Download presentation
Presentation is loading. Please wait.

1
Primary bone tumours of the Spine: Imaging and Pathology David Ritchie Robin Reid

2
Incidence: primary spinal (38) and sacral (14) tumours SBTR (2000-09), 52 patients Benign21Malignant31 ABC 6 (1)Chordoma 10 (4) Osteoblastoma 6 (1)Ewings 8 (3) Osteoid osteoma5Chondrosarcoma 5 (1) Giant Cell Tumour 1 (1)Myeloma 3 (1) Eosinophilic Gran1Plasmacytoma 2 (1) Chondroma1Osteosarcoma 2 (1) Fibrous Dysplasia1Haemangioendoth1 (x) Sacral tumour C spine (7), D spine (21), L spine (10)
 and sacral (14) tumours SBTR ( ), 52 patients Benign21Malignant31 ABC 6 (1)Chordoma 10 (4) Osteoblastoma 6 (1)Ewings 8 (3) Osteoid osteoma5Chondrosarcoma 5 (1) Giant Cell Tumour 1 (1)Myeloma 3 (1) Eosinophilic Gran1Plasmacytoma 2 (1) Chondroma1Osteosarcoma 2 (1) Fibrous Dysplasia1Haemangioendoth1 (x) Sacral tumour C spine (7), D spine (21), L spine (10)")
3
Spine – Tumours - Location ANTERIOR – Malignant Metastases Myeloma Lymphoma Exceptions Eosinophilic granuloma Haemangioma Giant cell tumour POSTERIOR - Benign Osteoblastoma Osteoid osteoma Aneurysmal bone cyst Osteochondroma Exceptions Sarcoma

4
KM, SBTR 4706 17F, 2/12 Hx of intermittant thoracolumbar pain Worse at night

8
Aneurysmal bone cyst Children/ young adults Metaphysis of long bones, spine Sponge-like mass, blood filled spaces Septa, fibroblasts, giant cells, osteoid Mitoses, but normal No endothelial lining Recur in 25%

12
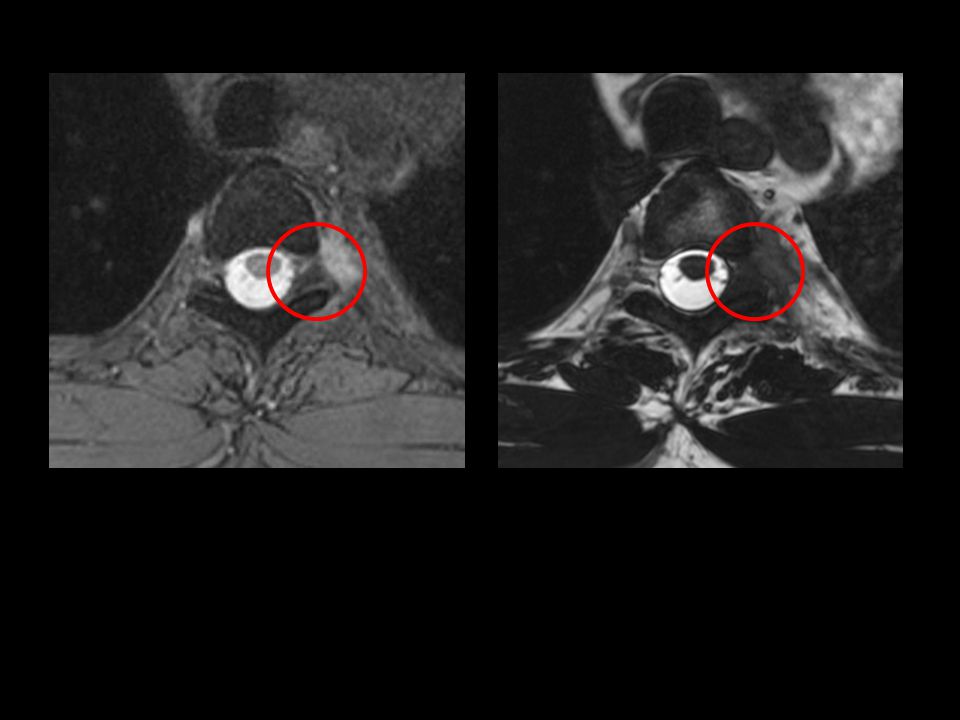
Aneurysmal Bone Cyst SBTR 4278, RW Clinical and Imaging 80% 1 st - 2 nd decades Benign expansile lesion containing thin-walled blood filled cavities Thin cortical shell and foci of cortical destruction Absent matrix Fluid-fluid levels caused by blood product sedimentation Differential diagnosis Osteoblastoma Giant cell tumour Telangiectatic osteosarcoma Brown tumour of hyperparathyoidism T2W T1W

