Download presentation
Presentation is loading. Please wait.

1
Physiological optics 12th lecture
Dr. Mohammad Shehadeh

2
Optics of Ametropia The ametropic eye fails to bring parallel light to a focus on the retina, i.e. the second principal focus of the eye does not fall on the retina

3
Myopia In the myopic eye, the second principal focus lies in front of the retina. Axial myopia: the eye is abnormally long. includes high myopia in which there may be a posterior staphyloma. Refractive or index myopia: the eye may be of normal length, but the dioptric power may be increased. Examples of this are keratoconus, where the corneal refractive power is increased, and nucleosclerosis, where the refractive power of the lens increases as the nucleus becomes more dense.

5
Hypermetropia In the hypermetropic eye, the second principal focus lies behind the retina Axial hypermetropia: If the eye is short relative to its focal power. Refractive hypermetropia: if the refractive power of the eye is inadequate. Aphakia is an extreme example of refractive hypermetropia.

6
Phakic patients can overcome some or all of their hypermetropia by using accommodation for distance vision. They then have to exercise extra accommodation for near vision. Because the amplitude of accommodation declines with age these patients require reading glasses at a younger age than emmetropic patients.

7
Manifest hypermetropia is defined as the strongest convex lens correction accepted for clear distance vision. Latent hypermetropia is the remainder of the hypermetropia which is masked by ciliary tone and involuntary accommodation. This may account for several dioptres, especially in children, for whom cycloplegic refraction is necessary to ascertain the full magnitude of the refractive error.

8
Facultative hypermetropia : hypermetropia which can be overcome by accommodation ,
Absolute hypermetropia: hypermetropia in excess of the amplitude of accommodation

9
Astigmatism The refractive power of the astigmatic eye varies in different meridians. The image is formed as a Sturm's conoid

10
If the principal meridians are at 90° to each other, this is called regular astigmatism.
If the principal meridians are at 90° to each other but do not lie at or near 90° and 180°, the term oblique astigmatism is used. If the principal meridians are not at 90° to each other, this is called irregular astigmatism and cannot be corrected by spectacles.

11
Retina a = Compound hypermetropic astigmatism. –
Retina a = Compound hypermetropic astigmatism – rays in all meridians come to a focus behind the retina. Retina b = Simple hypermetropic astigmatism – rays in one meridian focus on the retina, the other focus lies behind the retina. Retina c = Mixed astigmatism – one line focus lies in front of the retina, the other behind the retina. Retina d = Simple myopic astigmatism – one line focus lies on the retina, the other focus lies in front of the retina. Retina e = Compound myopic astigmatism – rays in all meridians come to a focus in front of the retina

12
Anisometropia Anisometropia: it is the condition When the refraction of the two eyes is different Small degrees of anisometropia are commonplace. Larger degrees are a significant cause of amblyopia. A disparity of more than 1 D in the hypermetropic patient is enough to cause amblyopia of the more hypermetropic eye because accommodation is a binocular function, i.e. the individual eyes cannot accommodate by different amounts. The more hypermetropic eye therefore remains out of focus. The myopic patient with anisometropia is less likely to develop amblyopia because both eyes have clear near vision. However, when one eye is highly myopic it usually becomes amblyopic. Older patients with nucleosclerosis and resulting index myopia affecting one eye more than the other may not tolerate the full spectacle correction of the more myopic eye as they are not accustomed to coping with anisometropia. However, myopic patients who have been anisometropic all their lives may tolerate higher degrees of anisometropia and achieve binocular vision with more than 2 D difference between the two eyes.

13
Pin-Hole Test Because no focused image is formed on the retina of the ametropic eye, the visual acuity is reduced. The pin- hole test is a useful method of determining whether reduced visual acuity is due to refractive error rather than ocular pathology or neurological disease. If the visual acuity is reduced by refractive error, the pin-hole acuity will be significantly better than the unaided acuity. If the reduced acuity is due to ocular pathology, there is characteristically no improvement in visual acuity with the pin-hole. In macular disease the pin-hole acuity may be even worse than the unaided acuity.

