Download presentation
Presentation is loading. Please wait.

1
ACUTE OTITIS MEDIA

2
OTITIS MEDIA Huyønh Khaéc Cöôøng , M.D.
Senior Lecturer – Otolaryngology Department University UMP at HoChiMinh City

3
Otitis Media Otitis media is one of the most common diagnoses among children Nat’l Ambulatory Medical Care Surveys data indicate that the number of office visits for OM increased by more than 2-fold from This survey estimated over 5.18 million episodes of AOM in 1995 at a cost of $2.98 billion

4
Acute Otitis Media OTITIS MEDIA = inflammation of the middle ear, is defined by the presence of fluid in the middle ear accompanied by signs or symptoms of acute illness. The peak incidence occurs in the first 3 years of life. The disease is less common in the school-aged child, adolescents, and adults. Nevertheless, infection of the middle ear may be the cause of fever, significant pain, and impaired hearing in these age groups.

5
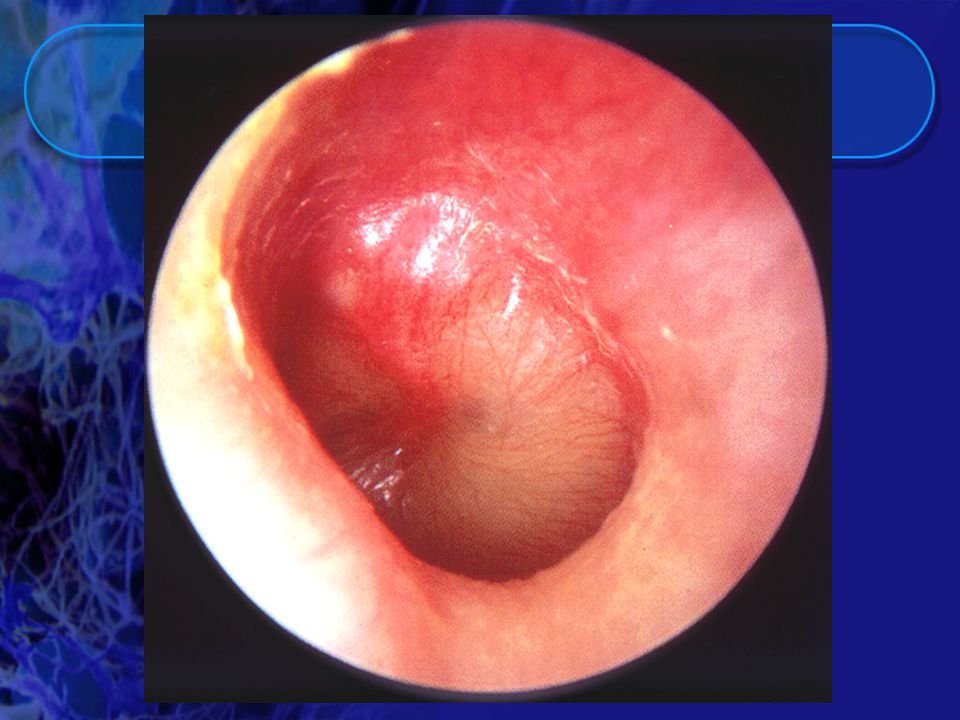
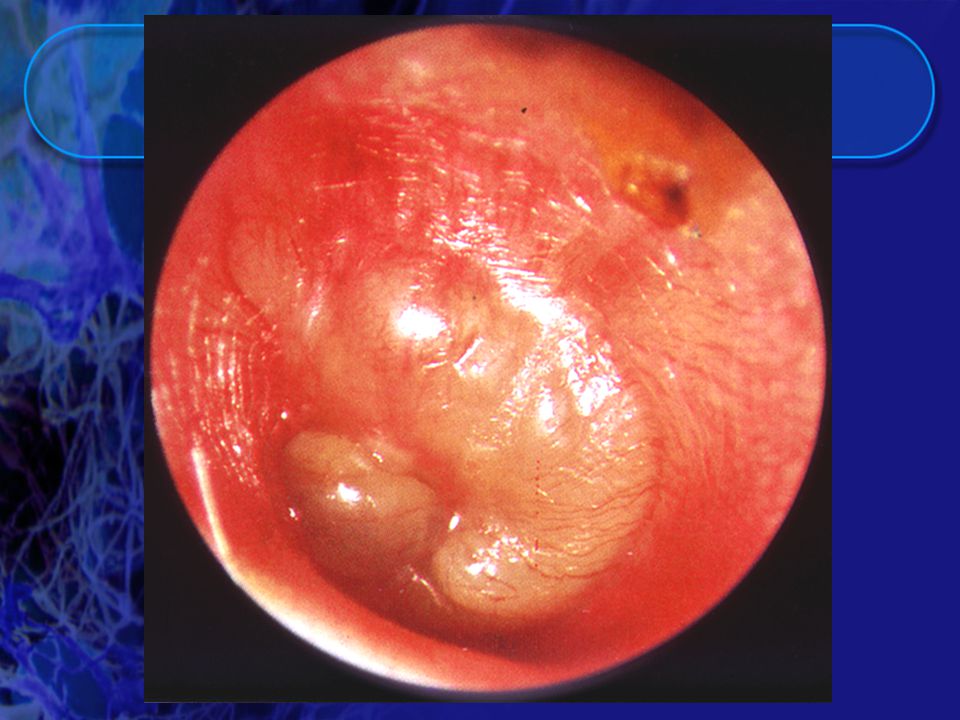
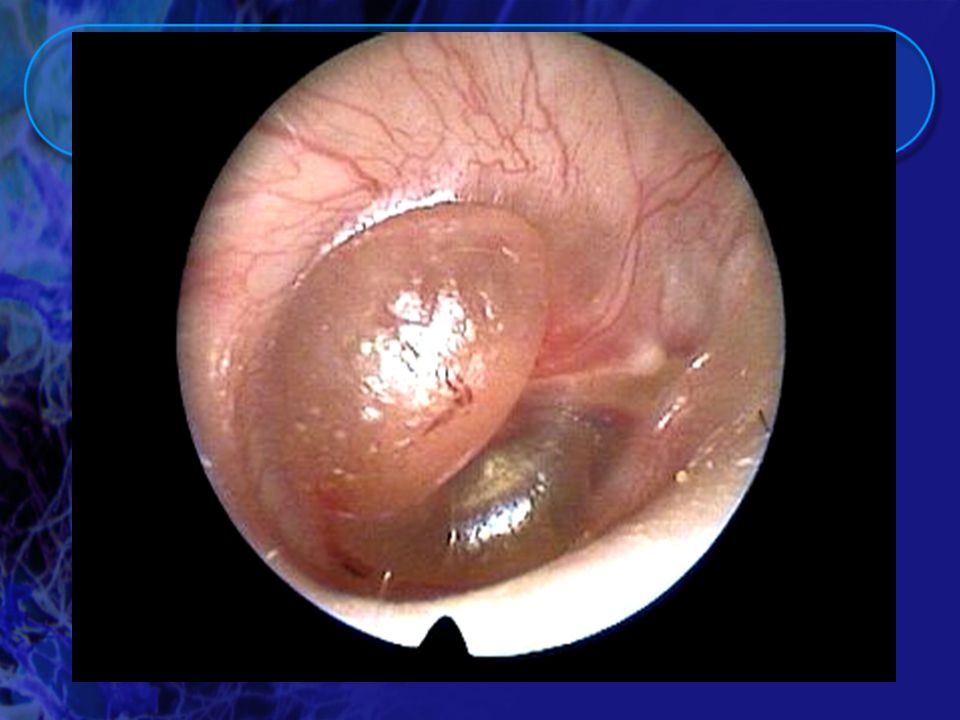
Definitions Acute Otitis Media with Effusion (AOME):
suppurative infection of the middle ear sudden onset short duration the inflamed tympanic membrane is bulging and/or opacified