13
SS, SBTR 4394 50M, Increasing LBP, Right buttock pain radiating to knee No bladder or bowel problems

16
AE1/3 and S100

17
Chordoma NeuroaxisNeuroaxis –Base of skull –Sacrum –Vertebrae Arises from notochord remnantArises from notochord remnant Local recurrence and extension usualLocal recurrence and extension usual Metastasis in <10%Metastasis in <10%

19
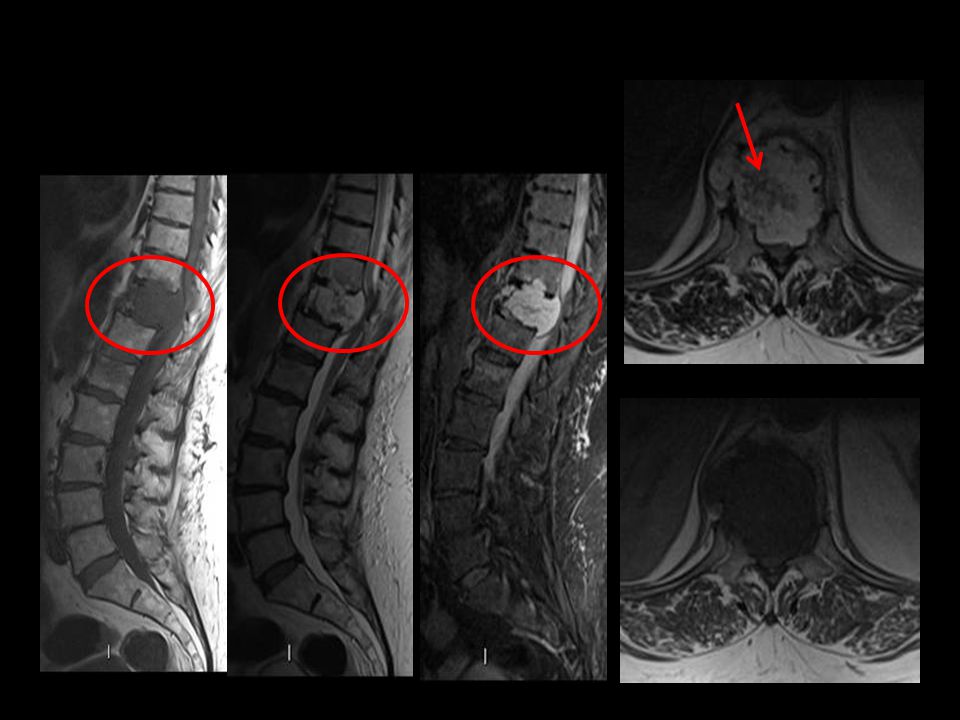
Chordoma Differential diagnosis Metastasis / Lymphoma / Myeloma Chondrosarcoma Giant cell tumour Osteosarcoma Clinical 50% of 1º malignant sacral tumours 50% of chordomas arise in sacrum 4-7th decades, 2M:1F Slow growing painful mass Low grade but recurrence common Metastases late (5 – 43%) 5 year survival rate 60-80% T2W STIR Recurrent / metastatic chordoma
 5 year survival rate 60-80% T2W STIR Recurrent / metastatic chordoma")
20
Surgery for Sacral Tumours Preserve power/sensation legs - S1 roots Preserve bowel / bladder function - S2 roots Retention of sexual function - S3 root - M, S2 - F Stability of the lumbo-sacral junction Preservation of neurological function Raque et al. Treatment of neoplastic diseases of the sacrum. J Surg Oncol 2001; 76: 301

