Download presentation
Presentation is loading. Please wait.

1
‘Resistant infections’ 22.03.13 Dr Julian Sutton Consultant in Infectious Diseases & Medical Microbiology

2
Case 1 21F N fit & well Admitted via ED to ICU Hypoxia CRP 470, neutrophilia (17) normotensive# CXR R-sided consolidation Empiric Rx for CAP – iv benpen & clarythromycin & oseltamivir
 normotensive# CXR R-sided consolidation Empiric Rx for CAP – iv benpen & clarythromycin & oseltamivir")
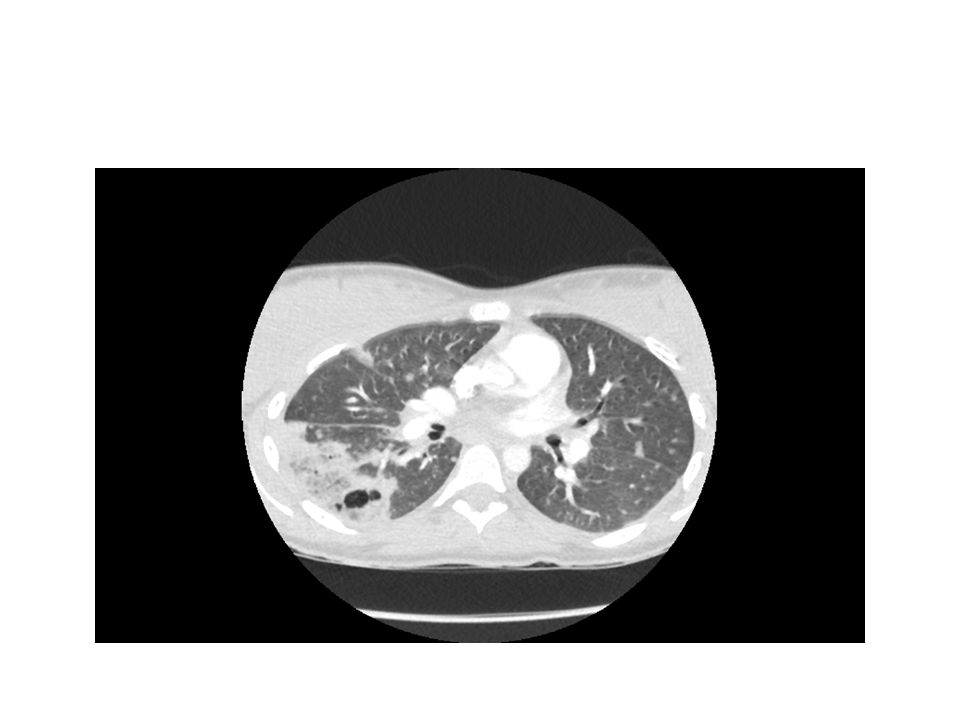
3
Initial CXR

6
Admission blood cultures positive ‘GPC ? Staph’ in both bottles CA-BSI PVL- MRSA bacteraemia and cavitating pneumonia Rx changed to include clindamycin, rifampicin and Linezolid 2-3 week admission – complicated by rash and deraanged LFTs Good respiratory recovery

7
S. aureus bacteraemia at UHS, 2006-2012 COMMUNITYHOSPITAL YearResistantSensitive Total Community Acquired Isolates % of Community Isolates Resistant to Rifampicin ResistantSensitive Total Hospital Acquired Isolates % of Hospital Acquired Isolates Resistant to Rifampicin MRSA 2006018 0%251534% 2007010 0%030 0% 20080330%013 0% 20090440%044 20100440%077 20110660%12333% 20120440%011 Mean Resistance 0% 5% MSSA 2006040 0%068 0% 2007147482%053 0% 2008044 0%040 0% 2009037 0%022 0% 2010150512%025 0% 2011056 0%023 0% 2012155562%031 0% Mean Resistance 1% 0% Combined MRSA & MSSA 2006058 0%21191212% 2007157582%083 0% 2008047 0%053 0% 2009041 0%026 0% 2010154552%032 0% 2011062 0%125264% 2012159602%032 0% Mean Resistance 1% 2012 - 92 S. aureus bacteraemias -64% were community-acquired) 86 MSSA, 6 MRSA (6.5%)
 86 MSSA, 6 MRSA (6.5%).")
8
Bilateral breast abscess surgically drained, 4 weeks post partum (30.04.12) ‘bilateral basal atelectasis’
 ‘bilateral basal atelectasis’")
9
Extensive bilateral basal and posterior consolidation with air bronchogram and shallow reactive pleural effusions