14
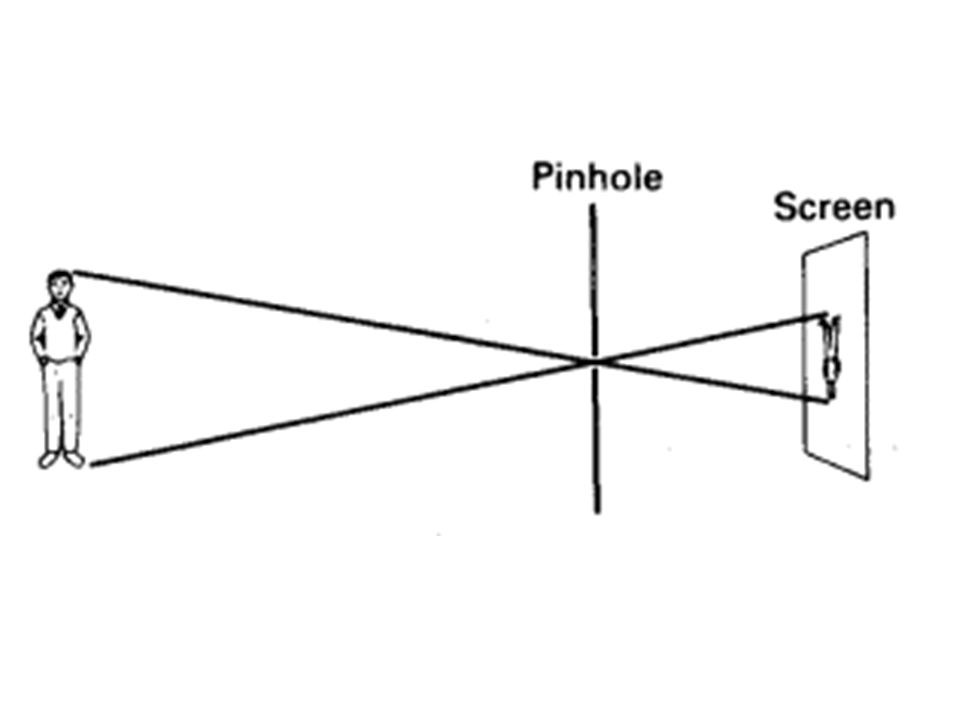
The pin-hole theoretically allows only one ray from each point on an object to pass through to the screen. Thus, a clear image is formed regardless of the position of the screen Likewise the use of the ideal pin-hole leads to the formation of a clear retinal image irrespective of the refractive state of the eye.

16
But in practice the pin-holes available clinically allow a narrow pencil of light to pass through them, rather than a single ray.

17
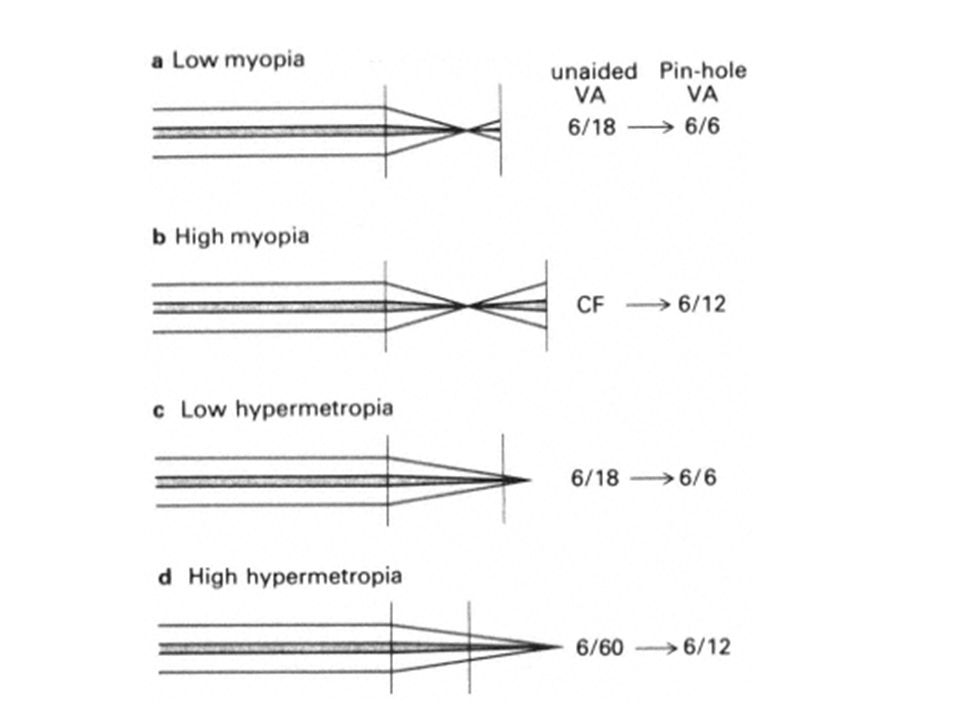
low degrees of refractive error the pin-hole's effect is sufficient to improve the clarity of the retinal image to such an extent that a good visual acuity results. However, in high degrees of ametropia, although the pin-hole helps, the retinal image is still too diffuse to achieve the improvement that is found in the case of low refractive errors. Thus errors outside the range +4 D to –4 D sphere are not corrected to 6/6 with a pin-hole.

