Download presentation
Presentation is loading. Please wait.

1
Treatment of Acute Lower Gastrointestinal Bleeding Experience of a Specialized Management Team Eric J. Dozois, MD Division of Colon & Rectal Surgery Mayo Clinic Rochester, Minnesota

2
Acute GI Bleeding Significant health problem : Morbidity Mortality Cost Disease of the Elderly : By 2050, 78 million Americans will be 65 years or older

3
Lower Gastrointestinal Bleeding (LGIB) Background Distinct entity from upper GI bleeding Spectrum of disease is broad Trivial hematochezia to massive hemorrhage and shock
 Background Distinct entity from upper GI bleeding Spectrum of disease is broad Trivial hematochezia to massive hemorrhage and shock")
4
Lower GI Bleed Background – Management Pathway Assessment of severity Establishment of diagnosis Appropriate use of resources Control of bleeding Prevention of rebleeding Lower morbidity, mortality, cost

5
Acute Gastrointestinal Bleeding Management - Advances Growth of Therapeutic Endoscopy:* – Decrease length of hospitalization – Decrease transfusion requirements – Lowers need for surgical intervention – Reduced mortality *Sacks et al JAMA 1990;264:494-9

6
Gastrointestinal Bleeding Team Mayo Clinic - Background Surgeons ER Physicians Radiologists Pharmacists ICU Physicians 1988 Mayo Clinic Gastrointestinal Bleeding Team (GIBT)
")
7
Management of Acute GI Bleeding Mayo Clinic - Background Designed to satisfy the need for rapid and specialized endoscopic management of acute GI conditions, primarily GI bleeding

8
Mayo Clinic GI Bleed Team Rapid response, 24/7 service Response time for emergent endoscopy is < 30 minutes Involved until patient stabilized or surgery intervention

9
Members of Team 1 Staff Endoscopist (1 - wk rotation) 1-2 GI Fellows (1 - mo rotation) 1 Endoscopy nurse (1 - wk rotation) 1-2 full-time study coordinators Colorectal or General Surgeon
 1-2 GI Fellows (1 - mo rotation) 1 Endoscopy nurse (1 - wk rotation) 1-2 full-time study coordinators Colorectal or General Surgeon")
10
Mayo Clinic GI Bleed Team Scope of Practice : ER, clinic, hospital, OR All endoscopic emergencies – Food impaction – Foreign body removal – Colonic decompression (stents)
")
12
Early Assessment – High Risk Screening Criteria Historical Criteria: – Age > 65 years – Previous bleeding; identified site(s) – Major organ system disease, aortic graft Clinical Criteria: – SBP 20, HR > 100 – Transfusion of > 4U/24hrs, 8U hospital stay – Re-bleed event > 2U
 – Major organ system disease, aortic graft Clinical Criteria: – SBP 20, HR > 100 – Transfusion of > 4U/24hrs, 8U hospital stay – Re-bleed event > 2U")
13
GIBT - Bowel Prep GoLYTELY: – 4 oz. Q 5 min. until effluent clear OR – 4 liter down NG tube over 2 hours

15
GIBT - Equipment Motorized, mobile unit State-of-the-art: DVD recording Accessories Scopes

16
GIBT - Database Prospectively collected data on all patients Indications, findings, therapeutic modality, complications and outcome Enhances research productivity related to GI bleeding and other GI emergencies

