAGB: 1.Safest procedure among all bariatric surgery; no cutting on stomach. 2.Degree of restriction is adjustable after initial surgery; no need additional surgery for adjustment if restriction is too tight or too loose. 3.Procedure is completely reversible; gastric band can be removed by another operation without alter the normal structure and function if the gastrointestinal tract. 4.Faster recovery with short hospital stay; usually discharge home 2 days after surgery. Disadvantages: 1.Placement of foreign body inside the body; potential risk of infection, leakage , gastric erosion and displacement, may require removal if problem happens (~10%). 2.Require frequent follow up for adjustment, need good compliance of new eating habit; may develop enlargement of stomach or oesophagus above the band if not complies. 3.Slower rate of weight loss; among of weight loss may be less in super-obese patients or patients with poor compliance. Adjustable gastric banding. Placing a constricting ring around the fundus. Adjust the size of the pouch through a subcutaneous access port. Least invasive, reversible, adjustable. Slower weight loss, less effective in super-obese patient. Risk of gastric erosion and band displacement.")
17
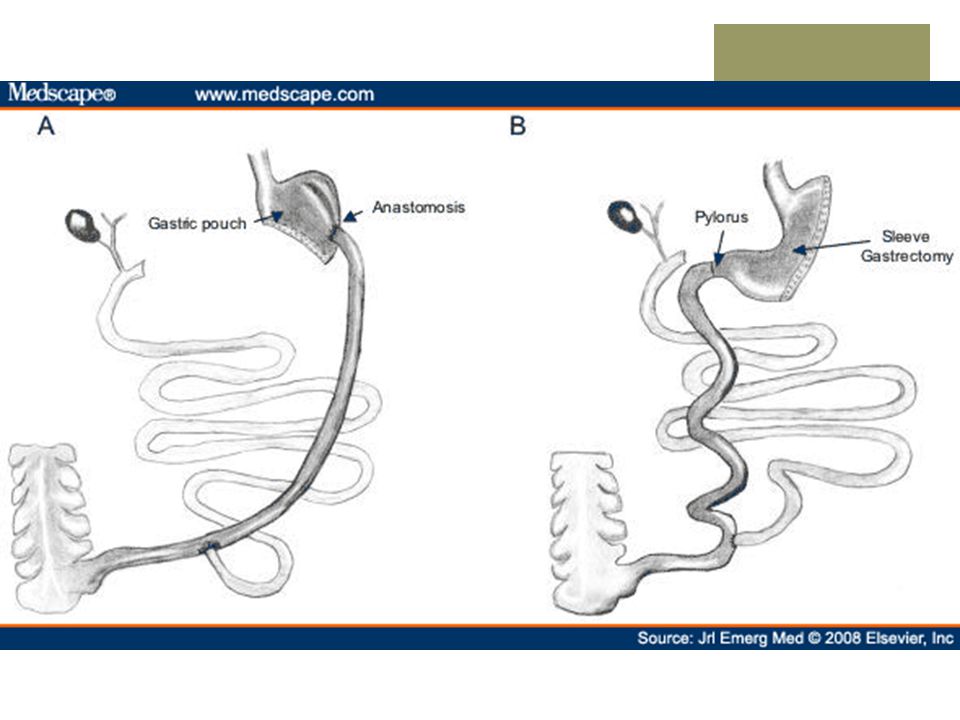
"Sleeve gastrectomy" or "vertical gastrectomy" is a new form of bariatric procedure in weight management. It involves removal of >75% of stomach and leaving a small gastric tube and this procedure resulting decrease in the stomach size inhibits distention of the stomach and increasing the patient’s sensation of fullness and decreasing their appetite. Some posit-increased satiety results from the decrease in production of an appetite hormone - Ghrelin, which secreted by the part of the stomach that was removed during surgery. Expected weight loss: Usually loss ~50 – 70% of the excessive body weight in 2 years. (lack long-term >5 years data) Advantages: 1.It does not require disconnecting or reconnecting the intestines. 2.It is a technically simpler and safer operation than the gastric bypass or the duodenal switch. 3.It does not affect adsorption of vitamin and minerals. 4.There is no foreign body inside your body. 5.It does not need adjustments or fills. Disadvantages: 1.Non-reversible surgery – stomach cannot return to normal. 2.Potential risk of leakage and bleeding from cutting edge of stomach tube (<5%). 3.New procedure – Lack of long-term data. Sleeve gastrectomy Division of the stomach vertically to reduce its size to about 25% Leave pyloric valve intact Risk of staple line leakage and bleeding Single procedure or as first part of a staged procedure Lack of long term data
 Advantages: 1.It does not require disconnecting or reconnecting the intestines. 2.It is a technically simpler and safer operation than the gastric bypass or the duodenal switch. 3.It does not affect adsorption of vitamin and minerals. 4.There is no foreign body inside your body. 5.It does not need adjustments or fills. Disadvantages: 1.Non-reversible surgery – stomach cannot return to normal. 2.Potential risk of leakage and bleeding from cutting edge of stomach tube (<5%). 3.New procedure – Lack of long-term data. Sleeve gastrectomy. Division of the stomach vertically to reduce its size to about 25% Leave pyloric valve intact. Risk of staple line leakage and bleeding. Single procedure or as first part of a staged procedure. Lack of long term data.")
18
Mal-absorptive procedures
Bilio-pancreatic diversion Duodenal switch

