Download presentation
Presentation is loading. Please wait.

1
﴿و ما أوتيتم من العلم إلا قليلا﴾
بسم الله الرحمن الرحيم ﴿و ما أوتيتم من العلم إلا قليلا﴾ صدق الله العظيم الاسراء اية 58

2
Physiology of Micturition Lecturer of Medical Physiology
By Dr. Abdel Aziz M. Hussein Lecturer of Medical Physiology Member of American Society of Physiology

3
Micturition Def., It is the periodic evacuation of the urinary bladder through the urethra.

4
Urinary Bladder

5
Physiological anatomy of urinary bladder
Site: The urinary bladder is a hollow, muscular and distensible or elastic organ that sits on the pelvic floor (superior to the prostate in males).
.")
6
Urinary Bladder in Male

7
Physiological anatomy of urinary bladder
Shape and Size: The size and shape of the urinary bladder varies with the amount of urine it contains and with pressure it receives from surrounding organs.

8
Physiological anatomy of urinary bladder
Parts: We can divide urinary bladder into: Body: which is the major part in which the urine collects Neck (posterior urethra): funnel-shaped that connects to urethra
: funnel-shaped that connects to urethra.")
10
Physiological anatomy of urinary bladder
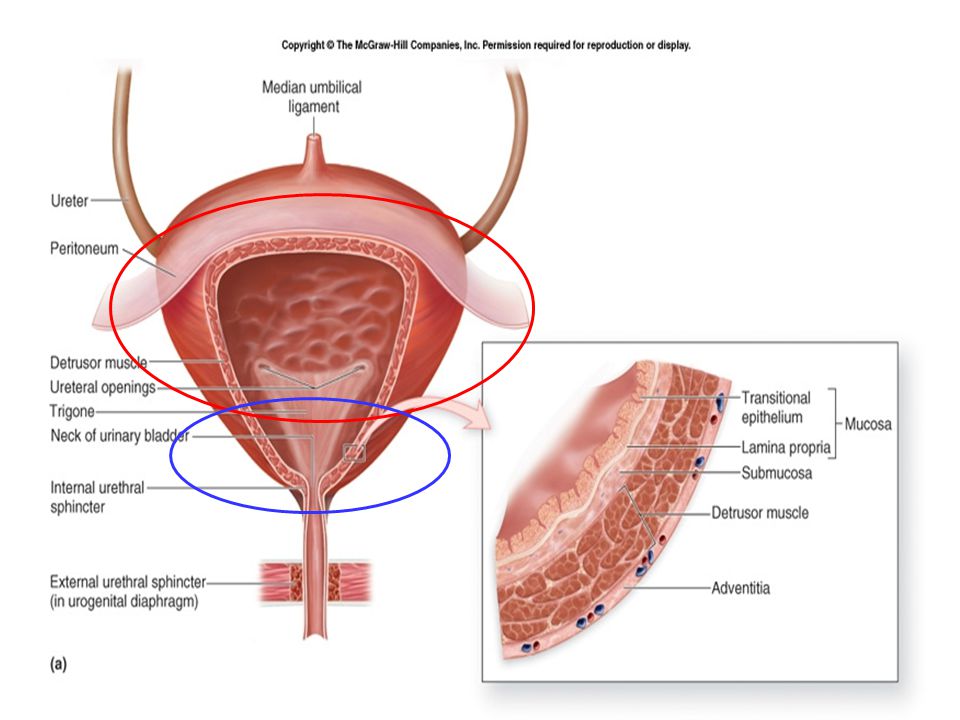
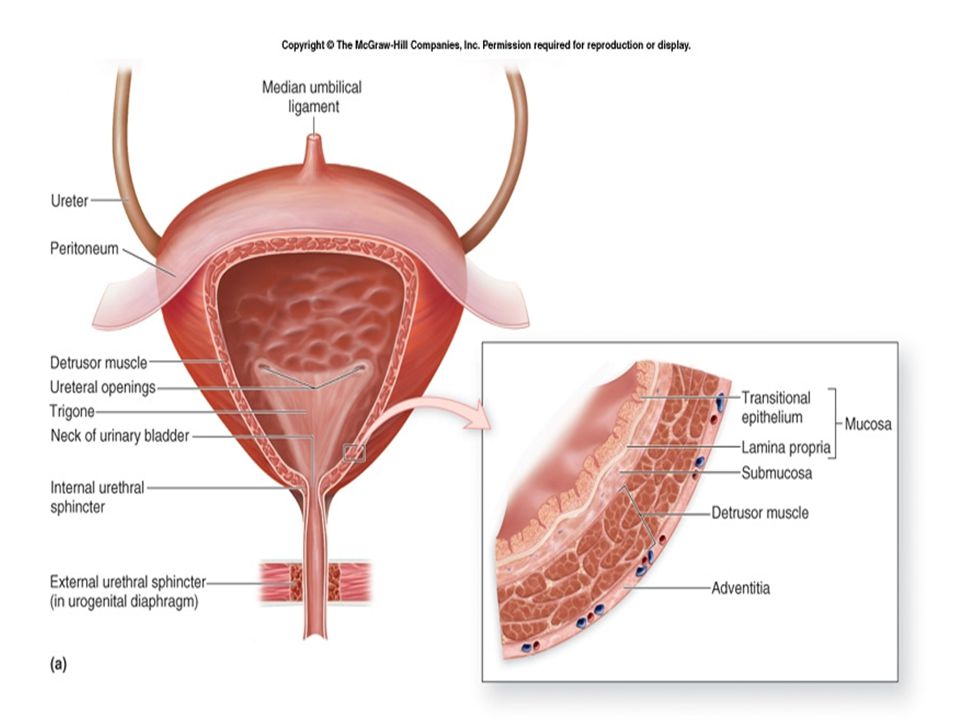
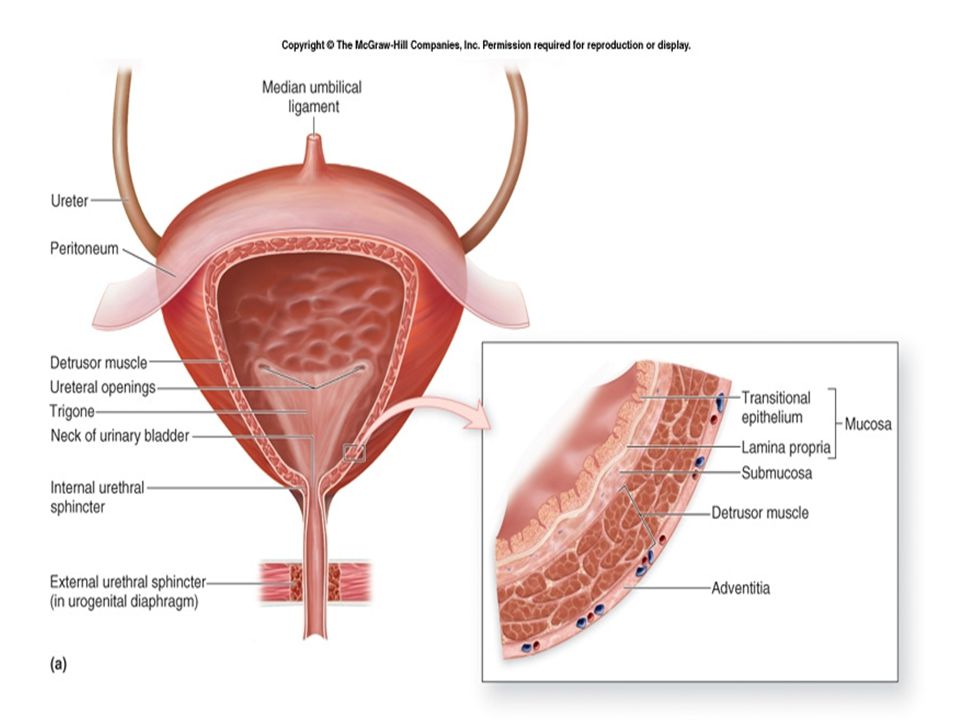
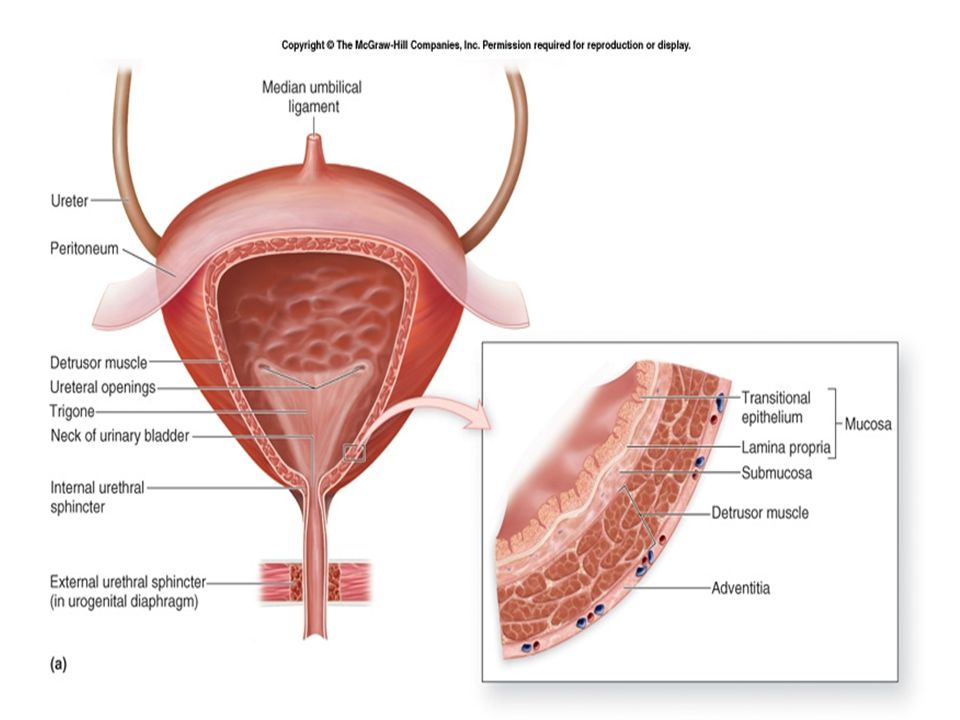