21
DH, SBTR 4604 P,10.2841 CHI 0710726171 Chordoma LV3

22
PC, SBTR 4591 31M, 2yr Hx mid thoracic / periscapular pain Scoliosis

26
Osteoid Osteoma Central nidus (<1cm) of vascular/gritty tissue Subperiosteal or cortical lesions provoke intense reactive new bone formation Nidus: active osteoblasts forming bone osteoclastic remodelling, very vascular Natural history: sometimes recur following incomplete excision Rare spontaneous regression suggests osteoid osteoma may not be neoplastic
 of vascular/gritty tissue Subperiosteal or cortical lesions provoke intense reactive new bone formation Nidus: active osteoblasts forming bone osteoclastic remodelling, very vascular Natural history: sometimes recur following incomplete excision Rare spontaneous regression suggests osteoid osteoma may not be neoplastic")
31
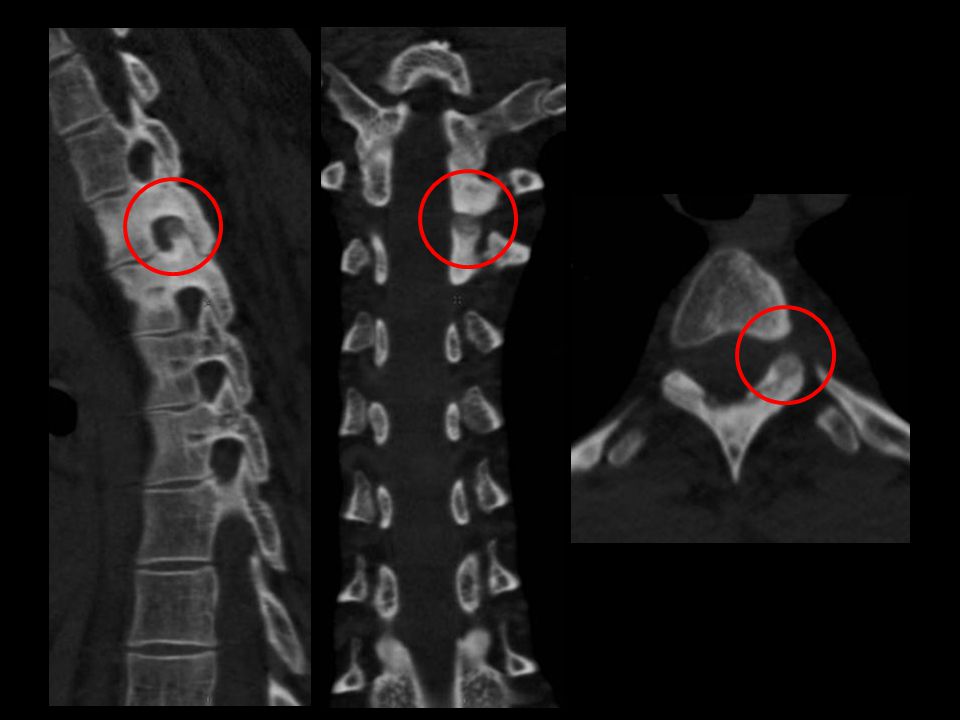
Osteoid Osteoma Clinical and Imaging Benign bone forming tumour 10% in axial skeleton 90% in 2 nd – 3 rd decades, 3M:1F Night pain relieved by non-steroidal analgesia Usually arise posterior elements Nidus <15mm, lucent but often mineralisations Reactive sclerosis / peri-tumoral oedema CT best cross-sectional imaging technique Differential diagnosis Chronic infection Bone island

32
SPINE T2WCT 28M, LBP R sciatica

33
Osteoblastoma “Giant osteoid osteoma” 2-10cm 1% of bone tumours Wide age range, mainly 10-30 years Spine (posterior elements), long bones Swelling, dull pain,nerve compression, Histology as in osteoid osteoma Local recurrence after curettage (?multifocality)
, long bones Swelling, dull pain,nerve compression, Histology as in osteoid osteoma Local recurrence after curettage ( multifocality)")
37
Osteoblastoma Clinical and Imaging Uncommon benign bone forming tumour Histologically similar to osteoid osteoma 90% in 2 nd – 3 rd decades, 2M:1F 3 imaging patterns –Large “osteoid osteoma” –Expansile mineralised lesion –Occasionally aggressive Differential diagnosis Osteoid osteoma Aneurysmal bone cyst Osteosarcoma

43
SR, SBTR 4623 72F Bilateral lower limb pain & loss of power and paraesthesia both thighs

45
Ritchie

49
Chondrosarcoma – conventional de novo (primary) or from a pre-existing enchondroma or exostosis (secondary) Central,within the medullary canal or peripheral on bone surface 10% of malignant primary bone tumours predominantly middle aged and elderly Males: females; 2:1 axial skeleton, pelvis, ribs, shoulder girdle proximal femur and humerus. Hands and feet rare

