Download presentation
Presentation is loading. Please wait.

1
Pretest questions The recommended ages for routine developmental screening tests are: 12m, 24m, 36m *9m, 18m, 24/30m 6m, 18m, 24/30m 6m, 12m, 24m The prevalence for developmental disabilities in children is approximately: 1% 5% *15% 30%

2
Developmental Surveillance and Screening Craig D. Boreman, MD, FAAP 21 February 2015

3
Disclosures I did not, do not, and likely will not have any financial relationships with proprietary entities that produce goods or services I am the medical director for the new Dayton Autism Center and have a vested interest in seeing children receive the best health care

4
Objectives Understand the reasons for developmental/behavioral monitoring Learn the importance of Surveillance vs Screening Experience specific tools (examples) for screening
 for screening")
5
Did You Know? ● Prevalence of developmental disabilities 1 in 7 children (~14%) ● Most developmental disabilities are ● Learning disabilities – 7.6% ● ADHD – 6.7% ● Intellectual disability – 0.7% ● Autism – 0.47% Blumberg SJ. Trends in the Prevalence of DD in US Children, 1997-2008. Presented at National Conference on Health Statistics, August 2012 Over the 12 years, increase of ------------17% ------------33% ------------290%
 ● Most developmental disabilities are ● Learning disabilities – 7.6% ● ADHD – 6.7% ● Intellectual disability – 0.7% ● Autism – 0.47% Blumberg SJ. Trends in the Prevalence of DD in US Children, Presented at National Conference on Health Statistics, August 2012 Over the 12 years, increase of % % %.")
6
A little more on autism – 1975, 1 in 5000: 0.2/1000 – 1985, 1 in 2500: 0.4/1000 – 1995, 1 in 500: 2/1000 – 2001, 1 in 250: 4/1000 – 2006, 1 in 110: 9/1000 (CDC) – 2008, 1 in 88: 11/1000 (CDC) – 2013, 1 in 50: 20/1000 (CDC)* * Health Resources and Services Administration and Centers for Disease Control report – Mar13
 – 2008, 1 in 88: 11/1000 (CDC) – 2013, 1 in 50: 20/1000 (CDC)* * Health Resources and Services Administration and Centers for Disease Control report – Mar13")
7
Autism There has been a 600% increase in prevalence in the past 20 years One in 50

8
What’s causing the rise? Many factors Diagnostic change Substitution (X → Y) Accretion (X → X + Y) Broadening (x → X) Advanced parental age Social influence and increased awareness Better education/Increased information dissemination Spatial clustering Advocacy interest groups National/International coverage Other factors? 2009 Amer J Epidemiology 2009 Oct Int J Epidemiol 2010 Mar Amer J Sociology
 Accretion (X → X + Y) Broadening (x → X) Advanced parental age Social influence and increased awareness Better education/Increased information dissemination Spatial clustering Advocacy interest groups National/International coverage Other factors Amer J Epidemiology 2009 Oct Int J Epidemiol 2010 Mar Amer J Sociology.")
9
WHY SCREEN??

10
Benefits of Monitoring Screening works Results in access to services Cost effective Improves patient/family satisfaction Because we are told to!

11
Early Intervention Efficacy Pediatric Care Intervention Arkansas8599 Einstein7485 Harvard9697 Miami6681 PA9295 Texas8087 Washington92 100 Yale91 103 TOTAL8594 JAMA. 1990;263:3035-3042

12
Effects of Psychosocial Risk Factors on Intelligence IQ RISKS: 3 children, > stressful life events, single parent, parental mental health problems, < responsive parenting, poverty, minority status, < social support

13
Cost Effective The cost of treating developmental problems early is substantially lower than treating a patient who is diagnosed late. May save society $30,000-$100,000 per child Patient and Family Satisfaction Parents want and expect support on child development. Screening can encourage parent involvement and investment in child’s health care.

