Download presentation
Presentation is loading. Please wait.

1
APPROACH TO POLY-ARTHRITIS
DR CB NEL

2
Joints cartilage/synovium
Arthritis Inflammatory Rheumatoid arthritis Seronegative spondiloarthropaties Gout Septic Degenerative Osteoartritis Lower back pain

3
Diagnostic approach Inflammatory vs. Noninflamatory Acute vs. Chronic
Temporal pattern of joint involvement Distribution of joint involvement Age of patient Sex of patient Systemic involvement

4
Inflammatory vs Mechanical
Morning stiffness >1 hr Fatigue Profound Activity Improves symptoms Rest Worsens symptoms Systemic involvement Yes Swelling, warmth, erythema, tenderness, loss of function Morning stiffness <30 min Fatigue Minimal Activity Worsens symptoms Rest Improves symptoms Systemic involvement No

5
Acute vs. Chronic

6
Acute Polyarthritis Infection Other inflammatory Gonococcal
Meningococcal Acute rheumatic fever Bacterial endocarditis Viral(esp.. rubella, hepatitis B, parvovirus, Epstein-Barr, HIV) Other inflammatory Rheumatoid arthritis Juvenile chronic arthritis SLE Reactive arthritis Psoriatic arthritis Polyarticular gout Sarcoid arthritis Serum sickness
 Other inflammatory. Rheumatoid arthritis. Juvenile chronic arthritis. SLE. Reactive arthritis. Psoriatic arthritis. Polyarticular gout. Sarcoid arthritis. Serum sickness.")
7
Chronic Polyarthritis (>6 weeks)
Inflammatory Rheumatoid arthritis Polyarticular Juvenile chronic arthritis SLE Progressive systemic sclerosis Polymyositis Reiter’s syndrome Psoriatic arthritis Enteropathic arthritis Polyarticular gout Pseudogout (CPPD) Sarcoid arthritis Vasculitis Polymialgia rheumatica
 Sarcoid arthritis. Vasculitis. Polymialgia rheumatica.")
8
Chronic Polyarthritis (>6 weeks)
Noninflammatory Osteoarthritis Pseudogout (CPPD) Polyarticular gout Paget’s disease Fibromyalgia Benign hypermobility syndrome Hemochromatosis
 Polyarticular gout. Paget’s disease. Fibromyalgia. Benign hypermobility syndrome. Hemochromatosis.")
9
Temporal patterns of joint involvement
Intermittent Rheumatoid arthritis Psoriatic arthritis Reactive Arthritis Palandromic Gout Migratory Rheumatic fever Gonococcal arthritis Additive Nonspecific Rheumatoid arthritis SLE

10
Distribution of joint involvement
Rheumatoid arthritis Commonly involved Wrist, MCP, PIP, elbow, glenohumeral, cervical spine, hip, knee, ankle, tarsal, MTP Commonly spared DIP, thoracolumbar spine

