Download presentation
Presentation is loading. Please wait.

1
Regional Anaesthesia and Thromboprophylaxis Dr Kate Fogg Royal Brompton Hospital

2
Regional Anaesthesia Regional AnaesthesiaEpidural/spinalRisks/benefits Thromboprophylaxis Thromboprophylaxis s/c heparin (unfractionated/LMWH) anti-Xa or direct thrombin inhibitors antiplatelet agents warfarin systemic heparinisation Can you put the two together or should you stop one in order to perform the other?
 anti-Xa or direct thrombin inhibitors antiplatelet agents warfarin systemic heparinisation Can you put the two together or should you stop one in order to perform the other")
3
Regional blocks Drug administered directly to the spinal cord to locally block afferent and efferent nerve input. Drug administered directly to the spinal cord to locally block afferent and efferent nerve input. Usually for major thoracic, abdominal and lower limb surgery Usually for major thoracic, abdominal and lower limb surgery Local anaesthetic +/- opiates Local anaesthetic +/- opiates

5
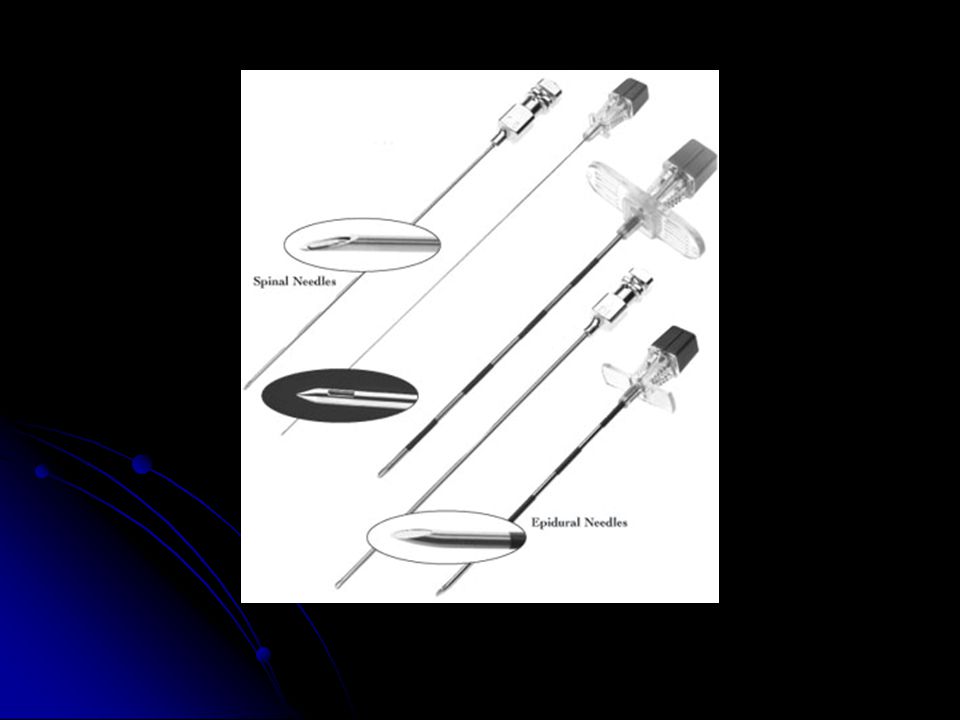
Spinal Dural puncture Dural puncture Single shot usually Single shot usually 24-26G needle, pencil point 24-26G needle, pencil point Less traumatic Less traumatic Catheter rarely Catheter rarely

6
Epidural Larger needle – 16 G Larger needle – 16 G Loss of resistance technique Loss of resistance technique Epidural vessels Epidural vessels Usually a catheter technique Usually a catheter technique Trauma may be on insertion or removal of catheter Trauma may be on insertion or removal of catheter

7
Benefits Improved analgesia, greater mobility, fewer opiate side-effects Improved analgesia, greater mobility, fewer opiate side-effects Decrease stress response Decrease stress response adverse cardiac, pulmonary and immune outcomes hypercoagulable state Decrease troponin release in cardiac patients Decrease troponin release in cardiac patients ? Does this translate into clinical benefit ? Does this translate into clinical benefit

