Download presentation
Presentation is loading. Please wait.

1
Cancer of the Vulva

2
Essentials of Diagnosis Typically occurs in postmenopausal women. Long history of vulvar irritation with pruritus, local discomfort, and bloody discharge. Appearance of early lesions like that of chronic vulvar dermatitis. Appearance of late lesions like that of a large cauliflower, or a hard ulcerated area in the vulva. Biopsy necessary for diagnosis.

3
Types of Vulvar Cancer Squamous Cell Carcinoma- most common type of tumor (85-90%) and most frequently involves the anterior half of the vulva. Malignant Melanoma- second most common vulvar cancer (5%) Carcinoma of Bartholin's Gland- most common site for vulvar adenocarcinoma Basal Cell Carcinoma- arise almost exclusively in the skin of the labia majora
 Carcinoma of Bartholin s Gland- most common site for vulvar adenocarcinoma Basal Cell Carcinoma- arise almost exclusively in the skin of the labia majora.")
4
Squamous Cell carcinoma 65% arises in labia majora and minora 25% percent in clitoris or perineum Appearance varies from a large, exophytic, cauliflowerlike lesion to a small ulcer crater superimposed on a dystrophic lesion of the vulvar skin primary determinant of nodal metastases is tumor size.

5
Malignant Melanoma Accounts for 5% of vulvar cancers most commonly arises in the labia minora and clitoris superficial spread toward the urethra and vagina nonpigmented melanoma may closely resembles squamous cell carcinoma darkly pigmented, raised lesion is a characteristic finding

6
All small pigmented lesions of the vulva are suspect and should be removed by excision biopsy with a 0.5- to 1-cm margin of normal skin large tumors, the diagnosis should be confirmed by a biopsy

7
Carcinoma of Bartholin's Gland Rare (1%) but the most common site of vulvar adenocarcinoma Most common type is squamous cell
 but the most common site of vulvar adenocarcinoma Most common type is squamous cell")
8
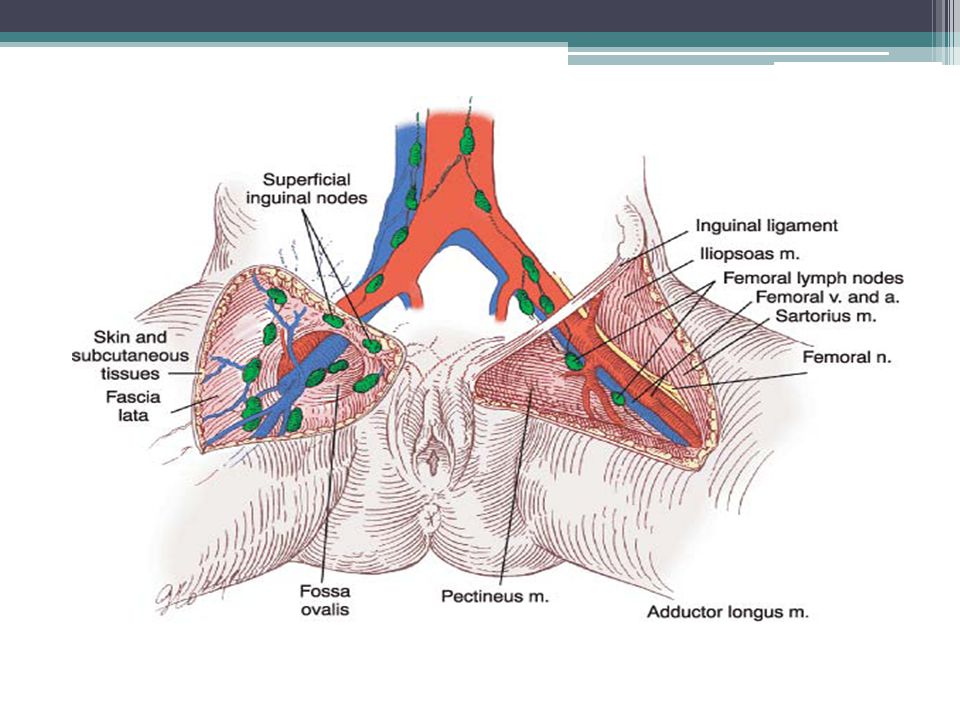
metastasis Primarily lymphatics to the superficial inguinal lymph nodes Direct extension to vagina, urethra and anus

12
Treatment TOC: wide local excision with inguinal lymph node metastasis Stage I: ipsilateral lymphadenectomy Stage II and III: bilateral lymphadenectomy Late stage III and IV: radical vulvectomy, lymphadenectomy and/or chemoradiation

13
Cancer of the Vagina

14
Rare, approximately 3% of gynecologic cancers Squamuos cell(85%)>adenocarcinomas> sarcomas>melanomas. Can be ulcerative or exophytic

15
Essentials of Diagnosis Asymptomatic: abnormal vaginal cytology. Early: painless bleeding from ulcerated tumor. Late: bleeding, pain, weight loss, swelling.