19
Bilio-pancreatic diversion
Limited horizontal subtotal gastrectomy to reduce oral intake The gastric pouch is larger Part of the small bowel is bypassed by construction of a long limb Roux-en-Y anastomosis with short common alimentary channel Risk of anastomotic leak and nutritional deficiency

20
Duodenal switch Sleeve gasrectomy rather than horizontal gastrectomy
Can be used as a staged procedure after sleeve gastrectomy

22
Mixed procedures Roux-en-Y gastric bypass

23
Roux-en-Y gastric bypass
Although LAGB and LSG are effective against most of our patient with morbid obesity, it still has its limitations. Restrictive procedure cannot limit fluid calories and patients with poor compliance of dietary advice are at risk of inadequate weight loss or pouch dilatation secondary to binge eating behavior. Gastric bypass, on the other hand, is a hybrid procedure combining gastric partition (restrictive) and foregut bypass (malabsorptive). Firstly, we divide the stomach into a small upper pouch and a much larger, lower "remnant" pouch, and then re-arrange the small intestine to allow food to enter distal small bowel without passage of remnant stomach, duodenum and proximal jejunum. There are two forms of reconstruction techniques. Expected weight loss: Usually loss ~50 – 70% of the excessive body weight in 2 years. Advantages: 1.Faster and more weight loss. 2.More effective control of diabetes after surgery. 3.More reliable weight loss for high BMI patients. Disadvantages: 1.Need division and re-join of bowel, more complex and higher surgical risk of development of complications. 2.A condition known as "dumping syndrome" can occur as the result of rapid emptying of stomach contents into the small intestine which lead to nausea, weakness, sweating, faintness and, on occasion, diarrhea after eating sweets and high fat diet. 3.Because the part of the bowel is bypassed, nutrition problems may happen if they do not follow doctor's treatment. Absorption of iron and Vitamin B12 is affected which may lead to anemia. Reduced the ability to absorb calcium and may also lead to bone disease especially in post-menopausal women. However, most of these problems can be prevent by vitamin and minerals supplements. 4.since most of the stomach is bypassed during surgery, any disease process (ulcer, cancer) will not be able to examine by ordinary investigation tools (contrast X-ray, upper endoscopy). A hybrid procedure combining gastric partition (restrictive) and foregut bypass (mal-absorptive) Creation of a small gastric pouch with a bypass that prevent nutrient from absorption Risk of anastomotic leak, nutritional deficiency, dumping syndrome
 and foregut bypass (malabsorptive). Firstly, we divide the stomach into a small upper pouch and a much larger, lower remnant pouch, and then re-arrange the small intestine to allow food to enter distal small bowel without passage of remnant stomach, duodenum and proximal jejunum. There are two forms of reconstruction techniques. Expected weight loss: Usually loss ~50 – 70% of the excessive body weight in 2 years. Advantages: 1.Faster and more weight loss. 2.More effective control of diabetes after surgery. 3.More reliable weight loss for high BMI patients. Disadvantages: 1.Need division and re-join of bowel, more complex and higher surgical risk of development of complications. 2.A condition known as dumping syndrome can occur as the result of rapid emptying of stomach contents into the small intestine which lead to nausea, weakness, sweating, faintness and, on occasion, diarrhea after eating sweets and high fat diet. 3.Because the part of the bowel is bypassed, nutrition problems may happen if they do not follow doctor s treatment. Absorption of iron and Vitamin B12 is affected which may lead to anemia. Reduced the ability to absorb calcium and may also lead to bone disease especially in post-menopausal women. However, most of these problems can be prevent by vitamin and minerals supplements. 4.since most of the stomach is bypassed during surgery, any disease process (ulcer, cancer) will not be able to examine by ordinary investigation tools (contrast X-ray, upper endoscopy). A hybrid procedure combining gastric partition (restrictive) and foregut bypass (mal-absorptive) Creation of a small gastric pouch with a bypass that prevent nutrient from absorption. Risk of anastomotic leak, nutritional deficiency, dumping syndrome.")
24
Comparisons of different surgical procedures
Weight loss Remission of diabetes Complications

25
Restrictive procedure
Adjustable gastric banding Sleeve gastrectomy Mal-absorptive procedure Bilio-pancreatic diversion Duodenal switch Mixed procedure Roux-en-Y gastric bypass

