Download presentation
Presentation is loading. Please wait.

1
Establishing and running a new Quitline in Hungary Peter Vajer Robert Urban Barna Boze Ferenc Tamás János Szabó

2
Content Background Preparation Launch Challenges

3
World Tobacco Atlas

4
Date of the survey Total smoking prevalence Men smoking prevalence Women smoking prevalence 198635,14922,4 19943543,726,6 19994153,130,4 20003338,929 200334,541,528,5 20043139,622,6 2005364330 2006364430 Tombor et al. Epidemiology of smoking in Hungary – a national representative study Orvosi Hetilap 151. évfolyam, 9. szám ■ 330–337

5
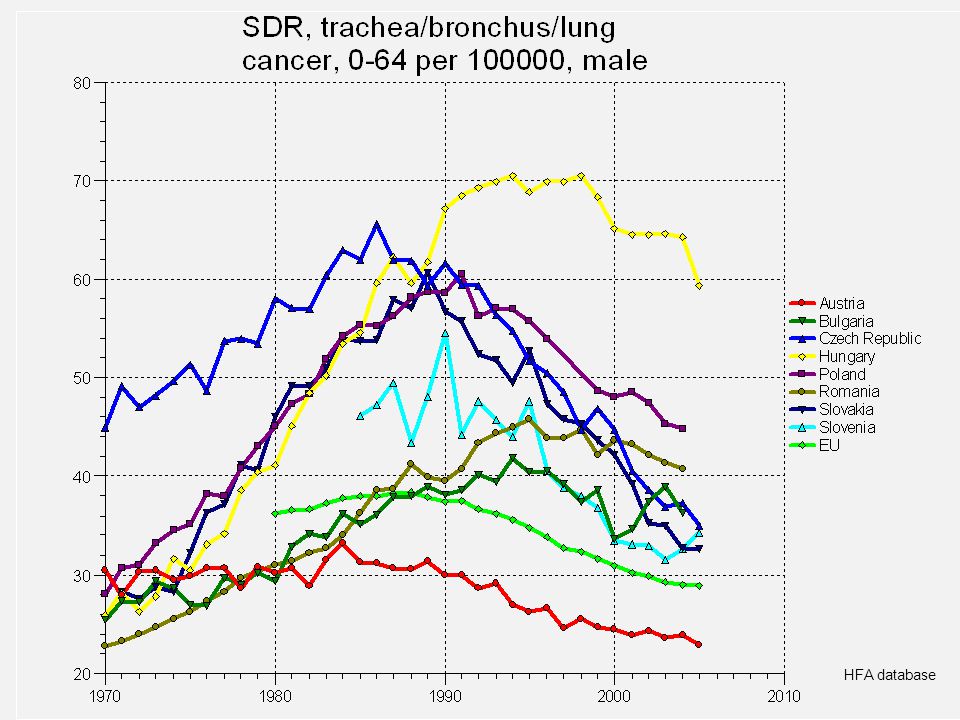
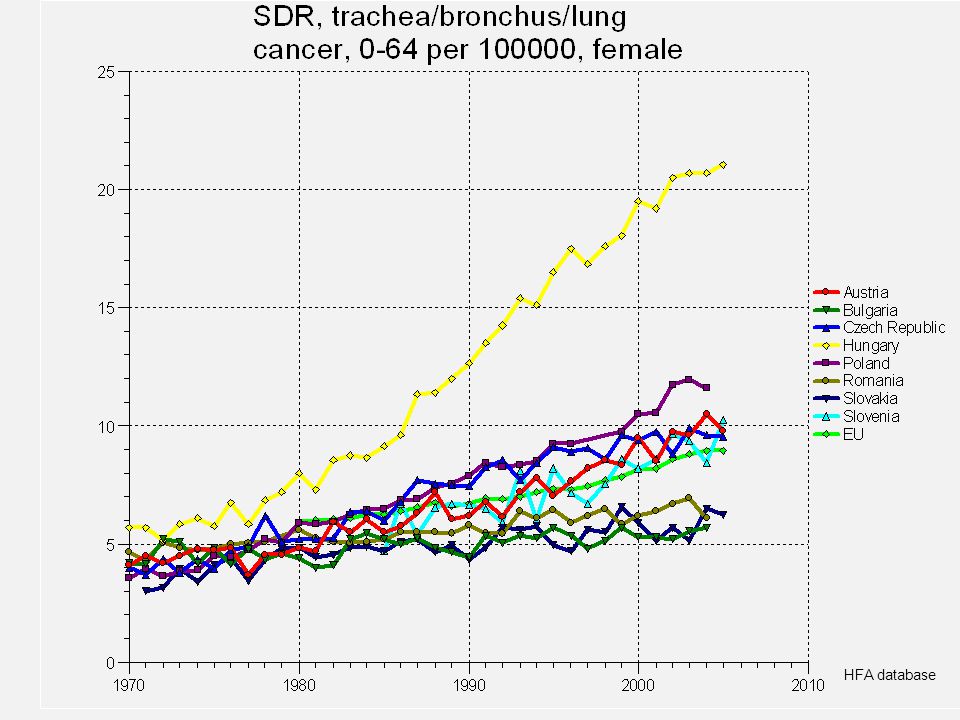
HFA database