A) Body of Bladder: Inner cavity: The posterior wall of the body, immediately above the bladder neck , shows a triangular zone, called trigone The apex of trigone joins the bladder neck, and its base marks the opening of the two ureters Wall : 3 layers Mucosa and submucosa Muscle layer (detrusor muscle) Adventia
 Body of Bladder: Inner cavity: The posterior wall of the body, immediately above the bladder neck , shows a triangular zone, called trigone. The apex of trigone joins the bladder neck, and its base marks the opening of the two ureters. Wall : 3 layers. Mucosa and submucosa. Muscle layer (detrusor muscle) Adventia.")
11
Physiological anatomy of urinary bladder
Its base is bounded by the opening of the 2 ureters, while its apex forms the bladder neck. The two ureters course obliquely through the detrusor muscle for 1-2 cm underneath the mucosa before emptying into the bladder. When the bladder is filled by urine, it compresses the 2 ureters (intravesical portion of the ureters) preventing reflux of urine into the ureter. The urine flow from the kidney by peristaltic movement of the ureter one every 6 seconds.
 preventing reflux of urine into the ureter. The urine flow from the kidney by peristaltic movement of the ureter one every 6 seconds.")
13
Physiological anatomy of urinary bladder
1) Submucosa: The wall of UB is lined by a transitional epithelium that is continuous with that in the ureters. When the bladder is empty, the mucosa has numerous folds called rugae. As the bladder fills with urine these rugae flatten out and distend with little change in intravesical pressure This results in high compliance of the bladder, so the volume of the bladder can ↑ from 10 ml to 400 ml with a pressure change of only 10 cm H2O
 Submucosa: The wall of UB is lined by a transitional epithelium that is continuous with that in the ureters. When the bladder is empty, the mucosa has numerous folds called rugae. As the bladder fills with urine these rugae flatten out and distend with little change in intravesical pressure. This results in high compliance of the bladder, so the volume of the bladder can ↑ from 10 ml to 400 ml with a pressure change of only 10 cm H2O.")
14
Physiological anatomy of urinary bladder
2) Submucosa: It supports the mucous membrane. It is composed of connective tissue with elastic fibers. 3) Muscle layer (Detrusor muscle): It is composed of smooth muscle. The smooth muscle fibers are interwoven in all directions and collectively these are called the detrusor muscle. It consist of a mixture of spiral and longitudinal muscle fibers It can increase the pressure in the bladder to 40 – 60 mmHg.
 Submucosa: It supports the mucous membrane. It is composed of connective tissue with elastic fibers. 3) Muscle layer (Detrusor muscle): It is composed of smooth muscle. The smooth muscle fibers are interwoven in all directions and collectively these are called the detrusor muscle. It consist of a mixture of spiral and longitudinal muscle fibers. It can increase the pressure in the bladder to 40 – 60 mmHg.")
15
Physiological anatomy of urinary bladder