6
Definitions Chronic Otitis Media (COM)
COM with Effusion or nonsuppurative OM : Middle ear effusion behind an intact eardrum Persist for more than 2-3 months Asymptomatic except for hearing loss No acute symptoms May follow AOM

7
Definitions Chronic Suppurative Otitis Media (CSOM):
chronic perforation of the TM purulent discharge for >6 weeks insidious onset may follow AOM

8
Otitis Media Epidemiology
Most common bacterial infection in children and most commonly diagnosed Half of all children will have an episode before the first birthday, and 80% before the third birthday The most frequent reason for prescribing antibiotics

9
Otitis Media Epidemiology
It accounts for more than 1/3 of office visits to pediatricians each year The number of office visits continues to rise, in 1997 it reached 25.9 billion 4-5 billion dollars spent each year in direct care costs

10
Pathogenesis The vast majority of children have no obvious defect responsible for severe and recurrent otitis media, but a small number have anatomic changes (cleft palate, cleft uvula, submucous cleft), alteration of normal physiologic defenses (patulous eustachian tube), or congenital or acquired immunologic deficiencies.
, alteration of normal physiologic defenses (patulous eustachian tube), or congenital or acquired immunologic deficiencies.")
11
Pathophysiology and Risk Factors for Infection
The introduction of infants into large day care groups increases the incidence of respiratory infections, including otitis media. Almost one episode of respiratory tract infections a month occurs during the first year of life, and AOM is a complication of about one third to one half of the respiratory tract infections.