11
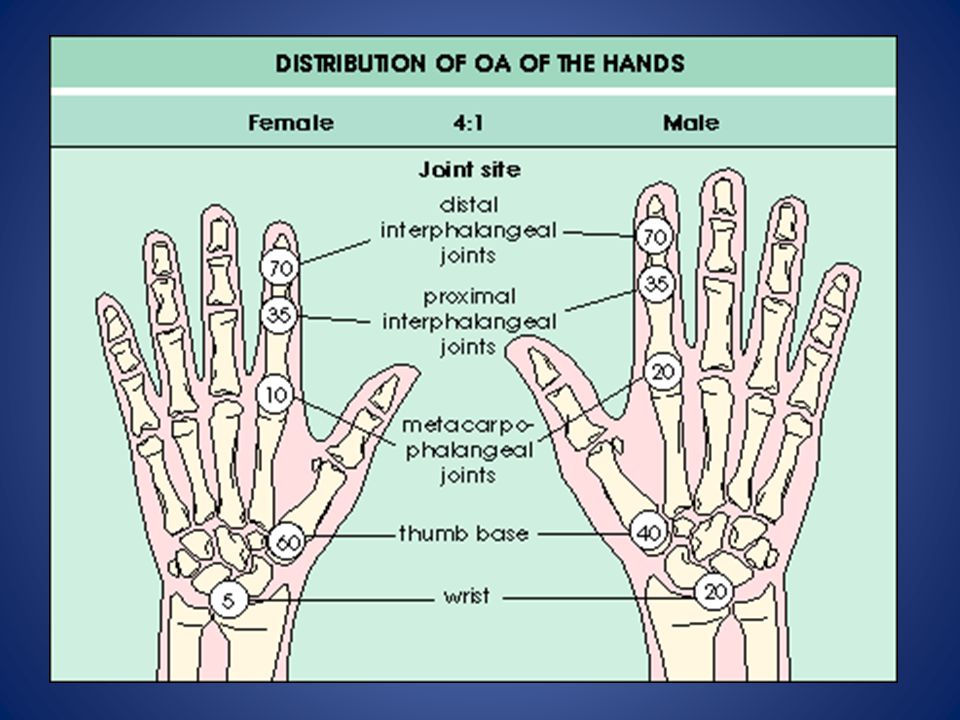
Distribution of joint involvement
Osteoarthritis Commonly involved First CMC, DIP, PIP, cervical spine, thoracolumbar spine, hip, knee, first MTP, toe IP Commonly spared MCP, wrist, elbow, glenohumeral, ankle, tarsal

12
Distribution of joint involvement
Reactive arthrits Commonly involved Knee, ankle, tarsal, MTP, toe IP, elbow, axial Gonococcal arthritis Knee, wrist, ankle, hand IP Commonly spared Axial

14
Hand Involvement

15
RHEUMATOID ARTHRITIS

16
CLINICAL FEATURES Prolonged morning stiffness
Synovitis of small joints of hands, wrists and feet Other synovial structures (tenosynovitis, bursae) also common Typical hand features: Symmetrical swelling of the MCP and PIP joints Tenderness of involved joints Swan neck deformities Boutonniére deformities Z-deformity of the thumb Dorsal subluxation of the ulna styloid Triggering of the fingers