50
Proportion of tumours % metastatic rate grade 164%5% grade 221%14% grade 315%75%

51
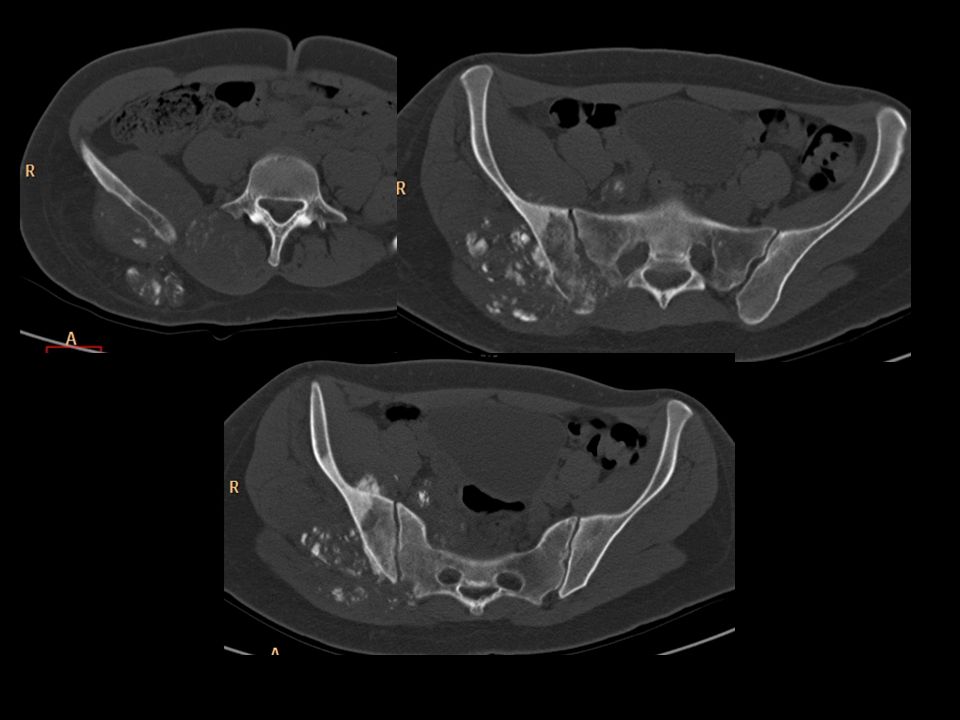
Chondrosarcoma Clinical and Imaging 7 - 12% of primary malignant spinal tumours 4th – 6 th decades Low grade - geographic growth pattern High grade - permeative growth pattern CT detects mineralisation in 90% MR – Unmineralised cartilage shows lobules of high signal on T2W separated by low signal septae Calcifications may display signal voids T1W T2W CT Differential diagnosis Chordoma Metastasis Myeloma Giant cell tumour

52
SBTR 4322, CH, 18F, 4/12 Hx right buttock / thigh pain and inguinal paraesthesia More recently bilateral thigh and buttock pain Urinary problems and decreased perianal tone