16
Endometrial Cancer 3 rd most common gynecologic malignancy in the Philippines Affects mostly peri/postmenopausal women RISK FACTORS: Estrogen replacement therapy4-8x Menopause after 52 years2.4x Obesity 3x-21 to 50lbs, 10x->50lbs Nulliparity 2-3x Diabetes2.8x Feminizing ovarian tumors Polycystic ovarian syndrome Tamoxifen therapy for breast cancer >2 years

17
Protective factors: Ovulation Progestin therapy Combination oral contraceptives Menopause prior to 49 years Normal weight Multiparity

18
Etiology: unopposed estrogen exposure Clinical presentation: Abnormal uterine bleeding (80) Physical exam ussually unremarkable
 Physical exam ussually unremarkable")
19
Staging FIGO Surgical Staging of Carcinoma of the Corpus Uteri Stage I Stage Ia G123 Tumor limited to endometrium Stage Ib G123 Invasion to less than one-half the myometrium Stage Ic G123 Invasion to more than one-half the myometrium Stage II Stage IIa G123 Endocervical glandular involvement only Stage IIb G123 Cervical stromal invasion Stage III Stage IIIa G123 Tumor invades serosa and/or adnexa, and/or positive peritoneal cytology Stage IIIb G123 Vaginal metastases Stage IIIc G123 Metastases to pelvic and/or paraaortic lymph nodes Stage IV Stage IVa G123 Tumor invades bladder and/or bowel mucosa Stage IVb Distant metastases including intra-abdominal and/or inguinal lymph nodes

20
Treatment Primary: surgery bilateral salpingo-oophorectomy, peritoneal washings for cytology, and removal of pelvic and periaortic lymph nodes Adjuvant Chemotherapy: for advanced stages Doxorubicin and cisplatin

21
Cancer of the Ovary

22
Epithelial -65% Germ cell- 20-25% Sex cord-6% Etiology =frequent ovulatio n Risk factors=nullipairty, decreased fertility, early and late menopause, ovulatory drugs

23
Clinical presentation Asymptomatic until late stage Enlarging abdomen, abdominal mass Urinary frequency, dysuria, GI complaints Metastasis to the umbilicus is known as Sister Mary Joseph Nodule

24
Epithelial Ovarian Cancer SEROUS- most common type MUCINOUS ENDOMETRIOID CLEAR CELL BRENNER

25
Management SURGERY- primary management CHEMOTHERAPY- ▫Paclitaxel-Carboplatin 6 cycles every 3-4 weeks CA-125- elevated in 80% of px with ovarian Ca -use to evaluate treatment

26
Germ cell Tumors 20-25% of ovarian cancers Arises from undifferentiated germ cells

27
Histologic Classification Dysgerminoma- most common malignant GCT Teratoma- most common GCT Endodermal sinus tumor Embryonal carcinoma Polyembryoma Choriocarcinoma Mixed forms

28
Serum Tumor Markers for Germ Cell Neoplasis tumorhCGAFPLDHCA-125 dysgerminoma++ Mixed germ cell tumor ++++ Embryonal Carcinoma +++ Endodermal sinus+

29
Clinical manifestation Tumors grow rapidly Distention of the ovarian capsule Hemorrhage Pelvic pain Pressure on rectum or bladder

30
Treatment Unilateral salpingo-oophorectomy Sensitive to chemotherapy- bleomycin, etoposide, cisplatin (BEC) Dysgerminomas- radiation theraPY SURVIVAL RATE(5 year): Dysgerminomas-85% Immature teratomas-70 to 80% Endodermal sinus tumors- 60 to 70%
 Dysgerminomas- radiation theraPY SURVIVAL RATE(5 year): Dysgerminomas-85% Immature teratomas-70 to 80% Endodermal sinus tumors- 60 to 70%")
31
Sex Cord-Stromal Tumors Low-grade malignancies Occur at any age Usually unilateral and do not often recur Functional tumors- produced hormones Granulosa-theca cells: large amounts of estrogens Sertoli-Leydig cells: testosterone and androgens

32
Granulosa-theca cell tumors Precocious puberty Menstrual irregularities Secondary ammenorrhea Post-menopausal bleeding Endometrial hyperplasia and/or endometrial cancer

33
Sertoli-Leydig Cell tumors Virilization: breast atrophy, hirsutism, deepened voice, acne, clitoromegaly and receding hairline Oligomenorrhea or amenorrhea

34
treatment Unilateral salpingo-oophorectomy Chemotherapy- not effective 5 year survival rate: 70-90%

35
Fallopian Tube Cancer Extremely rare: 0.5% of genital tract cancers 80-90% of FT malignancies are metastatic from other sites (ovary, uterus, GIT Unknown etiology Hereditary association (BRCA1)
")
36
Clinical manifestation Hydrops tubae profluens: profuse watery discharge, pelvic pain and pelvic mass - Classic triad of fallopian Ca, only 15% of cases, pathognomonic

37
Treatment TAHBSO, retriperitoneal lymph node sampling Carboplatin and paclitaxel- adjunct therapy

Similar presentations

















>")