 also common. Typical hand features: Symmetrical swelling of the MCP and PIP joints. Tenderness of involved joints. Swan neck deformities. Boutonniére deformities. Z-deformity of the thumb. Dorsal subluxation of the ulna styloid. Triggering of the fingers.")
17
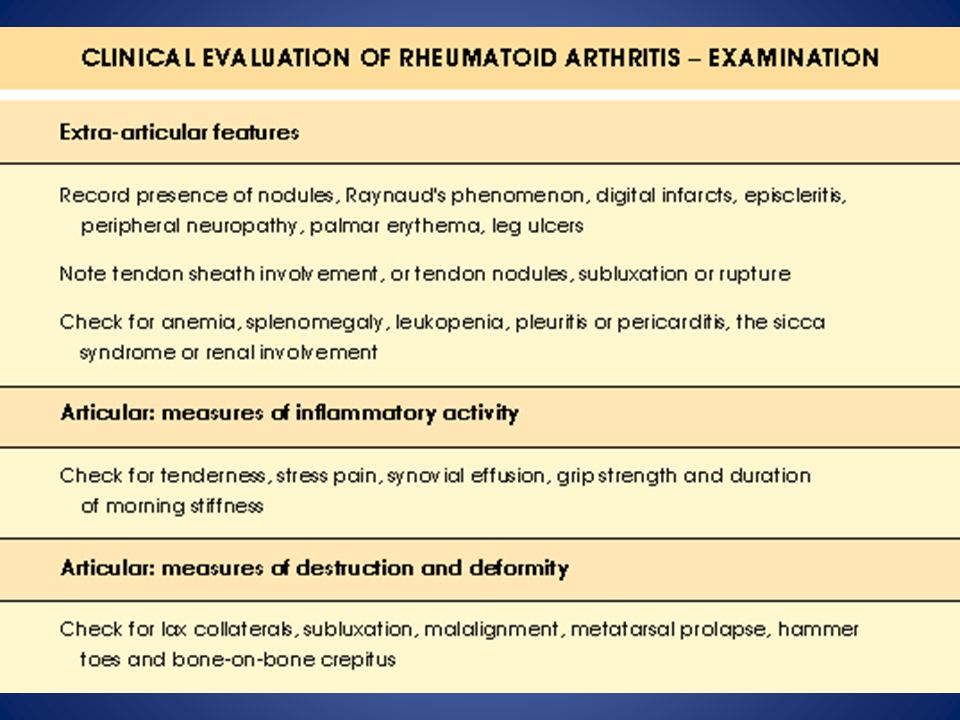
EXTRA-ARTICULAR MANIFESTATIONS
Systemic Fever, fatigue, weight loss, increased infection risk MSK Muscle-wasting, tenosynovitis, bursitis, osteoporosis Haematological Reactive thrombocytosis, microcytic anaemia, anaemia of chronic disease(normochromic, normocytic) Lymphatic Splenomegaly, Felty’s syndrome(RA, splenomegaly, neutropenia)
 Lymphatic. Splenomegaly, Felty’s syndrome(RA, splenomegaly, neutropenia)")
18
EXTRA-ARTICULAR MANIFESTATIONS
Ocular Episcleritis, scleritis, scleromalacia, keratoconjunctivitis sicca Vasculitis Nailfold infarcts, skin ulcers, pyoderma gangrenosum, mononeuritis multiplex, visceral arteritis Cardiac Pericarditis, myocarditis