14
Because we said so… AAP Council on Children with Disabilities recommends routine surveillance and standardized developmental and behavioral screening. Pediatrics 2006 Jul Policy reinforced in American Academy of Family Physicians AFP journal article. Am Fam Physician. 2011 Sep

15
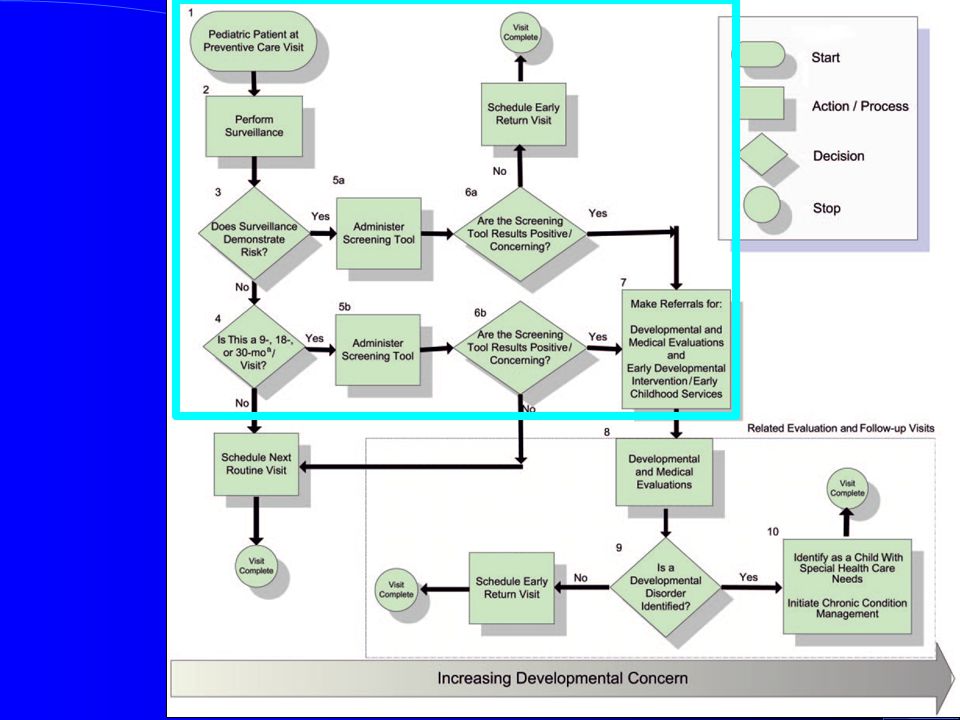
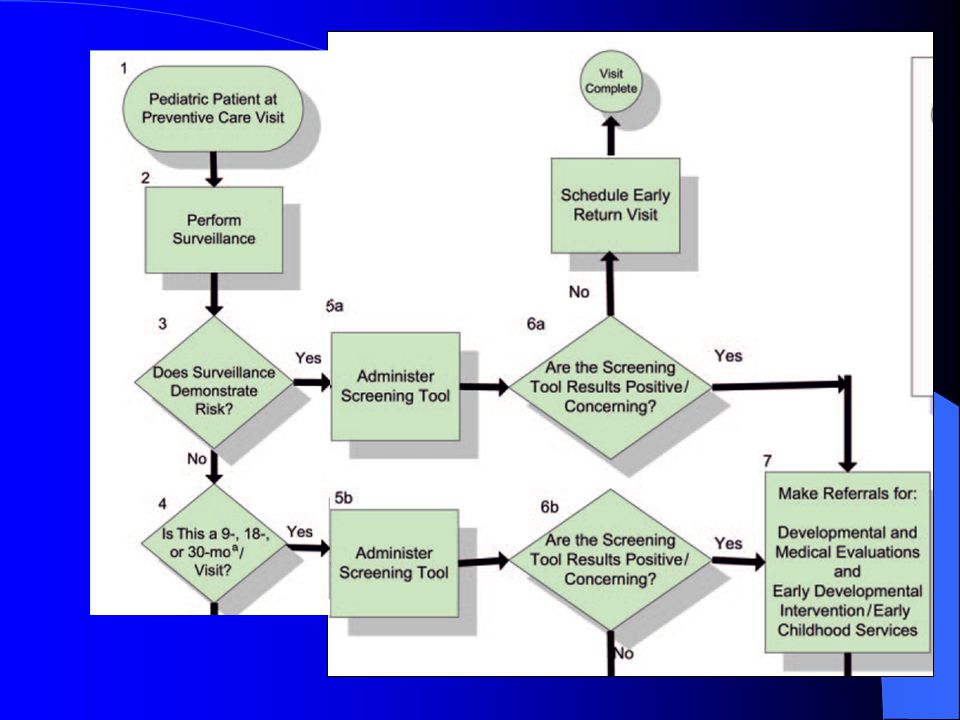