19
Stenopaeic Slit The stenopaeic slit can be used to determine the refraction and principal axes in astigmatism. The slit aperture acts as an elongated 'pin-hole', only allowing light in the axis of the slit to enter the eye. Hence, when the slit lies in one principal axis of the astigmatic eye, the second line focus is eliminated and the blur of Sturm's conoid reduced thus allowing a clearer image to be formed

20
During the refraction of a patient with astigmatism, the slit is first rotated to a position in which the clearest vision is obtained. Spherical lenses are added to give further improvement in acuity. The slit is then rotated through 90° and the spherical lens power adjusted to give best subjective acuity. The cylindrical correction required by the eye equals the algebraic difference between the two spherical corrections used, and its axis is that of the original direction of the slit.

21
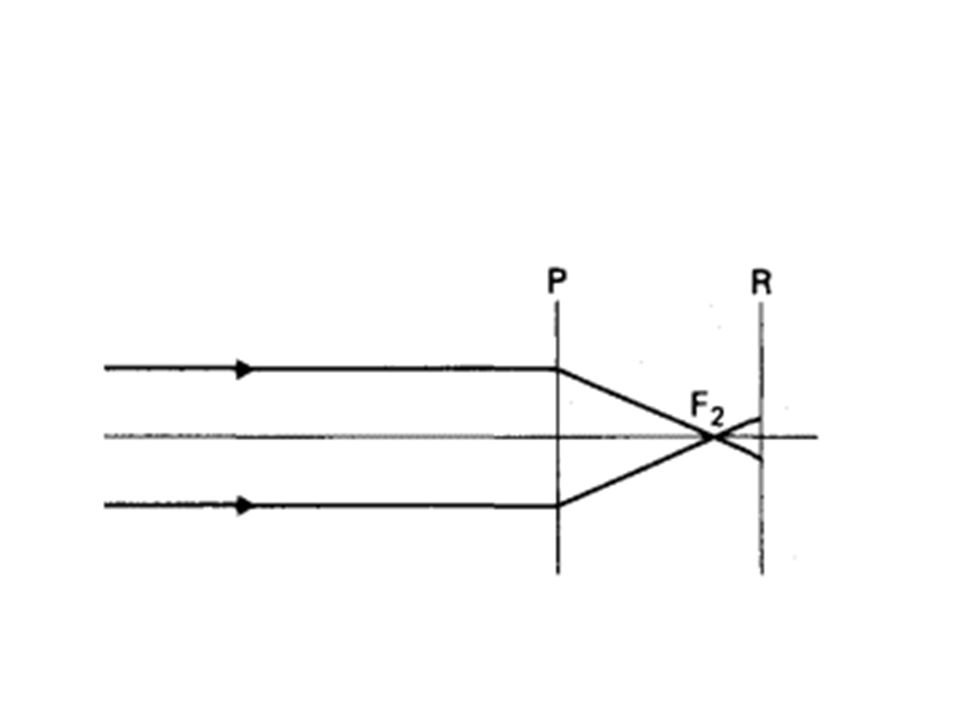
Far Point The far point (FP) of an eye is the position of an object such that its image falls on the retina of the relaxed eye, i.e. in the absence of accommodation. The distance of the far point from the principal plane of the eye is denoted by r, which according to sign convention carries a negative sign in front of the principal plane and a positive sign behind the principal plane.