8
Most impressive in high-risk patients undergoing major surgery Most impressive in high-risk patients undergoing major surgery Decrease blood loss and transfusion requirement Decrease blood loss and transfusion requirement Decrease thromboembolic complications Decrease thromboembolic complications Decrease pneumonia and resp depression Decrease pneumonia and resp depression Decrease MI and ARF Decrease MI and ARF Decrease mortality Decrease mortality

9
Risks Failure Failure Dural Tap Dural Tap Catheter migration subdurally Catheter migration subdurally Nerve damage Nerve damage Epidural abscess Epidural abscess Epidural Haematoma Epidural Haematoma

10
Haematoma Rare but potentially catastrophic Rare but potentially catastrophic Tryba (1993) – 1:150,000 epidural anaesthetics, 1:220,000 spinals (review 1.5 million patients) Risk probably higher if on drugs altering coagulation Tryba (1993) – 1:150,000 epidural anaesthetics, 1:220,000 spinals (review 1.5 million patients) Risk probably higher if on drugs altering coagulation Vandermeulen (1994) review for case reports of haematoma Vandermeulen (1994) review for case reports of haematoma 75% associated with epidural, 25% spinal 75% associated with epidural, 25% spinal 87% coagulation abnormalities/technical difficulties 87% coagulation abnormalities/technical difficulties Coag abnormalities include alcohol abuse, CRF, thrombocytopaenia as well as drugs Coag abnormalities include alcohol abuse, CRF, thrombocytopaenia as well as drugs
 – 1:150,000 epidural anaesthetics, 1:220,000 spinals (review 1.5 million patients) Risk probably higher if on drugs altering coagulation Tryba (1993) – 1:150,000 epidural anaesthetics, 1:220,000 spinals (review 1.5 million patients) Risk probably higher if on drugs altering coagulation Vandermeulen (1994) review for case reports of haematoma Vandermeulen (1994) review for case reports of haematoma 75% associated with epidural, 25% spinal 75% associated with epidural, 25% spinal 87% coagulation abnormalities/technical difficulties 87% coagulation abnormalities/technical difficulties Coag abnormalities include alcohol abuse, CRF, thrombocytopaenia as well as drugs Coag abnormalities include alcohol abuse, CRF, thrombocytopaenia as well as drugs")
13
Symptoms Sharp back pain Sharp back pain New motor/sensory loss New motor/sensory loss Urinary retention Urinary retention Variable and may be confused with effect of LA Variable and may be confused with effect of LA Paraplegia Paraplegia Need surgery within 8 hrs to get good or partial recovery. Need surgery within 8 hrs to get good or partial recovery.

14
Putting the two together? 1993 LMWH in USA b.d unlike in Europe o.d –sudden increase in reports of haematoma. 1993 LMWH in USA b.d unlike in Europe o.d –sudden increase in reports of haematoma. American Society of Regional anaesthesia and Pain Medicine – Consensus Statement,2002 American Society of Regional anaesthesia and Pain Medicine – Consensus Statement,2002 German Society of Anaesthesia and Intensive Care Medicine 2004 German Society of Anaesthesia and Intensive Care Medicine 2004

15
Unfractionated heparin Vascular or cardiac cases Vascular or cardiac cases Avoid if other coagulopathy Avoid if other coagulopathy Heparin delayed for 1hour after needle placement Heparin delayed for 1hour after needle placement Catheter removal 2-4 hr after last heparin Catheter removal 2-4 hr after last heparin Post-op monitoring for at least 48 hrs Post-op monitoring for at least 48 hrs

16
Cardiac Does the benefit outweigh the risk? Does the benefit outweigh the risk? Can show less troponin release Can show less troponin release Consistent decrease in ventilator time Consistent decrease in ventilator time Better analgesia on day 1 Better analgesia on day 1 ?fewer pulmonary complications ?fewer pulmonary complications No consistent improvement in arrythmia/cardiac/renal/neurologic outcome No consistent improvement in arrythmia/cardiac/renal/neurologic outcome No effect on mortality No effect on mortality

17
Recent case reports of haematomas Recent case reports of haematomas Can achieve other benefits with beta blockers/multimodal analgesic techniques Can achieve other benefits with beta blockers/multimodal analgesic techniques ?only in high risk COPD patients or those elderly at high risk of confusion ?only in high risk COPD patients or those elderly at high risk of confusion