16
Physiological anatomy of urinary bladder
Bladder Neck : It is a funnel shaped extension of the body toward the urogenital triangle, to join the anterior urethra (external urethra). The lower 2-3 cm of the bladder neck is called the posterior or internal urethra. The ms fibers in the bladder neck are arranged in 3 layers: inner longitudinal, middle circular, and outer longitudinal. The inherent tone of the bladder neck ms, specially the middle layer, prevents emptying of the bladder until the appropriate time for micturition.
. The lower 2-3 cm of the bladder neck is called the posterior or internal urethra. The ms fibers in the bladder neck are arranged in 3 layers: inner longitudinal, middle circular, and outer longitudinal. The inherent tone of the bladder neck ms, specially the middle layer, prevents emptying of the bladder until the appropriate time for micturition.")
18
Physiological anatomy of urinary bladder
Bladder Neck : The urethra passes through the urogenital diaphragm where it is surrounded by the external urethral sphincter (under voluntary control) used to prevent or interrupt urination, specially in males, it is poorly developed in females.
 used to prevent or interrupt urination, specially in males, it is poorly developed in females.")
20
Innervations of UB

21
Autonomic Innervations of the bladder Parasympathetic Supply
Nerve Pelvic nerve Hypogastric Nerve Efferents: Origin: Supply: Functions -LHCs of the S 2,3, and 4. -Body and neck of the bladder. a) Contraction of bladder wall. b) Relaxation of the bladder neck → stimulation of the detrusor ms of the body causes longitudinal layers to open the bladder neck. - L1,2, and 3. - Bladder neck. a) Contraction of bladder neck, specially the middle layer→ facilitate the storage of urine. b) Relaxation of the bladder wall by inhibiting the parasympathetic ganglia. Afferents: a) Carry input from stretch receptors in the bladder neck.. b) Detect bladder fullness. c) Carry pain and temperature sensation. Transmit pain sensation Detect bladder fullness
 Contraction of bladder wall. b) Relaxation of the bladder neck → stimulation of the detrusor ms of the body causes longitudinal layers to open the bladder neck. - L1,2, and 3. - Bladder neck. a) Contraction of bladder neck, specially the middle layer→ facilitate the storage of urine. b) Relaxation of the bladder wall by inhibiting the parasympathetic ganglia. Afferents: a) Carry input from stretch receptors in the bladder neck.. b) Detect bladder fullness. c) Carry pain and temperature sensation. Transmit pain sensation. Detect bladder fullness.")
22
Autonomic Innervations of the bladder

23
Somatic Innervations of the bladder
The Pudendal nerves (AHCs of S 2,3,and 4) Its efferent fibers arise as the parasympathetic nerves from the 2nd, 3rd and 4th sacral segments of the spinal cord but from the AHCs. They supply and control the activity of the external urethral sphincter
 Its efferent fibers arise as the parasympathetic nerves from the 2nd, 3rd and 4th sacral segments of the spinal cord but from the AHCs. They supply and control the activity of the external urethral sphincter.")
24
Autonomic and Somatic Innervations of the bladder

25
Functions of the Urinary Bladder
In healthy individuals, the bladder has two discrete phases of activity: The storage phase, when urine is stored in the bladder; and The voiding phase, when urine is released through the urethra.

