Download presentation
Presentation is loading. Please wait.

2
Christoph Lange & Giovanni Sotgiu Principles of designing a TB and MDR-TB drug regimen

3
41 y.o. Ethopian male Air plane engineer 14 d fever, night sweats TST 18 mm CXR: lymphadenopathy TCT: lymphadenopathy endosonography/cardia: -epithelioid-cell granuloma Started HREZ therapy Case presentation

4
2.5 months later: Hospital admission with ongoing fever and persistent mediastinal lymphadenopathy sputum and BAL: - AFB-negative mediastinal Bx: - no pathology seen in LN Bone marrow Bx: - „inflammation“, no granulomas, no lymphomas

5
Case presentation Day 4 in hospital: Continuation of Tx with HR Day 14 in hospital: GI-bleeding from cardia erosion Day 14 in hospital: MTB-culture from sputum + again HRZE therapy Day 15 in hospital: TCT: miliary pattern

6
Case presentation D 70D 90

7
Case presentation Day 16 in hospital: Transfer to a department of surgery because of repeated GI bleeding Day 16-24 in hospital: Repeated attempts for arterial embolization Day 22 in hospital: Preliminary result of drug resistance testing

9
Case presentation Day 22 in hospital: Change of the therapy to moxifloxacin, capreomycin, linezolid, terizidone und protionamide Day 16 in hospital: The patient dies due to GI bleeding despite mass transfusions Greinert et al. Med Klin 2007

10
Donald et al. NEJM 2009 MDR- and XDR- tuberculosis

11
Definition of MTB drug resistance Mono-drug-resistenceResistance against one (first- line) drug, INH, RMP, EMB, PZA Uncomplicated treatment. Duration of treatment may be prolonged Poly-drug-resistanceResistance against > 1 (first- line) drugs, but sensitivity to INH and/or RMP Usually uncomplicated treatment. Duration of treatment is is prolonged Multi-drug-resistance MDR Resistance against at least INH and RMP Complicated treatment. Duration of treatment is prolonged to > 18 months Outcome depends on level of drug resistance Extensively-drug-resistance XDR MDR plus resistance to - any fluoroquinolone - amikacin, capreomycin or kanamycin Complicated treatment. Duration of treatment is prolonged to > 24 months Outcome depends on level of drug resistance
 drugs, but sensitivity to INH and/or RMP Usually uncomplicated treatment. Duration of treatment is is prolonged Multi-drug-resistance MDR Resistance against at least INH and RMP Complicated treatment. Duration of treatment is prolonged to > 18 months Outcome depends on level of drug resistance Extensively-drug-resistance XDR MDR plus resistance to - any fluoroquinolone - amikacin, capreomycin or kanamycin Complicated treatment. Duration of treatment is prolonged to > 24 months Outcome depends on level of drug resistance.")
12
Drugs for the treatment against tuberculosis WHO 2009