19
EXTRA-ARTICULAR MANIFESTATIONS
Neurological Atlantoaxial subluxation, carpal tunnel syndrome, peripheral neuropathies, mononeuritis multiplex Pulmonary Nodules, pleural effusions, pulmonary fibrosis, bronchiolitis, Caplan’s syndrome(RA plus pneumoconiosis), bronchiectasis Nodules Subcutaneous, lungs, pericardium Amyloidosis
, bronchiectasis. Nodules. Subcutaneous, lungs, pericardium. Amyloidosis.")
21
Early RA

22
RA HANDS

23
Extensor tenosinovitis

24
Olecranon bursitis and subcutaneous nodules

25
Baker’s popliteal sist

26
RA FEET

27
RA feet

28
SPECIAL INVESTIGATIONS
CRP and ESR usually elevated Rheumatoid factor positive in 70% Anti-CCP positive in a sub-population X-rays: periarticular osteopenia and marginal erosion (x-ray changes takes months to develop)
")
29
CLASSIFICATION CRITERIA OF RA
NEW CRITERIA HAS BEEN PUBLISHED IN 2010

30
TREATMENT A multidisciplinary team approach is followed

31
PATIENT EDUCATION The nature of the disease as well as its chronic course Disease is characterised by fluctuations It takes a considerable time before the therapy starts to show results Ignorance and especially the fear of becoming an invalid must be adressed

32
PHYSIOTHERAPY Exercise programme Maintain muscle strength
Maintain joint mobility as well as prevent contractures

33
OCCUPATIONAL THERAPY Patient guidance with regard to work activities and joint-saving techniques, as well as the positions of joints during sleep Rest and night splints are also important Other aids for daily activies are also provided

34
PHARMACOLOGICAL THERAPY
Analgesics DMARD (changes the course of the disease) Corticosteroids Immunotherapy Other
 Corticosteroids. Immunotherapy. Other.")
35
ANALGESICS Oral analgesics (Paracetamol, tramadol) NSAID’s Coxibs
gastro-intestinal and renal side-effects high-risk cases Misoprostol (Cytotec) Proton pump inhibiters H2 antagonists Coxibs
 Proton pump inhibiters. H2 antagonists. Coxibs.")
36
CORTICOSTEROIDS Low dose oral (chronic as a “DMARD”)
Intra-articular steroids Pulse high dose treatment Flares Treatment of complications

37
DMARD’S Chloroquine Sulphasalazine Methotrexate
Other immunosuppressants Combination therapy Biologic agents when patients fail DMARD therapy - TNF alpha inhibiters - B cell inhibiters - Interleukin 6 inhibiters