12
Pathophysiology and Risk Factors for Infection
Passive smoking increased the incidence of new episodes of otitis media with effusion and the duration of effusion. The age at the time of the first episode of AOM appears to be among the most powerful predictors of recurrent middle ear infections. Breast-feeding for 3 or more months is associated with a decreased risk of AOM in the first year of life.

13
Caùc Yeáu Toá Beänh Caên Hoïc cuûa VIEÂM TAI GIÖÕA CAÁP TÍNH

14
Otitis Media Risk Factors
Host factors Environmental factors

15
Otitis Media Host Factors
Age < 2 years Gender ( Males > Females) Race (Native Americans, Alaskan>AA and Caucasian) Genetic predisposition Sibling with history of recurrent disease Down’s syndrome, cleft palate, tumors, immunodeficiency states
 Race (Native Americans, Alaskan>AA and Caucasian) Genetic predisposition. Sibling with history of recurrent disease. Down’s syndrome, cleft palate, tumors, immunodeficiency states.")
16
Otitis Media Environmental Factors
Allergies Second hand smoke + wood burning stoves Not breastfeeding Seasonal Large group day care Low socioeconomic group Use of pacifiers

17
Otitis Media Natural History
Upper respiratory tract mucosal congestion spreads to eustachian tube obstruction leading to stasis, effusion and multiplication of bacteria Spontaneous resolution with drainage via the eustachian tubes or with perforation of the tympanic membrane Effusion may remain if tube still obstructed

18
Etiology Virologic and epidemiologic data suggest that viral infection is frequently associated with AOM. Recent studies identify respiratory viruses or viral antigens in approximately one quarter of middle ear fluids of children with AOM. Respiratory syncytial virus, influenza virus, enteroviruses, and rhinoviruses = most common viruses found in middle ear fluids. Many patients with virus in middle ear fluid have a mixed viral-bacterial infection.

19
Etiology The bacteriology of otitis media has been documented by appropriate cultures of middle ear effusions obtained by needle aspiration. S. pneumoniae is the most important bacterial cause of otitis media . Relatively few types are responsible for most disease ; the most common types in order of decreasing frequencies are 19, 23, 6, 14, 3, and 18. All are included in the currently available 23-type PNEUMOCOCCAL POLYSACCHARIDE VACCINE.

20
Etiology Otitis media due to H. influenzae is associated with nontypable strains in the vast majority of patients. In 12 reports from the United States, Finland, and Canada, M. catarrhalis was isolated from a mean of 10% of children with AOM (range 2 to 15%).
.")
21
Signs and Symptoms AOM is defined by the presence of fluid in the middle ear along with signs or symptoms of acute illness. Signs and symptoms may be specific, such as ear pain, ear drainage, or hearing loss, or may be nonspecific, such as fever, lethargy, or irritability. Vertigo, nystagmus, and tinnitus may occur.