13
Standard TB drug regimen for new cases

14
Re-treatment regimen for previous treated cases

15
Drug resistance in strains of MDR and XDR- TB in Germany 2004-2006 Eker et al. Emerg Infec Dis 2008

17
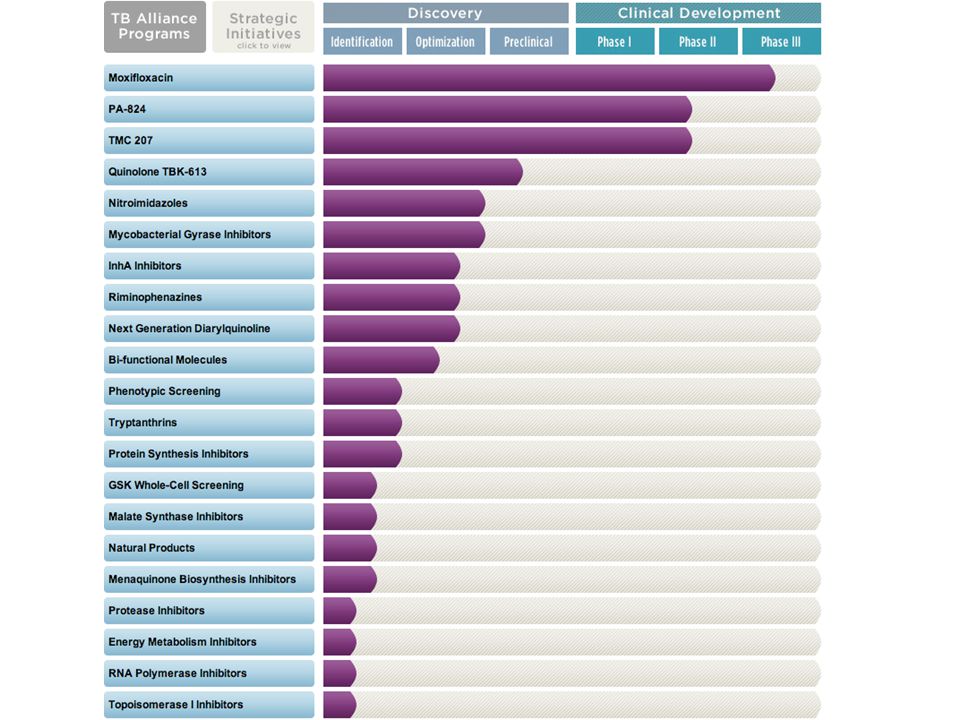
www.tballiance.org
18
Conde et al. Lancet 2009 n = 74 n = 72 Moxifloxacin for the treatment against tuberculosis

19
Dormann et al. AJRCCM 2009

20
Migliori et al. ERJ 2008 FLQ-drug resistance of M. tuberculosis is associated to treatment failure and death in MDR-TB

21
FLQ-drug resistance of M. tuberculosis in Mumbai, India Agrawal et al. IJTLD 2009

22
Diarylquinoline TMC207 for the treatment against MDR-tuberculosis Diacon et al. NEJM 2009

23
Migliori et al. ERJ 2009 Linezolid for the treatment against MDR- tuberculosis: adverse events

24
7 steps of drug treatment in MDR/XDR-tuberculosis 1.Use drugs shown to be sensitive in in vitro drug sensitivity testing. 2.Drugs are added until n > 5 3.Use any first line oral agent to which the organism is sensitive: Isoniazid, rifampin, ethambutol, pyrazinamide 4.Use an injectable drug (aminoglycoside or capreomycin) to which the organism is sensitive. Continue the injectable drug at least 6 months after culture conversion since it is frequently one of only two bactericidal components in the therapy 5.Use a fluoroquinolone. Consider use of moxifloxacin in cases of drug resistance to ciprofloxacin or levofloxacin 6.Add as many second line drugs as are needed to reach a number of > 5. Cycloserin and ethionamid are considerd first choice. PAS and linezolid are used in cases with highr- grade drug resistance 7.If the regimen does not contain > 5 adequate drugs consider the additional use of amoxicilin/clavulanic acid or clofazimine
 to which the organism is sensitive. Continue the injectable drug at least 6 months after culture conversion since it is frequently one of only two bactericidal components in the therapy 5.Use a fluoroquinolone. Consider use of moxifloxacin in cases of drug resistance to ciprofloxacin or levofloxacin 6.Add as many second line drugs as are needed to reach a number of > 5. Cycloserin and ethionamid are considerd first choice. PAS and linezolid are used in cases with highr- grade drug resistance 7.If the regimen does not contain > 5 adequate drugs consider the additional use of amoxicilin/clavulanic acid or clofazimine.")
25
Conclusions Drug resistant strains of MTB are increasing worldwide Causes for the emergence of MTB drug resistance are variable (healthcare mismanagment, unavailability of drugs, direct transmission of MTB resistant strains in vulnerable populations) The treatment prognosis is dependant upon the level of drug resistance and the availability of second line drugs Therapy of MDR/XDR TB is longlasting (> 18 months) and frequently requires modifications due to adverse effects of the drugs There is a need for biomarkers to predict the duration of therapy in individual patients There is a need for the development of new drugs against MTB but not much is changing for now
 The treatment prognosis is dependant upon the level of drug resistance and the availability of second line drugs Therapy of MDR/XDR TB is longlasting (> 18 months) and frequently requires modifications due to adverse effects of the drugs There is a need for biomarkers to predict the duration of therapy in individual patients There is a need for the development of new drugs against MTB but not much is changing for now")
Similar presentations