38
OTHER Orthopaedic aids Orthopaedic surgical treatment
Rx extra-articular complications Supportive therapy education anxiety depression

39
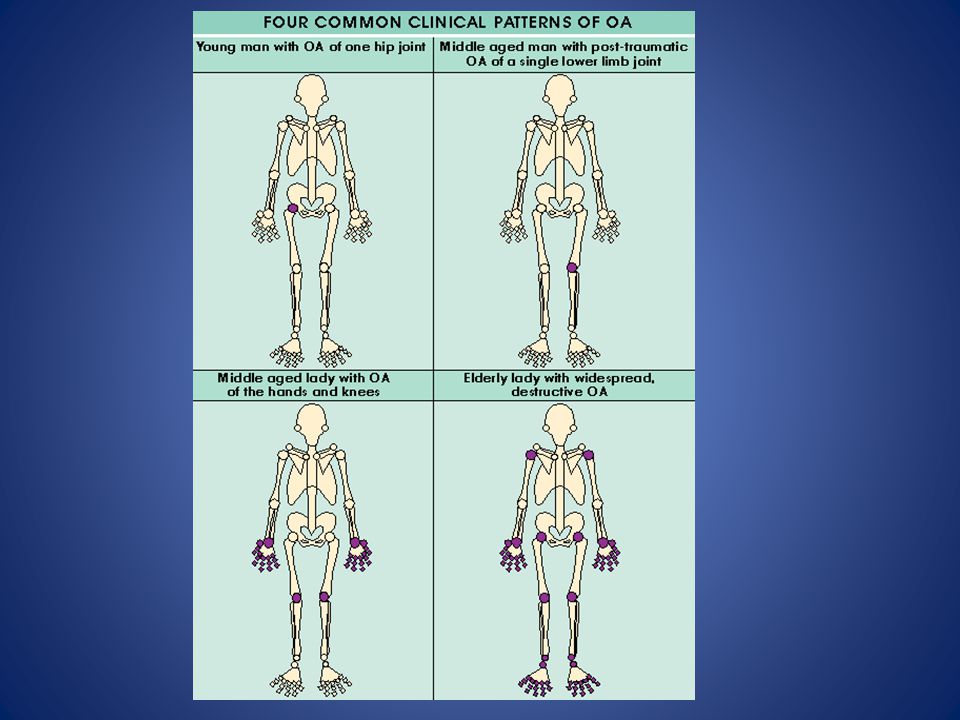
OSTEOARTHRITIS

40
OSTEOARTHRITIS Most common arthritis Strongly associated with aging
Characterised by focal loss of articular cartilage with new bone proliferation and remodelling of the joint contour Inflammation is NOT a prominent feature Risk factors Family history Caucasians Women Trauma Adverse loading(obesity,sport,profession)
")
41
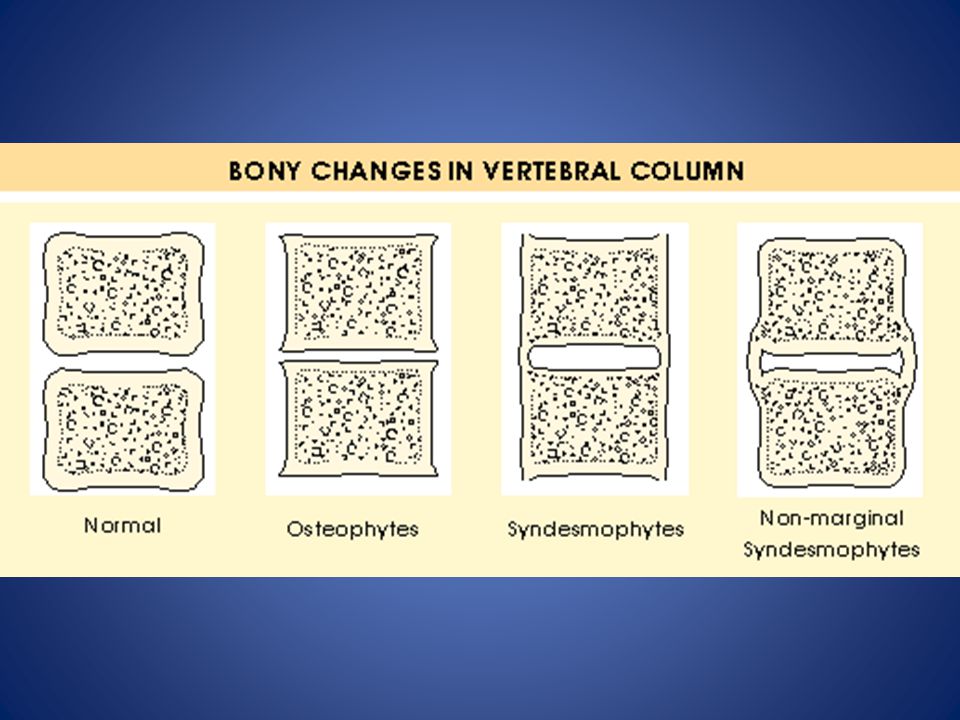
PATHOLOGICAL CHANGES IN OA