8
Tobacco control in Hungary 1990-2010 Taxes are raised regularly and above the rate of inflation (still much cheaper than in Western countries) Ban of direct and indirect marketing (June 2008) 11 th country in the world ratifying FCTC “Decade of Health - National Public Health Program”
 Ban of direct and indirect marketing (June 2008) 11 th country in the world ratifying FCTC Decade of Health - National Public Health Program")
9
ProblemBackground enforcement of tobacco related laws and regulations are still weak No incentives in tobacco-related regulations no regular communication of efforts of the anti-smoking community towards the public, the media and decision makers there are overlapping among programs and activities, resulting in a waste of time and resources no co-ordinated advocacy in the introduction of best practice, legislative, regulatory measures information of decision makers on the roles and impact of tobacco control interventions is inadequate lack of knowledge about the FCTC tobacco industry’s PR and communication is still more effective TI was successful in persuading the government on the call for derogation in the introduction of minimum EU tobacco tax level

10
Problem list Prevalence of smoking is stable in the past 10 years High smoking related mortality and morbidity Lack of good and comprehensive tobacco control programs No reimbursement neither for cessation activity nor for pharmacotherapy

11
Pfizer Global Health Fund + Pfizer Hungary Grant

12
Smoking cessation “services” Network of pulmonologists Family physicians/GPs No quit centers

13
GHP grant - summary Establishing a smoking cessation center in Budapest Training smoking cessation specialists Providing proactive and reactive telephone; group and individual counseling Capacity building (research, services, networking)
")
14
Main goals To implement intense behavioural smoking cessation programs To provide a referral system for health care providers To build up collaboration between the center and primary care providers To decrease smoking related mortality and morbidity

15
Target population Smokers who are willing to quit Daily smokers in Hungary: 2.290.000 adults Daily smokers in Budapest: 390.000 adults Daily smokers in Pest county: 207.000 adults

16
Implementation plan Year 1. Need assessment of the target population Building up the operation of the Tobacco Cessation Centre Intense training for the counselors Training the primary care physicians (minimal intervention, referral system)
.")
17
Implementation plan Year 2-3. Running and actuation of the service Monitoring and evaluation: – clients’ satisfaction – primary care providers’ satisfaction – cost-benefit analysis

18
Outcomes of the program Primary outcomesTotal outputsType of data Large number of physicians refer their smokers At least 200 physicians will regularly refer Number of referred patients Large number of smokers will be referred At least 30.000 patients will receive intense telephone counseling and 3000 patients will participate in intense group or individual counseling Number of participants, follow up interview and registered data of the interventions 25% of patients will report continuous abstinence at month 6, and 15% at month 12 At least 8200 patients will be abstinent at month 6 and 4950 at month 12 Self report data complemented with collateral interview or biochemical validation