 of an eye is the position of an object such that its image falls on the retina of the relaxed eye, i.e. in the absence of accommodation. The distance of the far point from the principal plane of the eye is denoted by r, which according to sign convention carries a negative sign in front of the principal plane and a positive sign behind the principal plane.")
24
Optical Correction of Ametropia
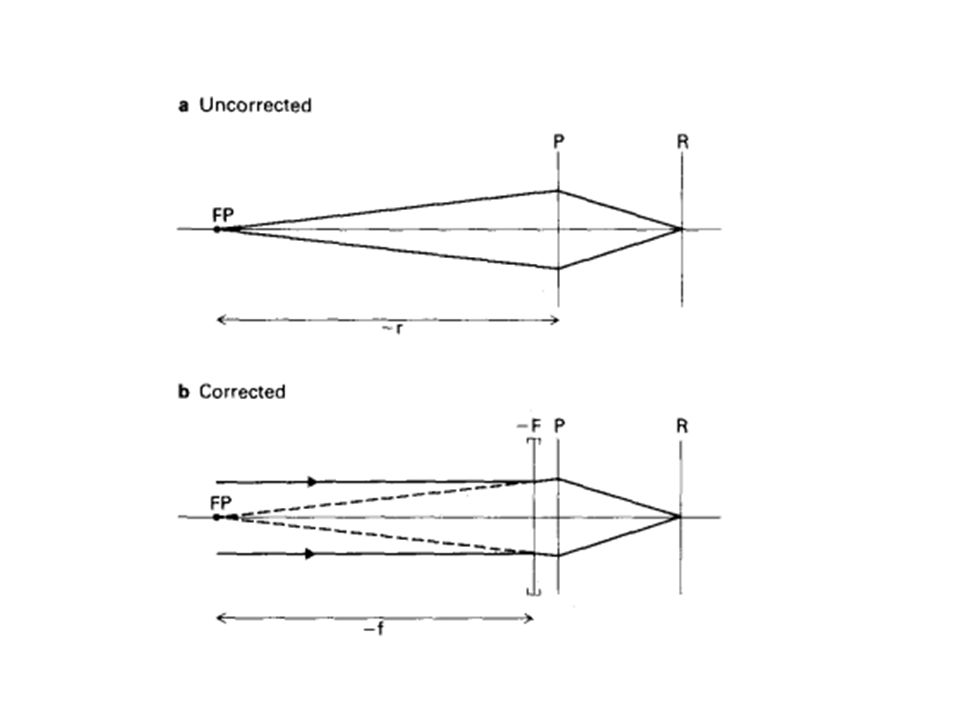
The purpose of the correcting lens in ametropia is to deviate parallel incident light so that it appears to come from the far point in myopia or to be converging towards the virtual far point in hypermetropia. The light will then be brought to a focus by the eye on the retina. Thus the far point of the eye must coincide with the focal point of the lens. The focal length, f, of the correcting lens is approximately equal to (~ ) the distance, r, of the far point from the principal plane when the correcting lens is close to the principal plane
 the distance, r, of the far point from the principal plane when the correcting lens is close to the principal plane.")
25
Thus the power of lens, F, required is
where F is the power of the lens in dioptres; f is the focal length of the lens in metres; and r is the distance of the far point from the principal plane in metres

26
The reciprocal of the far point distance r, in metres, is symbolised by R, expressed in dioptres.
R is known as the static refraction or the ametropic error.