42
SYMPTOMS Artralgia and functional restriction
Insidious onset of symptoms Pain worsened by movement and relieved by rest Brief (<15min.) morning stiffness and brief “gelling” after rest
 morning stiffness and brief gelling after rest.")
43
PHYSICAL SIGNS Bony swelling and deformity around joint margins
Joint-line tenderness Decreased range of movement Palpable coarse crepitations Muscle wasting Antalgic gait common with involvement of lower limbs

45
OA HANDS

46
SPECIAL INVESTIGATIONS
NO impact on inflammatory markers(CRP, ESR) X-ray changes Joint space narrowing Subchondral sclerosis Osteophytes Bone cysts Correlation between x-ray changes and the level of pain and disability is variable
 X-ray changes. Joint space narrowing. Subchondral sclerosis. Osteophytes. Bone cysts. Correlation between x-ray changes and the level of pain and disability is variable.")
47
TREATMENT OF OA Exercise Lose weight Heat or cold Analgesia
Paracetamol Topical NSAID Oral NSAID Opioids Intra-articular steroids can give temporary relief Surgery For uncontrolled pain Progressive functional impairment

48
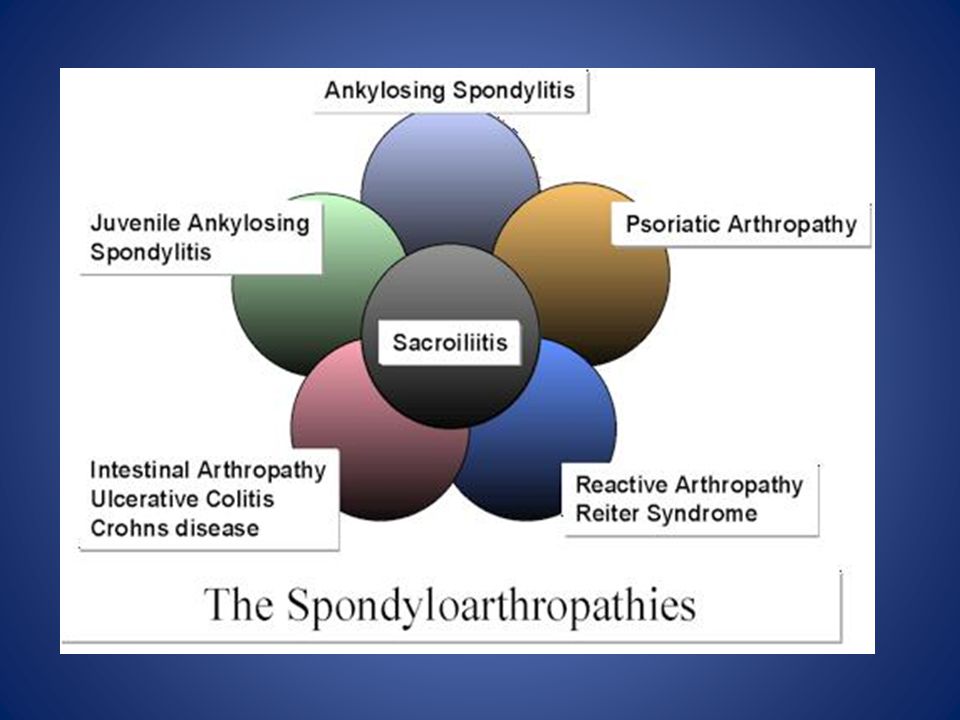
Seronegative spondilo-arthropathies

50
CLINICAL FEATURES OF THE SERONEGATIVE SPONDARTHRITIS