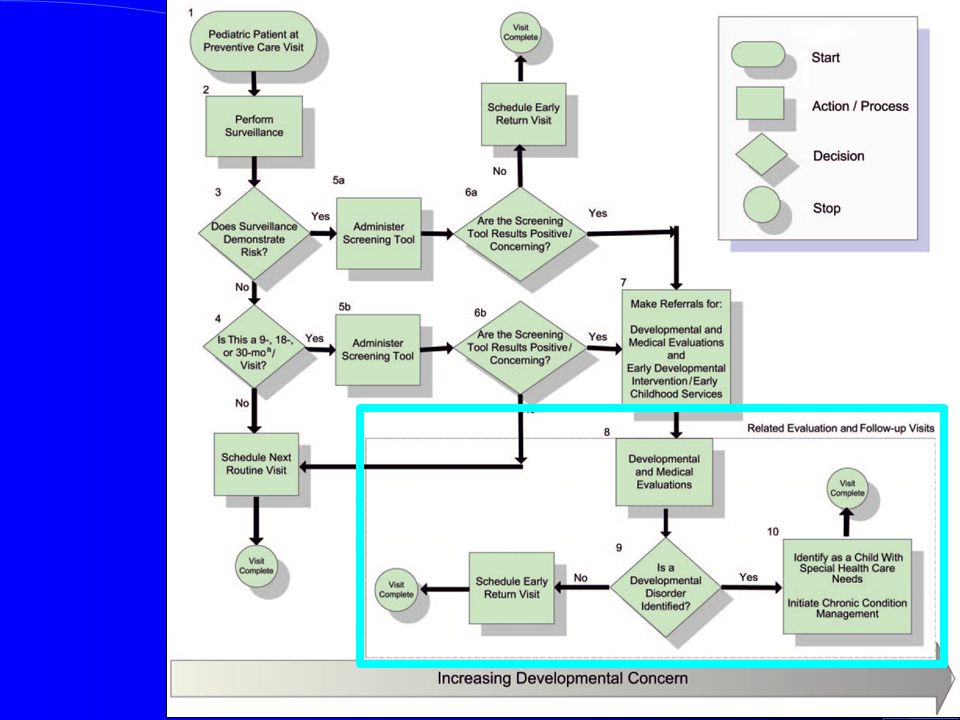
Guidelines Developmental surveillance at every well- child preventative care visit Developmental screening tests if: – Concerns exist, OR – Regularly at the 9-, 18-, 30-month visits Children identified with developmental disorders should be identified with a special health care need, and chronic-condition management should be initiated