28
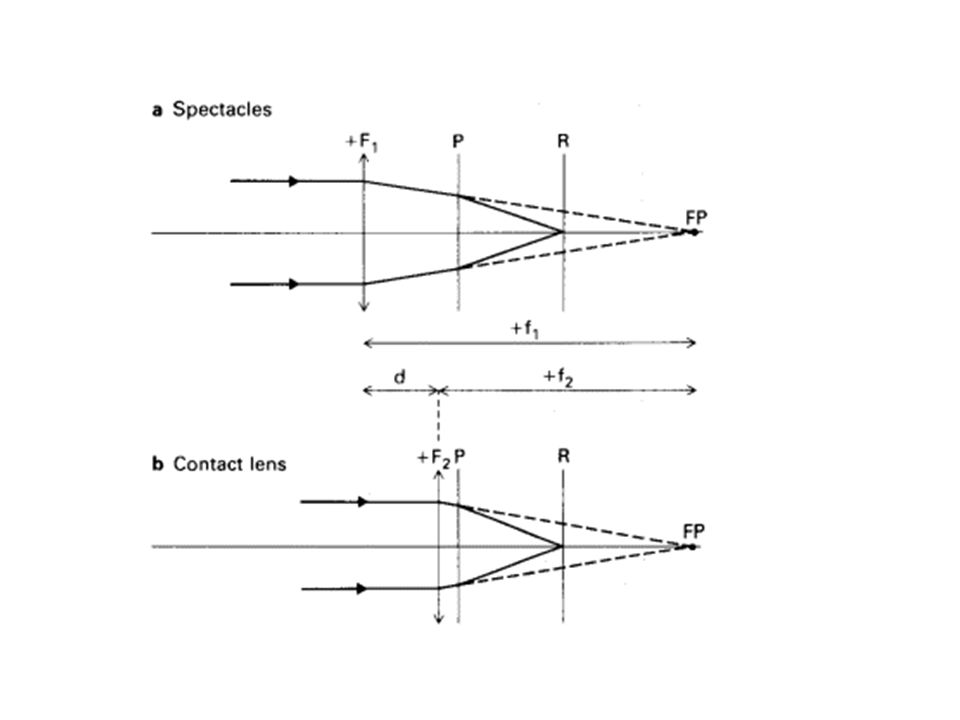
In practice, the correcting lens in ametropia is usually held in spectacles.
The lens is, therefore, some distance in front of the principal plane of the eye. The power of the lens necessary to correct a specific degree of ametropia must therefore be adjusted so that the far point and the focus of the lens still coincide

29
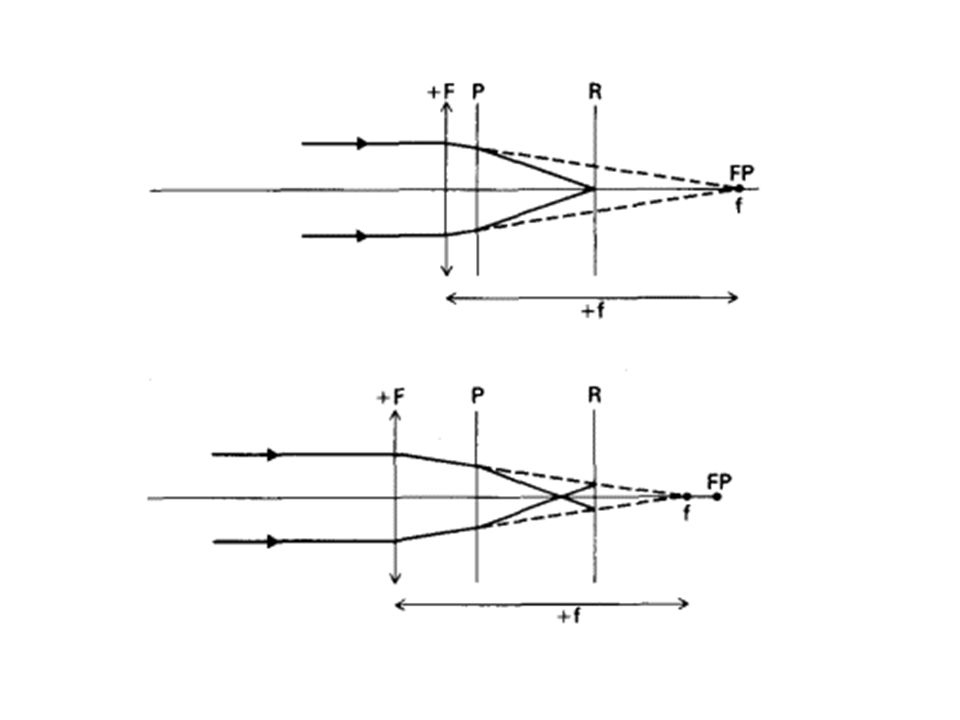
Effective Power of Lenses
If a correcting lens is moved either towards or away from the eye, its vergence power at the principal plane of the eye changes. The focus of the lens and the far point of the eye no longer coincide