Asymmetrical inflammatory oligoarthritis (lower>upper limb) Sacroiliitis and inflammatory spondylitis Inflammatory enthesitis Tendency for familial aggregation NO association with positve Rheumatoid factor Absence of nodules and other extra-articular features of RA Strong association with HLA-B27
 Sacroiliitis and inflammatory spondylitis. Inflammatory enthesitis. Tendency for familial aggregation. NO association with positve Rheumatoid factor. Absence of nodules and other extra-articular features of RA. Strong association with HLA-B27.")
51
ENTHESITIS: Inflammation of the attachment of tendons or ligaments to bone (hallmark feature of the seronegative spondarthritis)
")
52
LOWER BACKPAIN Inflammatory Mechanical Age < 40 years Any age
Progression Slowly/Chronic Acute Duration of symptoms > 3 months < 4 weeks Morning stiffness > 60 min. < 3o min. Night pain(vertebral) Common Absent Exercise Improve Worsens SI-joint tenderness Vertebral mobility ↓ all directions ↓ flection Chest expansion Decreased Normal
 Common. Absent. Exercise. Improve. Worsens. SI-joint tenderness. Vertebral mobility. ↓ all directions. ↓ flection. Chest expansion. Decreased. Normal.")
54
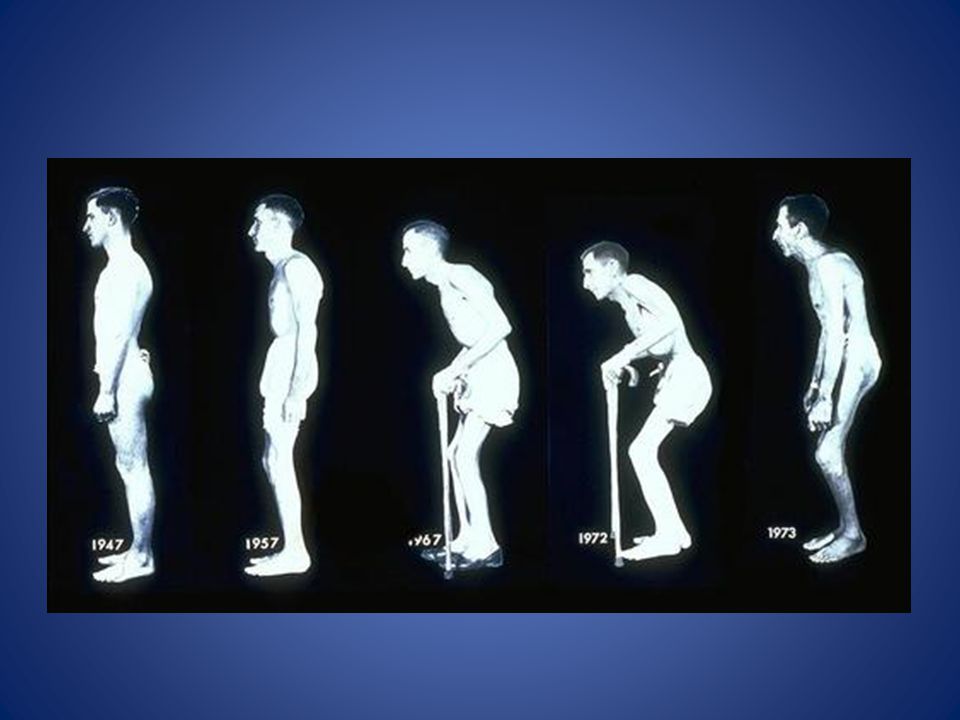
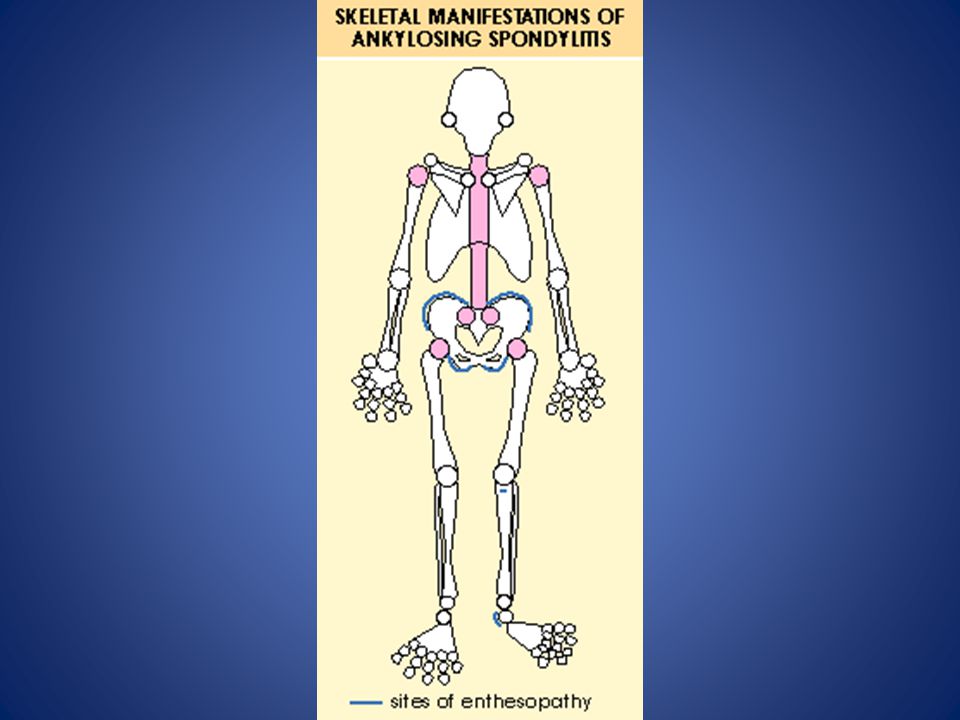
ANKYLOSING SPONDYLITIS
Predilection for the sacroiliac joints and spine Male : female ratio of 3:1 Progressive stiffening and fusion of axial skeleton