25
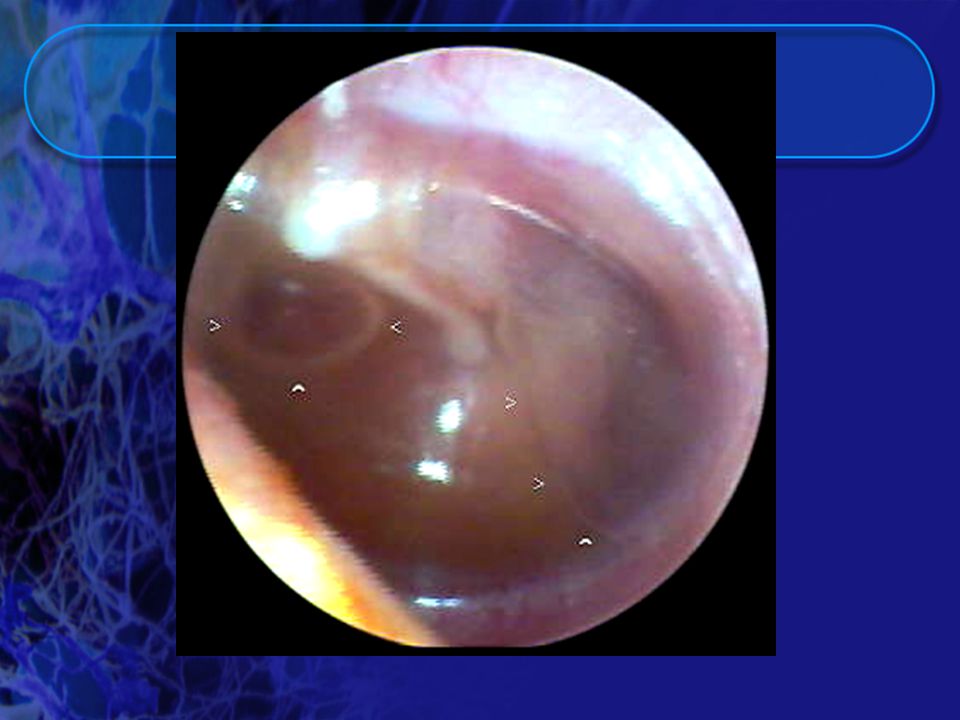
Signs and Symptoms Redness of the tympanic membrane is an early sign of otitis media, but erythema alone is not diagnostic of middle ear infection since it may be caused by inflammation of the mucosa throughout the upper respiratory tract (the so- called “red reflex”). The presence of fluid in the middle ear is determined by the use of pneumatic otoscopy, a technique that permits an assessment of the mobility of the tympanic membrane.
. The presence of fluid in the middle ear is determined by the use of pneumatic otoscopy, a technique that permits an assessment of the mobility of the tympanic membrane.")
29
Otitis Media Signs & Symptoms
Specific signs otalgia otorrhea hearing loss vertigo Nonspecific signs fever irritability lethargy anorexia vomiting diarrhea

30
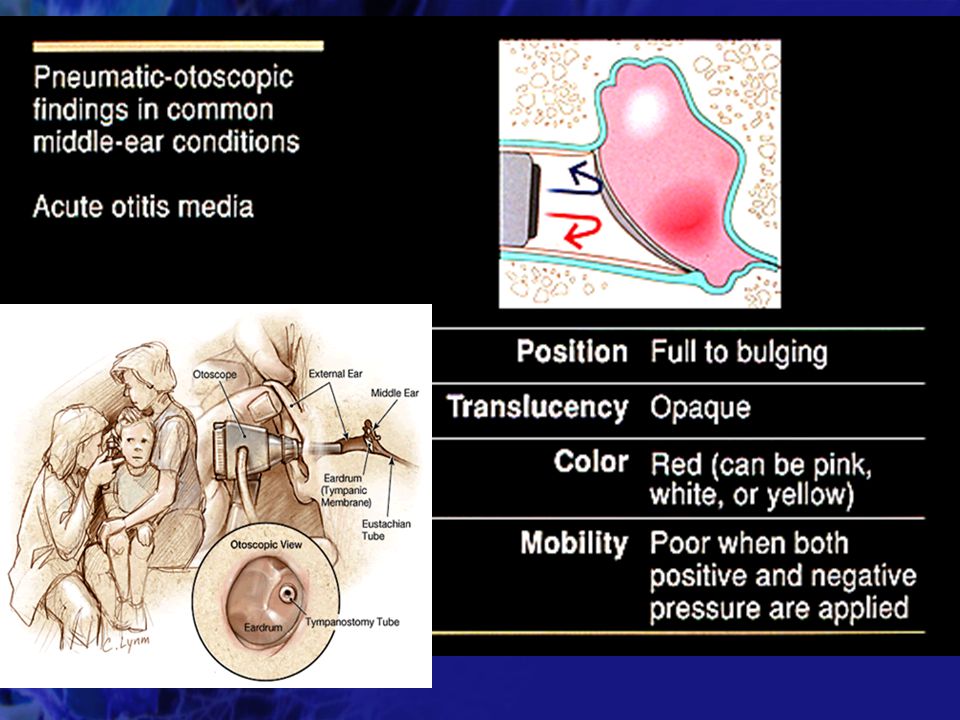
Otitis Media : Pneumatic Otoscopy
Used to assess the landmarks, mobility, color, transparency, vascularity and position of the tympanic membrane Fluid levels or bubbles can be seen if membrane is translucent Confirms middle ear effusion by assessing mobility when + or – pressure is applied Needs an adequate seal with ear canal