58
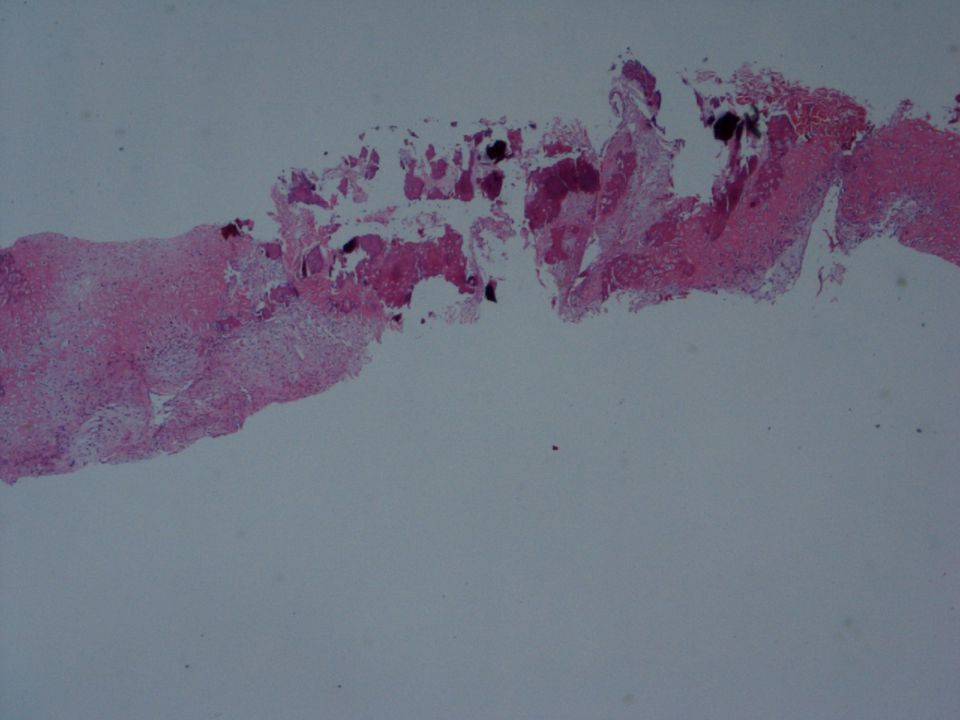
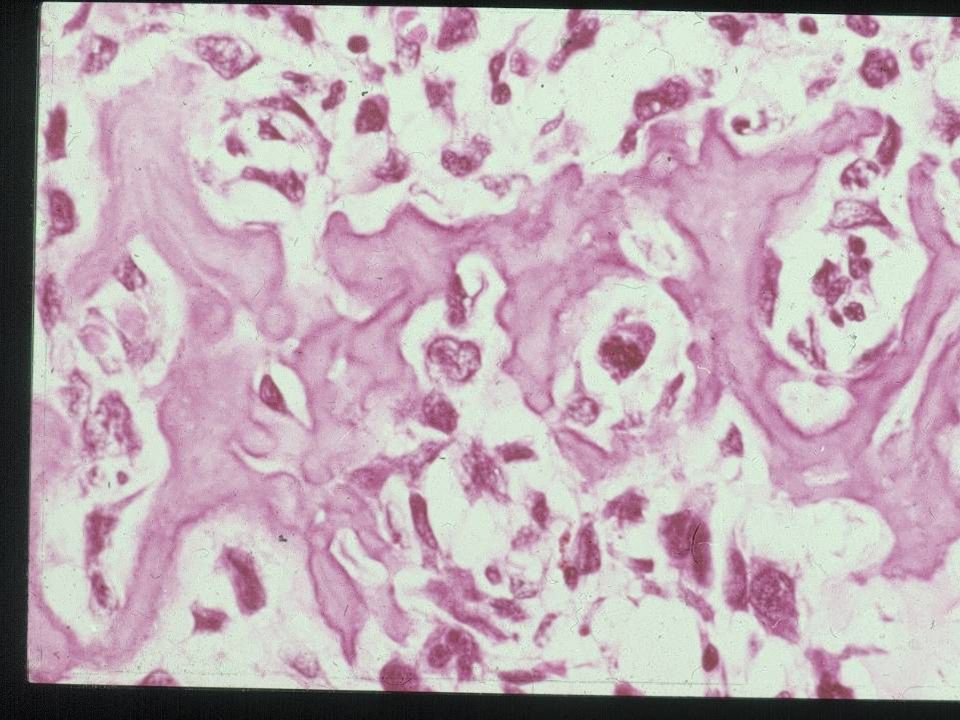
Osteosarcoma a malignant tumour whose cells form osteoid or bone

60
CH

61
Osteosarcoma Clinical and Imaging 5% of primary malignant spinal tumours 4th decade (older than long bone) Associated with Paget’s, DXRT Mixed lytic / sclerotic appearance Aggressive, soft tissue extension Osteoid mineralisation T1WT2W T1W CT Differential diagnosis Ewings Chondrosarcoma Metastasis Osteoblastoma Lymphoma
 Associated with Paget’s, DXRT Mixed lytic / sclerotic appearance Aggressive, soft tissue extension Osteoid mineralisation T1WT2W T1W CT Differential diagnosis Ewings Chondrosarcoma Metastasis Osteoblastoma Lymphoma")
Similar presentations






























>")








 normal cell of origin Most are classified.>")

 October 29, 2008.>")