16
AAP Policy Statement - 2006

22
Definitions Surveillance vs Screening

23
What is Surveillance? A flexible, continuous process, in which knowledgeable professionals perform skilled observations of children during child health care (in consultation w/families, specialists, child care providers, etc). SM Dworkin, A Shannon, and P Dworkin. ChildServ Curriculum. Center for Children’s Health and Development, St. Francis Hospital and Medical Center; 1999; Hartford, CT.
. SM Dworkin, A Shannon, and P Dworkin. ChildServ Curriculum. Center for Children’s Health and Development, St. Francis Hospital and Medical Center; 1999; Hartford, CT..")
24
Surveillance: 5 Components Eliciting and attending to the parent’s concerns Maintaining a developmental history Identifying the presence of risk and protective factors Making accurate and informed observations of the child Documenting the process and findings AAP Policy - Pediatrics 2006; 118; 405-420

25
What is Screening? Brief procedure using a standardized and validated developmental tool at pre- determined times Goal to differentiate children that are "probably ok" vs. "needing additional investigation” Performed at set points (eg. 9, 18, 24/30 months) OR if a specific concern arises* *AAP Policy - Pediatrics 2006; 118; 405-420
 OR if a specific concern arises* *AAP Policy - Pediatrics 2006; 118;")
26
Importance of Being Objective TOUCH OR TAKE TEMP?

27
Developmental Surveillance Versus Developmental Screening D-PIP Training Workshop Courtesy of Paul Lipkin MD FAAP: D-PIP Training Workshop 9 Months 18 Months 24/30 Months

28
A Typical Challenge Roger, new pt well visit, 2 years old Upset and crying when he checks in Mother reports he has limited words, does not listen, and has “temper tantrums” when he does not get his way How is this currently handled in your clinic? How would you like to handle it?

29
Screening’s Role In the optimal setting, primary care physicians have good surveillance skills - BUT Screening compliments continuous surveillance Research indicates effective screening is not always being done

30
Pediatrician Recognition of Developmental and Behavioral Problems Percent of Children Costello et al. Pediatrics. 1988;82:415-424 Sources: J. V. Lavigne et al, Pediatrics, Mar. 1993 91(3):649–55; E. J. Costello et al., “Pediatrics, Sept. 1988 82(3 Pt. 2):415–24. Slide thanks to: Edward L. Schor, MD
:649–55; E. J. Costello et al., Pediatrics, Sept (3 Pt. 2):415–24. Slide thanks to: Edward L. Schor, MD.")
31
Detection Rates Without Tools With Tools 20% of mental health problems identified (Lavigne et al. Pediatrics. 1993; 91:649-655) 30% of developmental disabilities identified (Palfrey et al. JPEDS. 1994; 111:651- 655) 80-90% with mental health problems identified (Sturner, JDBP 1991; 12:51-64) 70-80% with developmental disabilities correctly identified (Squires et al., JDBP 1996; 17:420- 427)
 30% of developmental disabilities identified (Palfrey et al. JPEDS. 1994; 111: ) 80-90% with mental health problems identified (Sturner, JDBP 1991; 12:51-64) 70-80% with developmental disabilities correctly identified (Squires et al., JDBP 1996; 17: ).")
32
Past Practices During Primary Care Visits Only 15-20% of pediatricians routinely use screening tests Most rely on developmental milestones or prompting for parental concern Only half of physicians in a national survey have a validated developmental screening instrument in their offices The Denver-II continues to be the predominant choice JDBP 24:409–417, 2003

33
The bad news… Practices that do not regularly screen for developmental, behavioral and emotional problems may miss opportunities for early referral and treatment.

34
Barriers to Screening Time Knowledge of tools and methods Familiarity with coding and billing procedures Referral resources JDBP 2003; 24:409–417

35
Challenges for Providers Resistance from within Lack of education on tools and their use Expectations about children’s development The “wait and see” approach Continued reliance on observations Failure to trust screening tests or results Reliance on poor quality or homemade tools

36
Challenges to Evaluating Children Development exists on a continuum Children manifest skills variably, inconsistently Developmental/behavioral problems increase with age – 2-3% of 0-18 month olds – 10% of 24-72 month olds – 16% of 0-21 year olds

37
The good news… The use of standardized screening tools increased significantly between 2002-2009. According to AAP periodic survey of fellows: 2002: 23% used one or more tools (always/almost always) 2009: 47% used one or more tools (always/almost always) Tools used: BINS, Denver II, ASQ, PEDS Pediatrics 2011; 128: 14-19
 2009: 47% used one or more tools (always/almost always) Tools used: BINS, Denver II, ASQ, PEDS Pediatrics 2011; 128:")
38
Summary/Intermission Developmental Screening is: Recommended by AAP & AAFP Different than surveillance Beneficial to children and practices Underutilized Challenging but rewarding to implement