26
Storage Phase During storage, bladder pressure stays low, because of the bladder's highly compliant nature. This property is helped by the presence of the transitional epithelium. This function is studied by a curve or plot between bladder (intravesical) pressure against the volume of fluid in the bladder (called a cystometrogram)
 pressure against the volume of fluid in the bladder (called a cystometrogram)")
27
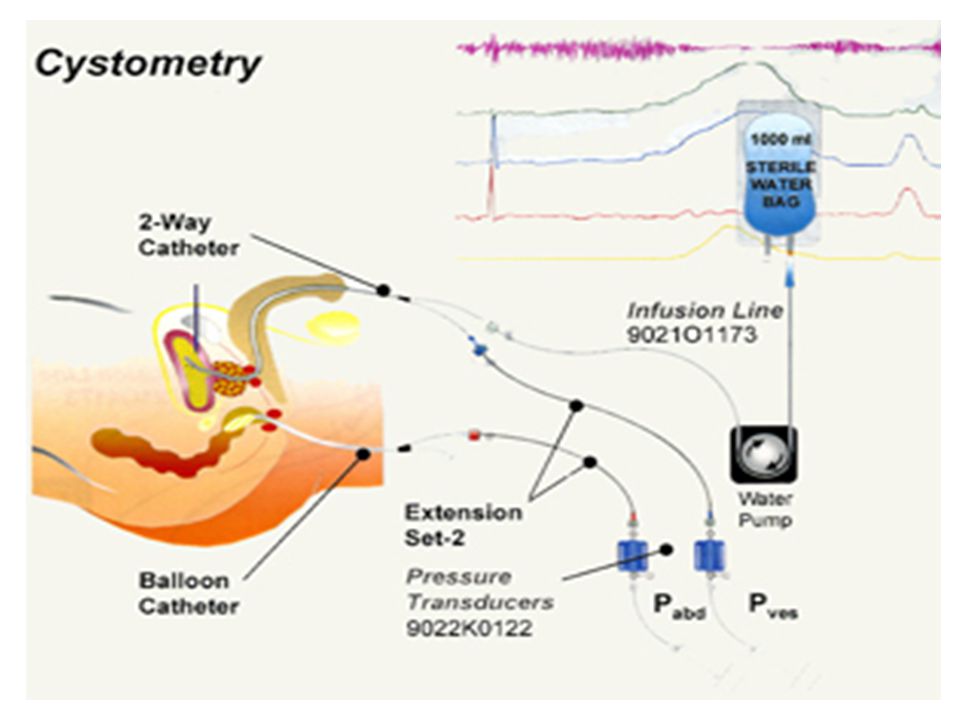
Cystometrogram Def. It is a curve which studies the relationship between intravesical pressure (IVP) and volume. Method: It is done by inserting a catheter into the bladder to fill and empty the bladder by water, and through special transducer, the intravesical pressure is recorded. First, the bladder is empted from urine and the pressure is recorded, then the bladder is filled with 50 ml water and the pressure is recorded for every ↑ in the volume.

