Download presentation
Presentation is loading. Please wait.

1
HOW I DO IT ? MODIFIED NORWOOD’S OPERATION
VICHAI BENJACHOLAMAS, MD. CHULALONGKORN HOSPITAL

2
HYPOPLASTIC LEFT HEART SYNDROME
Mitral valve atresia or stenosis Small left ventricle Aortic valve atresia or stenosis Small ascending aorta Various degree of aortic arch obstruction

3
HYPOPLASTIC LEFT HEART SYNDROME

4
HYPOPLASTIC LEFT HEART SYNDROME
Perop. Management PGE-1 open PDA Avoid oxygen Correct acidosis Inotrope Diuretic Intubation if neccessary

5
HYPOPLASTIC LEFT HEART SYNDROME
Hybrid procedure VS Modified Norwood’s operation

6
HYPOPLASTIC LEFT HEART SYNDROME
Hybrid procedure PDA stenting Bilateral PA banding +/- balloon atrial septostomy

7
HYPOPLASTIC LEFT HEART SYNDROME
Modified Norwood’s operation Aortic and arch reconstruction with/without homograft Atrial septectomy Shunt to pulmonary artery BT shunt or Sano shunt

8
HYPOPLASTIC LEFT HEART SYNDROME
Timing for Norwood’s operation AGE < = 10 days

9
MATERIALS AND METHODS August 1996 - November 2008
Modified Norwood’s Operation was performed in 26 neonates

10
AGE 3 - 75 days ( median 11 days )
MATERIALS AND METHODS AGE days ( median 11 days )
")
11
WEIGHT 2,000 - 4,200 grams ( median 2,850 grams )
MATERIALS AND METHODS WEIGHT 2, ,200 grams ( median 2,850 grams )
")
12
ASCENDING AORTA DIAMETER 2 - 7 mm. ( median 2.5 mm. )
MATERIALS AND METHODS ASCENDING AORTA DIAMETER 2 - 7 mm. ( median 2.5 mm. )
")
13
HOW I DO IT ?

14
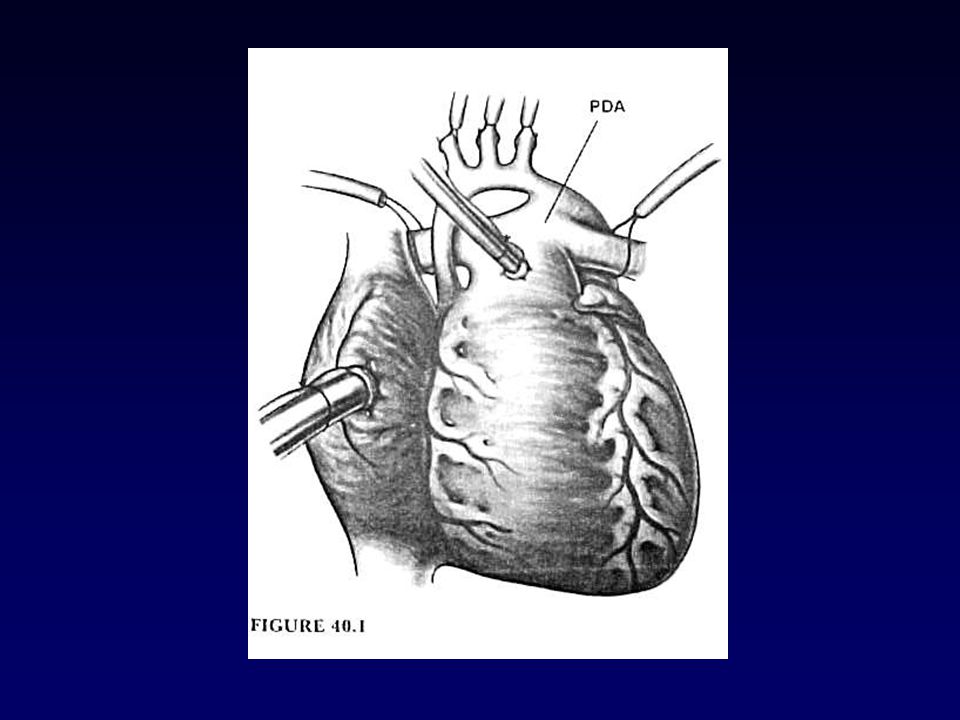
SURGICAL TECHNIQUE Operate under cardiopulmonary bypass
with profound hypothermia Arterial cannulation - at MPA for first 10 patients - at Goretex graft to right bracheo- cephalic artery for last 16 patients Venous cannulation with single venous at Rt. Atrial appendage