10
MSSA-PVL positive bilateral pneumonia and bilateral breast abscesses

11
Antibacterial gents for select resisttant gram positive organisms Glycopeptides - Vancomycin and Teicoplanin Linezolid Daptomycin Rifampicin Clindamycin

13
Streptococcus pneumoniae

14
Burden of pneumococcal disease at UHS over 9 years

16
MDR-TB and XDR-TB MDR-TB is defined as resistance to isoniazid and rifampicin, with or without resistance to other first-line drugs (FLD). XDR-TB is defined as resistance to at least isoniazid and rifampicin, and to any fluoroquinolone, and to any of the three second-line injectables (amikacin, capreomycin, and kanamycin). Within a year of the first reports of XDR-TB, isolated cases were reported in Europe that had resistance to all first-line anti-TB drugs (FLD) and second- line anti-TB drugs (SLD) that were tested.[3,4,5] In 2009, a cohort of 15 patients in Iran was reported which were resistant to all anti-TB drugs tested.[6] The terms “extremely drug resistant” (“XXDR-TB”) and “totally drug-resistant TB” (“TDR-TB”) were given by the respective authors reporting on this group of patients. Recently, a further 4 patients from India with “totally drug resistant” tuberculosis (“TDR-TB”) were described [7], with subsequent media reports of a further 8 cases.[8]
. Within a year of the first reports of XDR-TB, isolated cases were reported in Europe that had resistance to all first-line anti-TB drugs (FLD) and second- line anti-TB drugs (SLD) that were tested.[3,4,5] In 2009, a cohort of 15 patients in Iran was reported which were resistant to all anti-TB drugs tested.[6] The terms extremely drug resistant ( XXDR-TB ) and totally drug-resistant TB ( TDR-TB ) were given by the respective authors reporting on this group of patients. Recently, a further 4 patients from India with totally drug resistant tuberculosis ( TDR-TB ) were described [7], with subsequent media reports of a further 8 cases.[8].")
19
The Global threat of Multidrug resistant TB October 2012

20
Health Protection Agency, UK data on MDR TB October 2012

21
Clinical case 26 year old, female Born Bangladesh, married, moved to UK 2004 PMH Pulmonary TB Rx in Bangladesh 2004 Rx with 3 drugs Total duration Rx said to be 6 months, including ‘injections’ for 1st 3 months Miscarriages 2005 + April 2006 LMP 8 weeks ago

22
Clinical case 5/12 hx –Cough Saw GP –CXR R apical consolidation with cavity formation –Referred to local Respiratory clinic –Sputum AAFB positive –Commenced on conventional quadruple anti- tuberculous Rx rifinah, pyrazinamide, ethambutol 19.09.06 Initial susceptibilities available 05.10.06

23
Clinical case - Investigations Hb 12.5 Plts 508 WBC 7.8 neuts 4.5 lymphs 2.5 Clotting N; fibrinogen 4.12; ESR 64 Na 138 K 4.2 U 2.4 Creat 60 Alb 37 TP 72 globulins 35 AST 44, otherwise normal LFTs, incl ALT CRP 3 Urine pregnancy test positive; lab -hcg 16,000

24
Clinical case - Investigations CXR 18.08.06 –RUL opacification with thick wall cavity and septation within the upper lobe –L lung clear

25
Mycobacterium tuberculosis Susceptibilities Resistant –Rifampicin, Isoniazid, Ethambutol, Streptomycin Sensitive –Pryrazinamide, Ciprofloxacin

26
Initial Management… Isolate in negative pressure sideroom Stop all TB Rx Await further sensitivities Involve Obstetric team and Cardiothoracic team

27
BTS guidelines MDR TB Rx with 5 or more drugs to which organism is, is is likely to be, susceptible, until sputum cultures negative Continue with at least 3 drugs to which organism is susceptible, for minimum of 9 further months, perhaps up to or beyond 24 months Negative pressure isolation until deemed non-infectious All treatment (inpatient and outpatient) should be fully supervised
 should be fully supervised")
28
Agents available to use in this case... Pyrazinamide Moxifloxacin Cycloserine Capreomycin Ethionamide PAS Amikacin Clarithromycin

29
Widespread pneumonia. Decreased air entry at the bases. Cough and fever. Rule out TB Pneumonia. There is miliary shadowing seen bilaterally throughout both lungs. There is a moderately large rightsided pleural effusion.. Appearances are consistent with miliary tuberculosis.

Similar presentations





 Active TB Routine; FBE WCC (Infection) Hb (Anaemic of chronic disease) U&Es (baseline) LFTs (baseline) ESR/CRP (inflammation/infection)>")


