19
Need assessment Quantitative and qualitative research/need assessment has been carried out in order to optimize the services: – Quantitative research involved representative sample of 510 smokers from Budapest and Pest county; and 144 family physicians), Qualitative research involved focus groups (3 FGs with smokers, 2 FGs with family physicians, and 1 FG with nurses/assistants), and 15 individual interviews with family physicians
, Qualitative research involved focus groups (3 FGs with smokers, 2 FGs with family physicians, and 1 FG with nurses/assistants), and 15 individual interviews with family physicians")
20
survey among smokers Note: *: only in Budapest, and **: Budapest and Pest county

21
2009 – preparation survey among family physicians

22
Development of treatment protocols Desk research International collaboration related to best practices is built up. Participation in the 14 th WCTOH helped to build up international partnerships with other quitlines. A visit was made in the center of QUIT (London). Created a treatment protocol for individual, group and telephone counseling.
. Created a treatment protocol for individual, group and telephone counseling..")
26
Development of the information/communication system Specification was defined for the programmer. The software for the call-center and CRM has been pretested before purchase. IT management was established coordinating the system building Webpage was constructed

27
Smoking Cessation Specialists’ training – content areas Smoking and health Epidemiology of smoking including international statistics and Hungarian data Development of smoking and nicotine addiction Levels of smoking cessation supports: clinical and public health perspectives Diagnostic interview and factors that influence smoking cessation success Motivational interviewing in smoking cessation support

28
Smoking Cessation Specialists’ training – content areas Cognitive-behavioral therapy for smoking cessation Pharmacotherapy in smoking cessation support Treatment of withdrawal symptoms and relapse prevention counseling Long-term barriers of quitting: stress, weight concerns etc. Features and practices of telephone counseling Group processes - how to facilitate smoking cessation groups Special issues: adolescents, pregnant women, psychiatric population

31
Reactive and proactive service Reactive only Reactive + Proactive intense 15. Sept. 2009. 1. January 2010.

35
Proactive counseling Planned way of quitting smoking Different protocolls: 5-8 consultation 6 consultation: – Every call has its own objective: Motivational support Preparation for the quit date How to choose the quit date Dealing with withdrawal symptoms Relapse prevention Long term follow up (6 months)
")
36
Info-hub function Guiding people to local resources Pulmonologists Family physicians Psychologists/psychiatrists Other helplines Other information centres, handouts, websites

37
Website Seems to be effective, cheap, can be integrated with regular counseling. Our website offers: – Chatroom – “ask our expert” – Self help materials – Registration for proactive counseling

39
Milestones Milestone Office, basic infrastructure, call centre August 2009. Management, supporting team and backoffice August 2009. Operational program and protocols April 2009. Training of counselors22 counselors - August 2009. Training of physicians and nurses 983/480 Evaluation planNovember 2009

40
Reaching clients by the original plan The doctor/nurse informs and refers the client 1.Ask 2.Advise 3.Assess 4.Refer The ways of referring: – E-mail – Telephone – Fax – Post

41
First results in cessation counseling 488 registered on the website, – 124 involved in telephone counseling, – 30 involved in group counseling 36 referred (most of them from the “mobile screening”), 22 has started the cessation program
, 22 has started the cessation program")
42
Reaching clients – now! Website, facebook, “mobile screening – Health for a lifetime” Contacts with NGO’s of chronic patients European Network Smoke-free Hospitals Health centers Posters Midwifes

Similar presentations













 Skype What next?>")
 Gaylene Mooney, M.Ed., RRT-NPS, CTTS Program Director, Respiratory Therapy San Joaquin.>")





 Children's Art Contest. Support for the 2010 AAP.>")