17
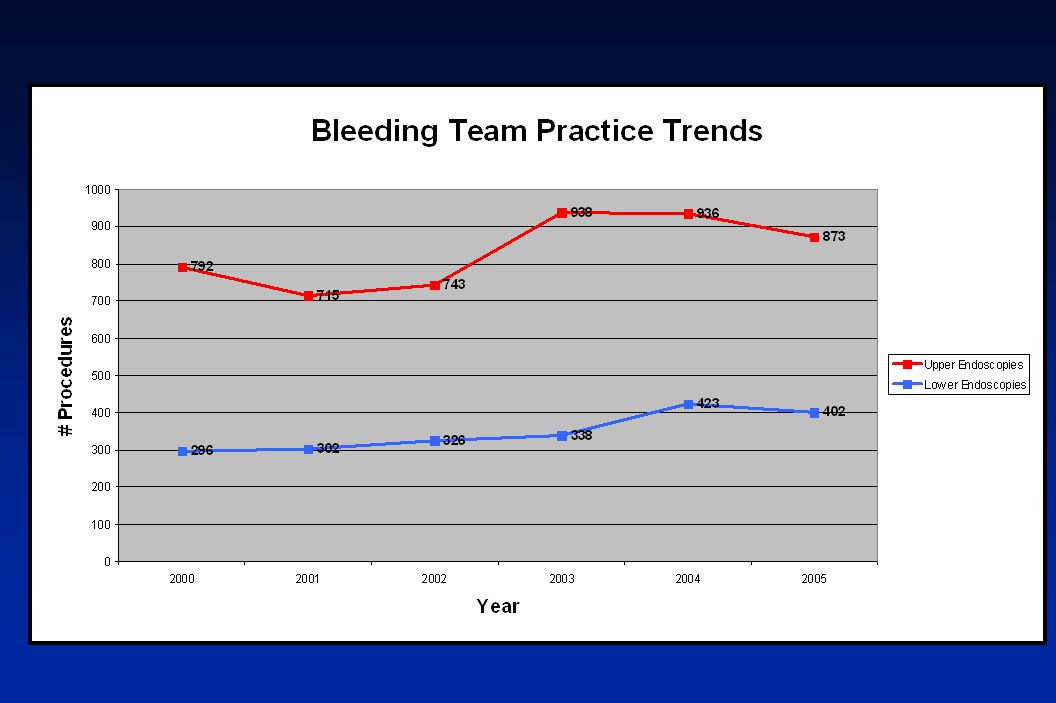
Year-end 2005 > 42,000 Procedures

18
Extra procedures include PEG/PEJ, bedside NG-NJ tube placement, etc.

21
All GI Bleeding Etiologies - 2005 PUD 29% Gastroesophageal varices 7% Vascular ectasias 6% Diverticular bleeding 6% Postpolypectomy 4% Colonic ulcers 4% Ischemia 3% Mallory-Weiss tear 3% Malignancy 0.8% Anastomotic site 0.7% Dieulafoy 0.1%

22
Causes of LGI Bleeding - 2005 Diverticular21% Ulcers/erosions 15% NSAID, infection, idiopathic Ischemic colitis12% Post-polypectomy11% Vascular ectasias 8% Malignancy 2% Anastomotic site 2%

23
Lower GI Bleed Risk Factors for Mortality* Age > 70 years Vital organ disease (*heart, liver, lungs) History of Cancer Shock Re-bleeding (> 4 units/event) Hospitalized patients *With permission from CJ Gostout, MD
 History of Cancer Shock Re-bleeding (> 4 units/event) Hospitalized patients *With permission from CJ Gostout, MD")
24
Lower GI Bleed Risk Factors for Re-bleeding Bleeding > 24 hours Hemodynamic instability Hemoglobin, 10 g/dL Anticoagulation/coagulation disorder Cirrhosis Transfusion > 4 U per resuscitation event Undiagnosed prior major bleeding *With permission from CJ Gostout, MD

25
GIBT – Complications Study Period 1989 - 2000 No. of Cases10,520 Complications 230 Gostout et al. AJG 2001;96:3452 Complication Rate 2.19%

26
GIBT – Complications Gostout et al. AJG 2001;96:3452 Iatrogenic bleeding24.3% Perforation20.0% Hypoxia 9.6% Hypotension 9.6% Mucosal tears 8.0% Arrhythmias 6.1% Aspiration 3.0% Death 2.0%

27
GIBT - Technical Expertise Injection: Epi, sclerosants, cyanoacrylate glue Thermal : Heat probe, Bipolar electrocoagulation Mechanical : Clipping, Banding, Cryotherapy

28
Endoscopic Management LGIB Principles: – If active bleeding, inject epinephrine (1:10,000) to slow or stop bleeding – Epinephrine is generally a temporary solution and used as an adjunct to definitive therapy (e.g., clipping or thermal coagulation)
 to slow or stop bleeding – Epinephrine is generally a temporary solution and used as an adjunct to definitive therapy (e.g., clipping or thermal coagulation)")
29
Endoscopic Management LGIB Principles: – If feasible, clipping generally preferred in the colon due to perceived increased safety relative to thermal techniques – Clipping and thermal coagulation techniques are equally effective for most bleeding colonic lesions

30
Indications for Clips Mallory-Weiss Tear Peptic Ulcer Disease Dieulafoy lesion Post-polypectomy bleeding Diverticular bleeding Angioectasias* (*APC or contact thermal modality preferred) Raju GS et al. Gastrointest Endosc 2004;59:267

31
Vascular Ectasia Non-BleedingBleeding Coaptive Coagulation APC (preferred) Epinephrine Injection Coaptive Coagulation APC (preferred) Clipping not optimal for vascular ectasias
 Epinephrine Injection Coaptive Coagulation APC (preferred) Clipping not optimal for vascular ectasias")
32
Diverticular & Postpolypectomy Bleeding Angiographic Embolization Coaptive Coagulation Clipping (preferred) Epinephrine Injection Coaptive Coagulation Clipping failed
 Epinephrine Injection Coaptive Coagulation Clipping failed")
33
Anastomotic Site Bleed StigmataActive Bleed Coaptive Coagulation Clipping (preferred) Epinephrine Injection Coaptive Coagulation Clipping (preferred)
 Epinephrine Injection Coaptive Coagulation Clipping (preferred)")
34
Conclusions Mayo Clinic GI Bleed Team Organized, highly skilled team Delivers immediate and advanced endoscopic therapy to patients with acute GI bleeding Should improved outcomes

35
Mayo GIBT – Future Research How will the presence of the GIBT effected: Mortality, Morbidity, Cost Transfusion requirements Need for surgical intervention Length of hospital stay

Similar presentations













 682-3793; (p) 413-3222.>")