29
Intravesical Pressure Intravesical Volume (ml)
Cystometrogram II Intravesical Pressure (cm H2O2) Ib Ia Intravesical Volume (ml)
 Ib. Ia Intravesical Volume (ml)")
30
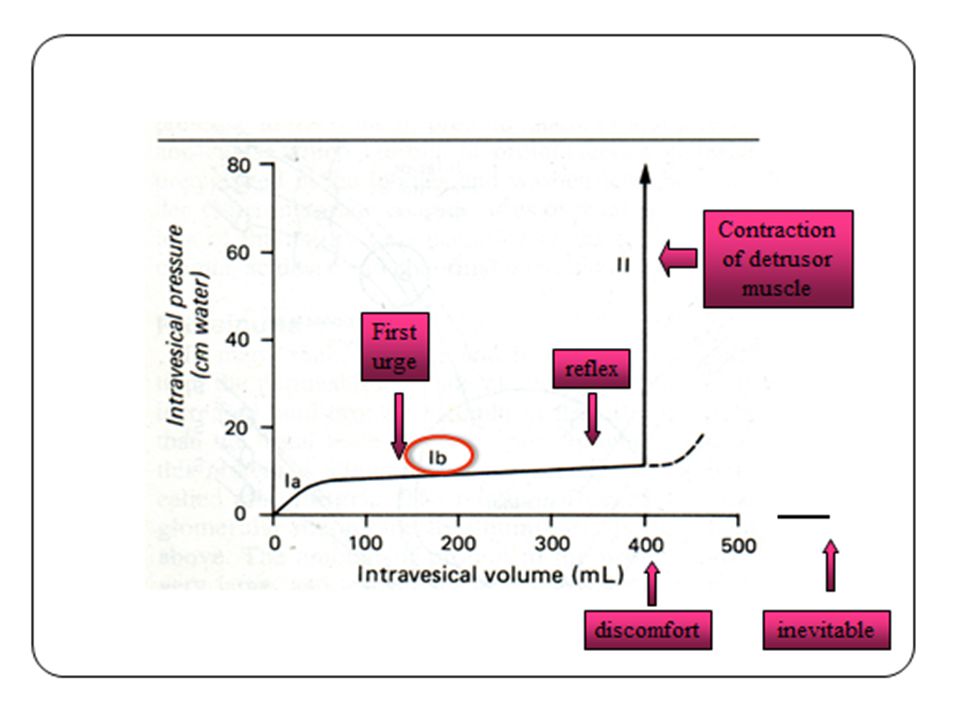
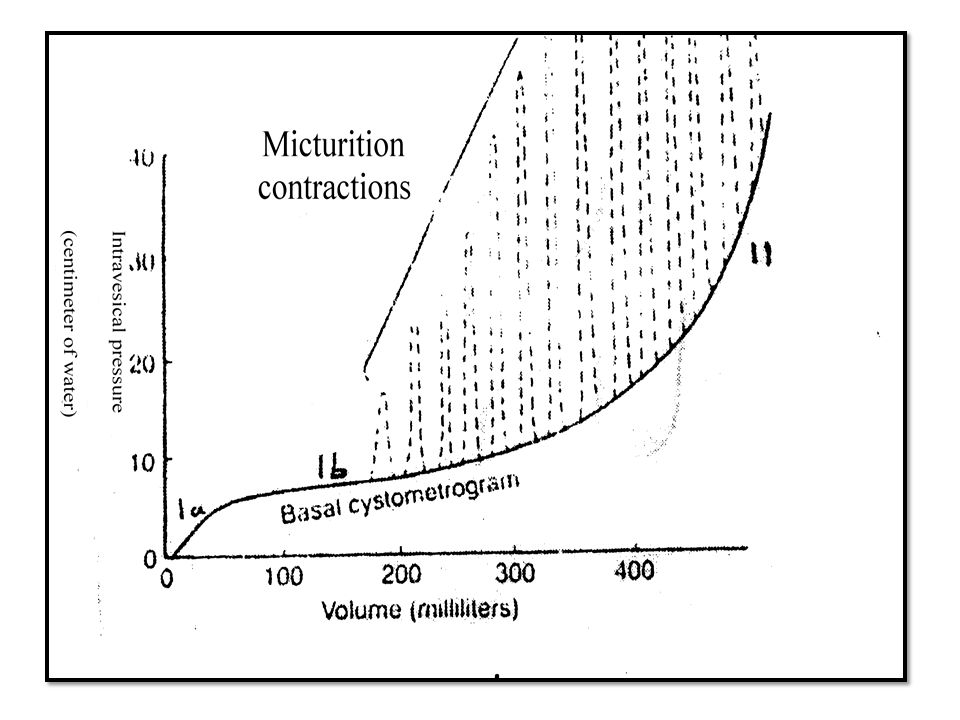
Cystometrogram Ia Ib II Initial slight rise Long flat segment
Sharp rapid rise Produced by the 1st increment of volume by about 50 ml. Produced by further increase in volume up to 400 ml. Produced by further increase in volume above 400 ml.