39
Questions?

40
Tool Time ToolAgesAdmin timePsychometricsComments Ages and Stages Questionnaire B-66m10-15m, 1-3m scoring Normed, broad population $225 Unlimited copy Battelle Dev Inventory B-95m10-30m direct Normed, broad population $1280 Bayley Infant Screen 3-24m10-15m direct Normed, broad population $225 BriganceB-90m10-15m direct Normed, broad population $299 + data sheets Denver0-6y10-20m direct Normed, narrow population Parents’ Eval of Dev Status 0-8y2-10m, 1-2m scoring Standardized, broad population $36/ 50 copies I do not have any financial ties to any of these products (or any other ties!)
")
41
Time required: Parent 10-15 minutes to complete 3 minutes to score Cost: One time purchase; photocopying permitted or print from CD Features: Age-appropriate sensitivity and specificity; comes with suggestions for parents Adapted from: Michelle Macias MD FAAP, D PIP Training

42
Ages and Stages Questionnaire (ASQ) 2 Months to 5 Years 21 questionnaires from 1-66 months 30 - 35 items per form describing skills Taps 5 domains of development Validity is.82-.88; Test-retest reliability is.91 and inter- rater reliability is.92 ASQ-Social-Emotional (ASQ-SE) works similarly and measures behavior, temperament, etc.
 2 Months to 5 Years 21 questionnaires from 1-66 months items per form describing skills Taps 5 domains of development Validity is ; Test-retest reliability is.91 and inter- rater reliability is.92 ASQ-Social-Emotional (ASQ-SE) works similarly and measures behavior, temperament, etc.")
43
What’s new in ASQ-3? 2 and 9 month old questionnaire “Anytime screening” – ages 1-66 months Larger standardization population (15,138) Improved sensitivity (.86) and specificity (.85) Revised illustrations, wording, examples to improve accuracy
 Improved sensitivity (.86) and specificity (.85) Revised illustrations, wording, examples to improve accuracy.")
44
Ages & Stages ™ Sample Items 1. When your child wants something, does she tell you by pointing to it? Yes Sometimes Not Yet 4. Does your child say eight or more words in addition to “Mama” and “Dada”? Yes Sometimes Not Yet

45
Ages & Stages ™ Sample Item 48 months Using the shapes below to look at, does your child copy at least three shapes onto a large piece of paper using a pencil or crayon, without tracing? Your child’s drawings should look similar to the design of the shapes below, but they may be different in size. Yes Sometimes Not Yet

46
ASQ Scoring Communication Gross Motor Fine Motor Problem Solving Personal-Social Assign a value of 10 to yes, 5 to sometimes, 0 to not yet. Be sure each item has been answered The scoring grid below shows the cutoff score for each domain, indicated by the dark bar Any score touching or in the dark bar requires further evaluation

47
ASQ Scoring

48
Questions so far?

49
Autism Spectrum Disorders There has been a 600% increase in prevalence in the past 20 years 1 in 50 children* * Health Resources and Services Administration and Centers for Disease Control report – Mar13