32
It can also be seen from the diagrams that, on moving either a convex or a concave lens away from the eye, the image is moved forward. In the uncorrected hypermetropic eye the image falls behind the retina. The purpose of the correcting convex lens is to bring the image forward on to the retina. When the correcting lens is moved further away from the eye the image is brought still further forward. Thus the effectivity of the lens is said to be increased. Therefore in this position a weaker convex lens throws the image onto the retina and corrects the hypermetropia.

33
In the myopic eye the image falls in front of the retina.
The purpose of the correcting concave lens is to take the image back on to the retina. When the correcting lens is moved further away from the eye, the image moves forward again. Thus the effectivity of the lens is said to be reduced. Therefore, in this position, a stronger concave lens is needed to throw the image on to the retina.

34
In practice, patients with strong convex lenses, especially those who are aphakic, sometimes pull their glasses down their nose in order to read. The enhanced effectivity thus produced is sufficient to provide the reading correction. Also, myopes dislike their glasses slipping down their nose (as they tend to do if heavy glass lenses are used) as this makes the correction less effective.
 as this makes the correction less effective.")
35
Thus, to correct a specific degree of ametropia, the power of the correcting lens must be adjusted to take into account its position in front of the eye

36
where F2 is the power of lens in dioptres required at the new position; f1 is the focal length in metres of the original lens; and d is the distance moved in metres The value of d is positive if the lens is moved towards the eye, and negative if moved away from the eye. The usual sign convention applies to the lens.

37
Mathematically the above formula can also be expressed as
where F1 is the dioptric power of the original lens

40
Practical Application:
Back Vertex Distance For any lens of power greater than 5 dioptres, the position in front of the eye materially affects the optical correction of ametropia. This is especially true in aphakia where high power lenses are prescribed. For this reason the refractionist must state how far in front of the eye the trial lens is situated so that the dispensing optician can adjust the lens power if a contact lens is to be used, or if spectacles are to be worn at a different distance, e.g. because of a high-bridged nose or deep-set eyes.

41
Therefore any high powered lens should be placed in the back cell of the trial frame and the distance between the back of the lens and the cornea measured. This is called the back vertex distance (BVD) and must be given with all prescriptions over 5 dioptres. The measurement may be made with a ruler held parallel to the arm of the trial frame. Other means include a small rule which is slipped through a stenopaeic slit placed in the back cell of the trial frame until it touches the closed eyelid. Two millimetres must be added to the measurement to correct for the thickness of the lid.
 and must be given with all prescriptions over 5 dioptres. The measurement may be made with a ruler held parallel to the arm of the trial frame. Other means include a small rule which is slipped through a stenopaeic slit placed in the back cell of the trial frame until it touches the closed eyelid. Two millimetres must be added to the measurement to correct for the thickness of the lid.")
42
Example 1 Refraction shows that an aphakic patient requires a +10
Example 1 Refraction shows that an aphakic patient requires a D lens at BVD 15 mm. He needs a contact lens (F2)
")
43
Example 2 Likewise a high myope whose spectacle correction is –10
Example 2 Likewise a high myope whose spectacle correction is –10.0 D at BVD 14 mm requires a contact lens (F2)
")
Similar presentations





















![L 33 Light and Optics [3] images formed by mirrors](/15/4681859/big_thumb.jpg "L 33 Light and Optics [3] images formed by mirrors>")