33
Cystometrogram Segment Ib is a manifestation of the law of Laplace, which states that the pressure in a spherical viscus is equal to twice the wall tension divided by the radius. In the case of the bladder, the tension increases as the organ fills, but so does the radius. Therefore, the pressure increase is slight until the organ is relatively full.

34
Micturition

35
Micturition Def: It is the periodic evacuation of urinary bladder through urethra Mechanism: Micturition is fundamentally a spinobulbospinal reflex facilitated and inhibited by higher brain centers and, like defecation, subject to voluntary facilitation and inhibition.

36
Micturition Reflexes Center: sacral segments 2, 3 & 4.
Receptors: stretch (receptor) in the wall of bladder. Afferent & efferent: pelvic nerve. Response: Contraction of detrusor muscle (body). Relaxation of internal sphincter of urethra. Relaxation of external urethral sphincter via the pudendal nerve which is somatic nerve originating from AHC of sacral segment 2, 3, & 4.
 in the wall of bladder. Afferent & efferent: pelvic nerve. Response: Contraction of detrusor muscle (body). Relaxation of internal sphincter of urethra. Relaxation of external urethral sphincter via the pudendal nerve which is somatic nerve originating from AHC of sacral segment 2, 3, & 4.")
37
↑ IVP Stretch receptors Center S2,3,4, Contraction of wall Afferents
Pelvic Nerve Relaxation of int. sphincter Efferent Pelvic Nerve Relaxation of ext. sphincter

38
Voluntary Control of Micturition

39
Higher Centers Control Micturition
1) Cerebral cortex: Motor cortex exerts a voluntary control of micturition either stimulation or inhibition. 2) Hypothalamus: There is facilitatory area in the hypothalamus. 3) Midbrain: Inhibition. 4) Pons: facilitation
 Cerebral cortex: Motor cortex exerts a voluntary control of micturition either stimulation or inhibition. 2) Hypothalamus: There is facilitatory area in the hypothalamus. 3) Midbrain: Inhibition. 4) Pons: facilitation.")
40
Higher Centers Control Micturition
Keeping the micturition reflex partially inhibited all the time except when there is a desire for micturition. Prevent the micturition even when the reflex is initiated until appropriate time allows.

41
Voluntary Initiation of Micturition
Relaxation of perineal ms causing traction on the bladder Contraction of anterior abdominal wall and diaphragm to increase intra-abdominal pressure compressing bladder. Relaxation of external urethral sphincter. Flow of urine in urethra intensification of the reflex. If the condition unfavourable, the higher center will delay micturition until convenient time by: 1) Inhibition of sacral segment of micturition. 2) Stimulation of external urethral sphincter. 3) Contractions of perineal muscle decrease intravesical pressure.
 Inhibition of sacral segment of micturition. 2) Stimulation of external urethral sphincter. 3) Contractions of perineal muscle decrease intravesical pressure.")
42
If the bladder fluid content exceeds 700 ml, urine starts to dribble in spite of the voluntary control

43
Effects of various lesions on micturition
1) Tabetic bladder: Due to interruption of the afferent fibers sensory atonic bladder over flow incontinence. Occurs in tabes dorsalis. 2- Denervated or decentralized bladder: There is interruption of the afferent and efferent fibers as in cauda equine lesion shrunken and hypertrophied bladder, it can expel dripples ml at a time.
 Tabetic bladder: Due to interruption of the afferent fibers sensory atonic bladder over flow incontinence. Occurs in tabes dorsalis. 2- Denervated or decentralized bladder: There is interruption of the afferent and efferent fibers as in cauda equine lesion shrunken and hypertrophied bladder, it can expel dripples ml at a time.")
44
Effects of various lesions on micturition
3- Injury to superior frontal gyrus: Causes reduction in the desire to micturition, but once started it's difficult to interrupt. 4- Transection of spinal cord: Complete transection of spinal cord affects micturition as such: During the spinal shock over flow incontinence. After recovery automatic bladder the U.B fill with urine, till certain volume and pressure capable of micturition reflex to be carried out in the spinal sacral centers without supraspinal influence and with conscious feeling of micturition as infants and children below 2 years.

46
THANKS

Similar presentations