16
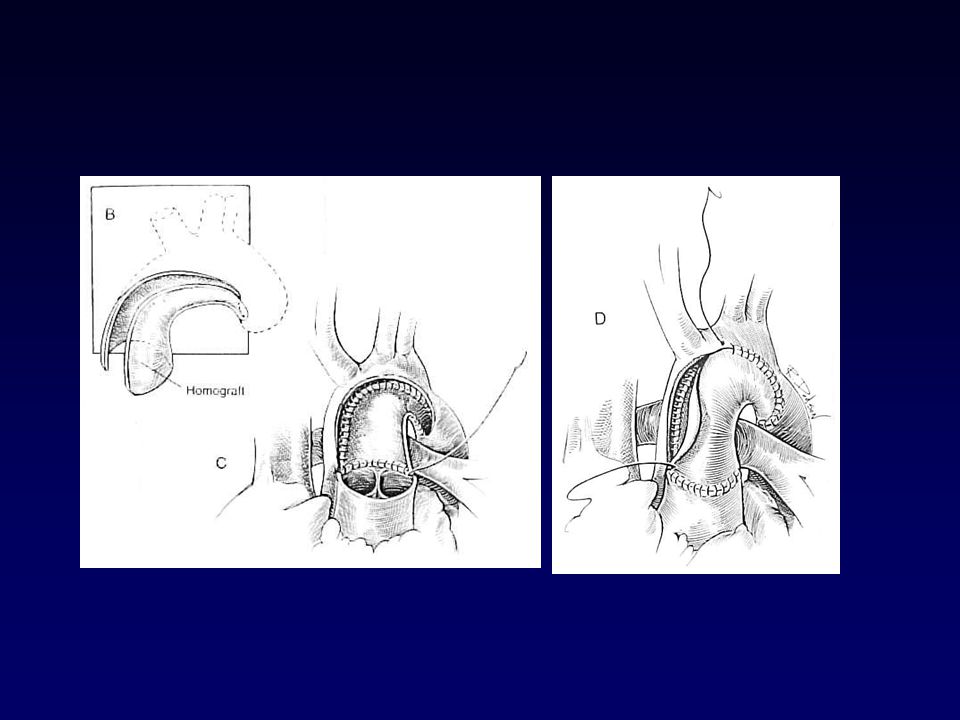
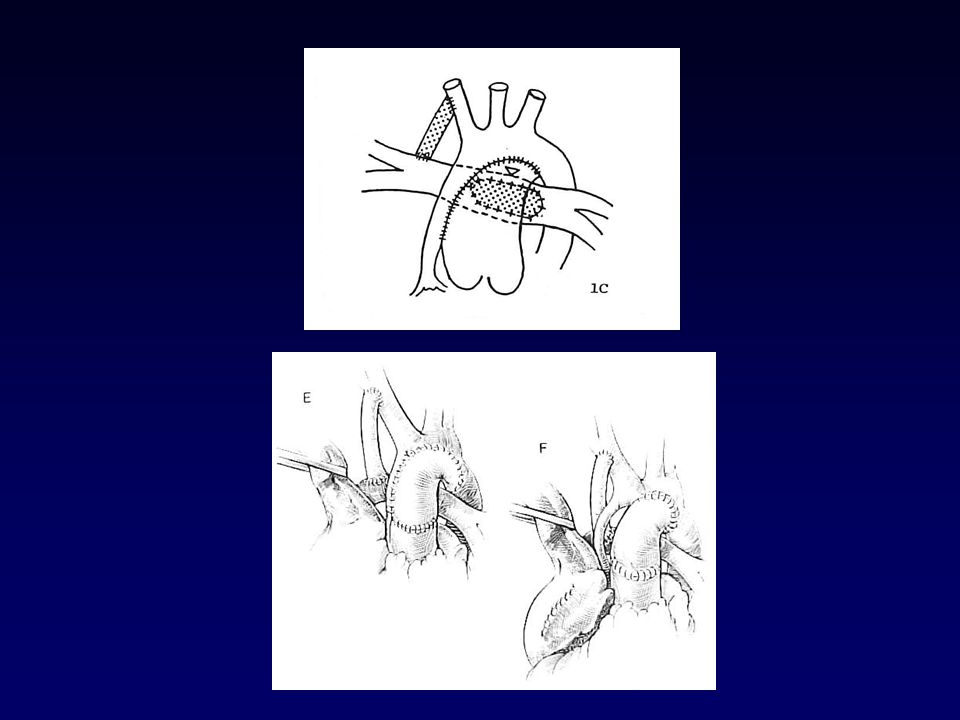
SURGICAL TECHNIQUE Resected PDA tissue and aortic ischmus
Arch reconstruction with MPA or homograft Atrial septectomy Rt. Modified Blalock-Taussig shunt