55
SPINAL FEATURES Insidious onset over months to years
Restriction of lumbar movements Possible involvement of the entire spine as disease progress Progressive spinal fusion Loss of lumbar lordosis Marked thoracic kyphosis Reduced chest expansion

58
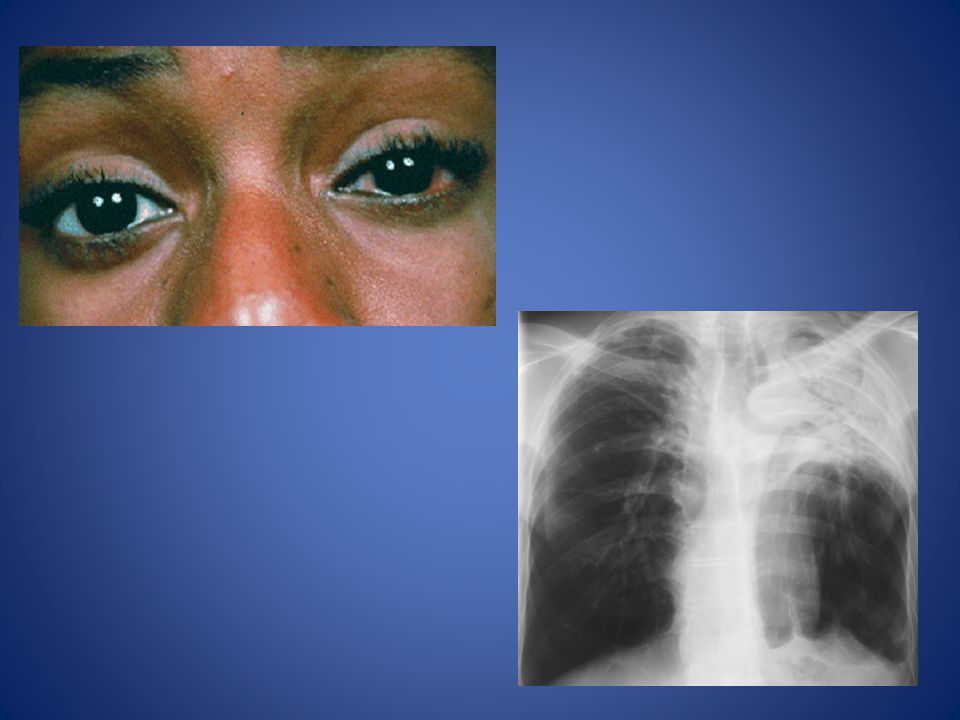
EXTRASPINAL FEATURES Plantar fasciitis and Achilles tendinitis
Asymmetrical peripheral arthritis: shoulders, hips, knees and ankles Anterior uveitis Aortic incompetence Cardiac conduction defects UPPER lobe pulmonary fibrosis Osteoporosis

59
PLANTAR FASCIITIS

60
ACHILLES TENDON ENTHESITIS

62
TREATMENT Physiotherapy Regular NSAID’s
Sulfasalazine for peripheral arthritis Tumour necrosis factor(TNF)-Alpha inhibiters
-Alpha inhibiters.")
63
REACTIVE ARTHRITIS Classically young men
Acute onset inflammatory oligoarthritis 1-3 weeks afer an infection affecting the small and large joints of the lower limbs Infective “trigger” Bacterial dysentery (due to Salmonella, Campylobacter, Shigella, Yersinia) Non-spes. urethritis (due to Clamydia) First attack usually self-limiting with spontaneous remission within 4-6 months Treatment: Mostly symptomatic with NSAID’S DMARD’s in worse cases
 Non-spes. urethritis (due to Clamydia) First attack usually self-limiting with spontaneous remission within 4-6 months. Treatment: Mostly symptomatic with NSAID’S. DMARD’s in worse cases.")
64
PSORIATIC ARTHROPATHY
Five major articular presentations: Asymmetrical inflammatory oligoarthritis Symmetrical polyarthritis (Strongly resemble RA) Predominantly distal interphalangeal joint arthritis Psoriatic spondylitis (strongly resemle Ankylosing spondylitis) Arthritis mutilans Skin lesions Nail changes: pitting, onycholysis, subungual hyperkeratosis Treatment similar to Ankylosing spondulitis (methotrexate will also help for peripheral arthritis)
 Predominantly distal interphalangeal joint arthritis. Psoriatic spondylitis (strongly resemle Ankylosing spondylitis) Arthritis mutilans. Skin lesions. Nail changes: pitting, onycholysis, subungual hyperkeratosis. Treatment similar to Ankylosing spondulitis. (methotrexate will also help for peripheral arthritis)")
65
Symmetric psoriatic polyarthritis resembling RA

66
Distal interphalangeal joint involvement

67
Nail pitting Skin Enthesophathy Dactilitis
Psoriatic Arthritis Nail pitting Skin Enthesophathy Dactilitis

68
ARTHRITIS ASSOCIATED WITH INFLAMMATORY BOWEL DISEASE
Two patterns of articular involvement: Acute oligoarthritis with a predilection for the lower limb joints. Sacroiliitis and ankylosing spondylitis

69
QUESTIONS?

Similar presentations

 25 th Nov 2013.>")







 M:F 1:3 Age range:>")








 is the name for a family of inflammatory rheumatic diseases that cause.>")