50
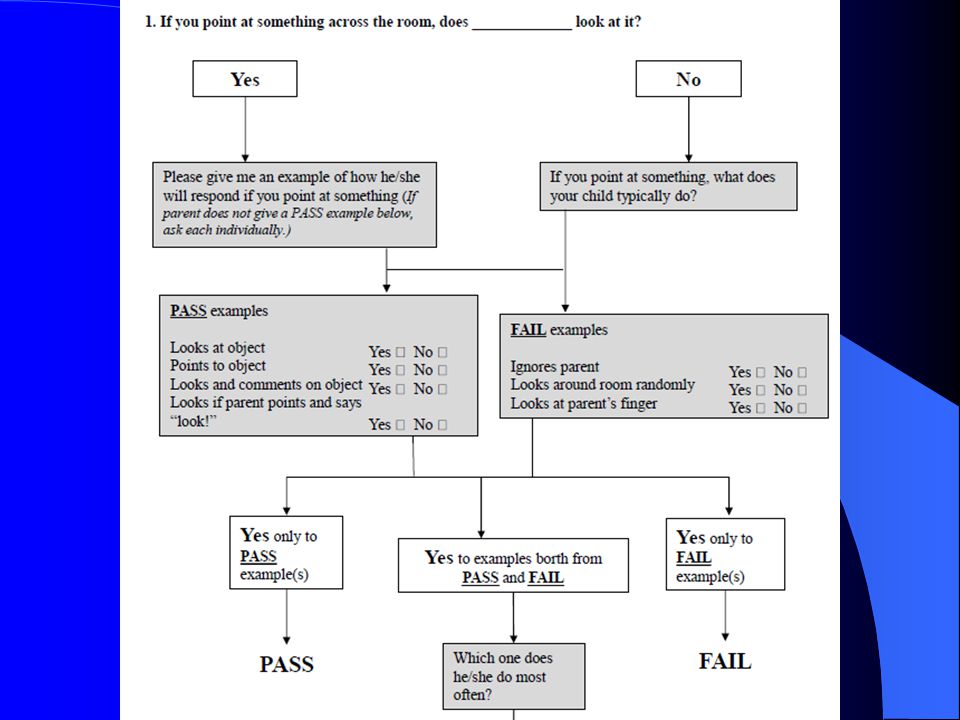
Modified Checklist for Autism in Toddlers (M-CHAT) Administered at 16-30 months 23 questions expanded and adapted from earlier CHAT (English or Spanish) – 1999 Modified to update/clarify language – 2009 Free: www.m-chat.orgwww.m-chat.org Available in >25 languages (including Icelandic) Can be scored in 2-5 minutes by a professional or paraprofessional Yes/No responses convert to Pass/Fail responses
 Administered at months 23 questions expanded and adapted from earlier CHAT (English or Spanish) – 1999 Modified to update/clarify language – 2009 Free: Available in >25 languages (including Icelandic) Can be scored in 2-5 minutes by a professional or paraprofessional Yes/No responses convert to Pass/Fail responses")
51
M-CHAT Considered “High-risk” if fails 8 or more items Recommended to refer directly for diagnostic evaluation Considered “Medium-risk” if fails 3 to 7 items Recommended to administer follow-up (second stage) questions Considered “Low-risk” if fails 2 or less items Recommended to continue routine surveillance and screening. Not all children who fail the checklist will meet all criteria for diagnosis on the autism spectrum

54
M-CHATR Follow-up Question/interview algorithm designed to further validate M-CHATR results Failure of any 2 items is considered significant – Refer for diagnostic testing

56
Summary Conduct surveillance at every pediatric health supervision visit Conduct screening when concerns arise OR at set intervals (9, 18, 24/30 months) If failure/concerns noted on screening tools – Refer family to Early Intervention/Help-Me-Grow services – Begin evaluation process (hearing, speech evaluation, etc) – Consider referral for full diagnostic evaluation (developmental pediatrics, child psychology, neurology, etc)
 If failure/concerns noted on screening tools – Refer family to Early Intervention/Help-Me-Grow services – Begin evaluation process (hearing, speech evaluation, etc) – Consider referral for full diagnostic evaluation (developmental pediatrics, child psychology, neurology, etc)")
57
Questions??

Similar presentations





 I have no relevant financial relationships with the manufacturer(s)>")



>")


>")


>")


 is notified ASAP about the evaluation result and service plans in order to have a follow-up with the family. PCP shares results.>")

: Early Screening & Diagnostic Assessment Laura Grofer Klinger, Ph.D. University of Alabama.>")