20
SURGICAL TECHNIQUE Homograft = 22 patients aortic = 3/22 patients
Arch reconstruction with native MPA = patients Homograft = 22 patients aortic = 3/22 patients pulmonic = 19/22 patients

22
SURGICAL TECHNIQUE BT Shunt size selection
3.5 mm. for Body weight <= 3.5 kg. 4.0 mm. for Body weight > 3.5 kg.

23
SURGICAL TECHNIQUE Median CPB time
= min. ( min.) Median DHCA time = min. (51-97 min.) Median CPB+ DHCA time = min. ( min.)
 Median DHCA time. = 66 min. (51-97 min.) Median CPB+ DHCA time. = 159 min. ( min.)")
24
SURGICAL TECHNIQUE BT shunt VS Sano shunt

25
SURGICAL TECHNIQUE Advantages/disadvantages of the modified Blalock-Taussig shunt Advantages Disadvantages No ventriculotomy Increased diastolic runoff Decreased coronary perfusion Decreased right ventricle function Decreased end organ perfusion Limits right ventricle overload Shunt stenosis/thrombosis Good pulmonary artery growth

26
SURGICAL TECHNIQUE Advantages/disadvantages of the Sano shunt
Improved coronary perfusion Higher diastolic pressure Narrowed pulse pressure Right ventriculotomy Arrhythmias Right ventricle dysfunction Right ventricle aneurysm Tricuspid valve dysfunction Lower pulmonary to systemic ratio Early or progressive hypoxemia Pulsatile pulmonary blood flow Increased volume load on right ventricle Improved end-organ perfusion Inadequate pulmonary artery growth Shunt stenosis/thrombosis

27
Sano shunt benefit in AA, MA
SURGICAL TECHNIQUE Sano shunt benefit in AA, MA

28
POSTOPERATIVE CARE RULE OF FOURTY (40) - Fi O2 ~ 0.40
- Pa CO 2 ~ mmHg. - Pa O2 ~ mmHg. - Hct. ~ 40 %

29
78 - 85 % ( average 82 % ) POSTOPERATIVE CARE Oxygen saturation
after extubation % ( average 82 % )
")
30
Survival rate = 76.9 % (20/26) RESULTS
Hospital mortality was % (6/26 ) (within 30 days) DOT 3/6 Survival rate = 76.9 % (20/26)
 (within 30 days) DOT 3/6. Survival rate = 76.9 % (20/26)")
31
RESULTS Mortality rate by arch reconstruction technique
Autologous tissue mortality rate = 50 % (2/4) survival rate = 50 % (2/4) Homograft patch mortality rate = 18.2 % (4/22) survival rate = 81.8 % (18/22)
 survival rate = 50 % (2/4) Homograft patch. mortality rate = 18.2 % (4/22) survival rate = 81.8 % (18/22)")
32
LATE RESULTS 26 patients 20 survivors 3 loss F/U 5 BDG
1 wait for FONTAN 4 FONTAN 2 waiting for BDG 5 not suitable for BDG 5 BTS 1 FONTAN 2 F/U 2 LD 5 LD 6 HD

33
DISCUSSION PRE-OPERATION - Need experienced cardiologist to take
care the patient before operation - Not to put ET tube in the patient - Stabilize cardiovascular, no acidosis

34
DISCUSSION INTRA-OPERATION - Arch reconstruction with homograft seem
to be better ( smooth postoperative care, early extubation and no late coarctation, especially pulmonary homograft ) - Select proper shunt size to maintain O2 saturation ~ %
 - Select proper shunt size to maintain. O2 saturation ~ %")
35
DISCUSSION POST-OPERATION - Early catheterization at either
5 or 6 mo. old or progress cyanosis - Change to BCP shunt before out-growth of the BT shunt

36
SUMMARY The treatment of hypoplastic left heart syndrome need a lot effort. Despite good equipment, it needs very good team include neonatal cardiologist, neonatal cardiac anesthetist, neonatal cardiac surgeon, well- trained scrub nurse, keen perfusionist, and keen ICU nurse.

Similar presentations






















 when the heart contracts. They.>")