26
Restrictive procedures
Adjustable gastric banding Sleeve gastrectomy

27
Restrictive procedures
Adjustable Gastric Banding (AGB) Meta-analysis demonstrated a 49.4% excessive weight loss for laparoscopic AGB surgery (p<0.001) AGB leads to a reversal rate of type 2 DM of 62% Lowest complication rate Meijer RI, et al. Bariatric surgery as a novel treatment for type 2 diabetes mellitus: a systematic review. Archives of Surgery 2011 Garb J, et al. Bariatric surgery for the treatment of morbid obesity: a meta-analysis of weight loss outcomes for laparoscopic adjustable gastric banding and laparoscopic gastric bypass. Obesity Surgery 2009
 Meta-analysis demonstrated a 49.4% excessive weight loss for laparoscopic AGB surgery (p<0.001) AGB leads to a reversal rate of type 2 DM of 62% Lowest complication rate. Meijer RI, et al. Bariatric surgery as a novel treatment for type 2 diabetes mellitus: a systematic review. Archives of Surgery Garb J, et al. Bariatric surgery for the treatment of morbid obesity: a meta-analysis of weight loss outcomes for laparoscopic adjustable gastric banding and laparoscopic gastric bypass. Obesity Surgery")
28
Restrictive procedures
Sleeve gastrectomy (SG) Mean excess weight loss was reported to be 55.4% 70% of patients had remission of type 2 diabetes Laparoscopic SG is an effective weight loss procedure that can be performed safely as a primary procedure or staged procedure Brethauer SA, et al. Systematic review of sleeve gastrectomy as staging and primary bariatric procedure. Surg Obes Relat Dis 2009
 Mean excess weight loss was reported to be 55.4% 70% of patients had remission of type 2 diabetes. Laparoscopic SG is an effective weight loss procedure that can be performed safely as a primary procedure or staged procedure. Brethauer SA, et al. Systematic review of sleeve gastrectomy as staging and primary bariatric procedure. Surg Obes Relat Dis")
29
Mal-absorptive procedures
Bilio-pancreatic diversion Duodenal switch

30
Mal-absorptive procedures
Weight loss associated with BPD/DS has been greater than any other bariatric procedure Excess weight loss of 70% to 80% has been achieved long- term Excellent resolution of co-morbidities has been associated with a 98% cure rate for type 2 diabetes BPD/DS are more technically demanding and are frequently performed on super-morbidly obese patients, complication and mortality rates have been higher Fontana MA, et al. The surgical treatment of metabolic disease and morbid obesity. Gastroenterology Clinics of North America, 2010 Marceau P, et al. Biliopancreatic diversion with duodenal switch. World J Surg 1998

31
Mixed procedures Roux-en-Y gastric bypass

32
Mixed procedure Meta-analysis demonstrated 62.6% (p<0.001) excessive weight loss for Laparoscopic gastric bypass surgery Roux-en-Y Gastric bypass leads to a reversal rate of type 2 DM of 83% Meijer RI, et al. Bariatric surgery as a novel treatment for type 2 diabetes mellitus: a systematic review. Archives of Surgery 2011 Garb J, et al. Bariatric surgery for the treatment of morbid obesity: a meta-analysis of weight loss outcomes for laparoscopic adjustable gastric banding and laparoscopic gastric bypass. Obesity Surgery 2009

33
Conclusion

34
Comparisons of different surgical procedures
Excessive weight loss Diabetes remission Mortality Restrictive Adjustable gastric banding 49.4% 62% 0.05% Sleeve gastrectomy 55.4% 70% 0.17% Mal-absorptive Bilio-pancreatic diversion 70-80% 98% 1.9% Mixed Roux-en-Y Gastric bypass 62.6% 83% 0.5%

35
Comparisons of different surgical procedures
Excessive weight loss Diabetes remission Mortality Restrictive Adjustable gastric banding 49.4% 62% 0.05% Sleeve gastrectomy 55.4% 70% 0.17% Mal-absorptive Bilio-pancreatic diversion 70-80% 98% 1.9% Mixed Roux-en-Y Gastric bypass 62.6% 83% 0.5%

36
Comparisons of different surgical procedures
Excessive weight loss Diabetes remission Mortality Restrictive Adjustable gastric banding 49.4% 62% 0.05% Sleeve gastrectomy 55.4% 70% 0.17% Mal-absorptive Bilio-pancreatic diversion 70-80% 98% 1.9% Mixed Roux-en-Y Gastric bypass 62.6% 83% 0.5%

37
Conclusion Weight loss is greatest for purely mal-absortive procedure (BPD/ DS) but with higher complication rates and mortality Sleeve gastrectomy can be performed safely as a primary or staged procedure, but more long term data is required Roux-en-Y gastric bypass is considered as the gold standard and is the commonest performed procedure in USA

38
Take home message Management of patient with morbid obesity required a multi- disciplinary approach Surgery is more effective than conventional management It is important to match the appropriate surgery to the appropriate patient

39
The end

Similar presentations