31
Acute Otitis Media Diagnosis
Identification of middle ear effusion pneumatic otoscopy tympanometry acoustic reflectometry Signs or symptoms of acute local or systemic illness

32
OM : Short Term Complications
Intratemporal : mastoiditis labrynthitis facial nerve paralysis petrositis hearing loss subperiosteal abscess Intracranial : meningitis lateral sinus thrombosis brain abscesses sigmoid sinus thrombophlebitis

33
OM Long Term Complications
Speech and Language delay Tympanic membrane perforation Cholesteatoma Tympanic membrane retraction pockets Hearing loss Chronic otorrhea Cognitive impairment

34
Otitis Media Etiology S. Pneumoniae 32% H. Influenzae 22%
M. Catarrhalis 16% Group A Strep 5% Staph Aureus 2% Negative culture/ 25% non pathogens

35
Otitis Media : Antimicrobial Resistance
S. pneumoniae 30-40% penicillin resistant H. influenzae 30-40% -lactamase positive M. catarrhalis 80-90% -lactamase (+) Levels of resistance vary with different geographic areas
 Levels of resistance vary with different geographic areas.")
36
Resistance Patterns in the Common Bacterial Pathogens
Pneumococcus: variable resistance to penicillin is found including both high level and intermediate level resistance. H. influenzae: increasing beta-lactamase production , up to 80% in some areas M. catarrhalis: nearly universal beta- lactamase production

37
Guidelines for the use of Antibiotics in AOM
Rationale for the continued use of amoxicillin : S. pneumoniae is responsible for about 40% of cases of AOM. Concentrations of amoxicillin can be achieved in the middle ear fluid sufficient to sterilize all but highly resistant strains. Less than 10% of pneumococci isolated from the nasopharynx of Boston children are high level resistant (MIC’s>2 mug/ml) and treatment in about 4% of all children with acute otitis might fail if they are treated with regular doses of amoxicillin (40 mg/kg/day).
 and treatment in about 4% of all children with acute otitis might fail if they are treated with regular doses of amoxicillin (40 mg/kg/day).")
38
Guidelines for the use of Antibiotics in AOM
The recent recommendation of doubling the dose of amoxicillin to 80 mg/kg/day will achieve higher concentrations in middle ear fluid and further reduce the number of children in whom amoxicillin therapy will fail because of resistant pneumococci.

39
Guidelines for the use of Antibiotics in AOM
H. influenzae and M. catarrhalis are responsible for about 30 and 10% of AOM cases, respectively. If 30% of H Flu and 75% of M. cat are b-lactamase +, then 16% of AOM cases are caused by beta-lactamase-producing organisms. If 50% improve spontaneously or despite beta-lactamase activity, then less than 10% of the failures could be anticipated to be due to failure of amoxicillin to be active against beta-lactamase-producing organisms.

40
Second Line Therapy CHOICES:
Augmentin® (adds coverage for beta-lactamase producing organisms) Cefuroxime axetil; cefpodoxime; azithromycin; ceftriaxone IM injection
 Cefuroxime axetil; cefpodoxime; azithromycin; ceftriaxone IM injection.")
41
To treat or not to treat ? Previous studies have shown that the majority of cases of AOM will resolve without specific therapy Antibiotic usage varies from 31% in the Netherlands to 98% in the US and Australia Cockrane Abstract : review of evidence-based literature to assess the effects of antibiotherapy in AOM

42
Cockrane Abstract : review of evidenced based literature to assess the effects of antibiotics in children with AOM 10 randomized trials comparing antimicrobial agents to placebo in children with AOM Total of 2,202 children Pain: No reduction in pain at 24 hours with antibx 28% relative reduction in pain at 2-7 days Since ~ 80% of cases will have resolved in this time, this represents an absolute reduction of about 5%

43
Cockrane Abstract : review of evidenced based literature to assess the effects of antibiotics in children with AOM Other Effects: No effect on hearing problems (as measured by tympanometry and audiometry in two studies only) No influence on other complications or recurrences Complications: One case of mastoiditis occurred (in PCN treated group)
 No influence on other complications or recurrences. Complications: One case of mastoiditis occurred (in PCN treated group)")
44
What can we do ? Increase the accuracy of AOM diagnosis
Understand societal pressures for antibiotic prescriptions and educate parents about appropriate use of antibiotics Evaluate non-antimicrobial treatments or preventives (e.g. vaccines)
")
Similar presentations










>")





. >")
 is inflammation.>")