18
LMWH Dose dependent antithrombotic effect by anti-Xa inhibition Dose dependent antithrombotic effect by anti-Xa inhibition Anti-Xa level not predictive of bleeding Anti-Xa level not predictive of bleeding Beware antiplatelet or oral anticoagulant Beware antiplatelet or oral anticoagulant Needle placement 10-12 hours after last dose LMWH Needle placement 10-12 hours after last dose LMWH Higher dose….wait 24hrs Higher dose….wait 24hrs

19
Post-op: Post-op: Catheter technique safe Catheter technique safe B.D dosing; remove catheter beforehand. Wait 2hrs after catheter removal before first dose B.D dosing; remove catheter beforehand. Wait 2hrs after catheter removal before first dose O.D. can have indwelling catheter. Remove minimum of 10-12 hours after last dose. Subsequent dose minimum 2hrs later O.D. can have indwelling catheter. Remove minimum of 10-12 hours after last dose. Subsequent dose minimum 2hrs later

20
Oral anticoagulants Stop 4-5 days before Stop 4-5 days before PT/INR within normal limits PT/INR within normal limits If on low dose post-op need to monitor INR daily If on low dose post-op need to monitor INR daily Catheter removal when INR<1.5 Catheter removal when INR<1.5

21
Antiplatelet medications Include: aspirin, NSAIDs, thienopyridine derivatives (ticlodipine/clopidogrel), GP IIb/IIIa antagonists (abciximab/tirofiban) Include: aspirin, NSAIDs, thienopyridine derivatives (ticlodipine/clopidogrel), GP IIb/IIIa antagonists (abciximab/tirofiban) GPIIb/IIIa in acute coronary syndrome….unlikely to be heading for surgery where epidural needed GPIIb/IIIa in acute coronary syndrome….unlikely to be heading for surgery where epidural needed No wholly accepted test to guide antiplatelet therapy No wholly accepted test to guide antiplatelet therapy CLASP study in obstetric patients – aspirin alone does not increase risk CLASP study in obstetric patients – aspirin alone does not increase risk NSAID alone no increased risk NSAID alone no increased risk
, GP IIb/IIIa antagonists (abciximab/tirofiban) Include: aspirin, NSAIDs, thienopyridine derivatives (ticlodipine/clopidogrel), GP IIb/IIIa antagonists (abciximab/tirofiban) GPIIb/IIIa in acute coronary syndrome….unlikely to be heading for surgery where epidural needed GPIIb/IIIa in acute coronary syndrome….unlikely to be heading for surgery where epidural needed No wholly accepted test to guide antiplatelet therapy No wholly accepted test to guide antiplatelet therapy CLASP study in obstetric patients – aspirin alone does not increase risk CLASP study in obstetric patients – aspirin alone does not increase risk NSAID alone no increased risk NSAID alone no increased risk")
22
Actual risk of haematoma with clopidogrel etc unknown. Actual risk of haematoma with clopidogrel etc unknown. Based on half-lives etc… Based on half-lives etc… Stop ticlodipine 14 days, clopidogrel 7 days Stop ticlodipine 14 days, clopidogrel 7 days GPIIb/IIIa contraindicated with 4 weeks GPIIb/IIIa contraindicated with 4 weeks Beware concurrent medications Beware concurrent medications

23
Little evidence increased surgical bleeding in non-cardiac studies Little evidence increased surgical bleeding in non-cardiac studies ? Stop only to make epidural safer (continue aspirin) ? Stop only to make epidural safer (continue aspirin) Usually on aspirin + clopidogrel because of intracoronary stent Usually on aspirin + clopidogrel because of intracoronary stent
 . Stop only to make epidural safer (continue aspirin) Usually on aspirin + clopidogrel because of intracoronary stent Usually on aspirin + clopidogrel because of intracoronary stent.")
24
Drug eluting stents Stop intimal hyperplasia which leads to early occlusion Stop intimal hyperplasia which leads to early occlusion Delay epithelialisation – hence need long term antiplatelet Rx Delay epithelialisation – hence need long term antiplatelet Rx Stopping antiplatelet Rx before surgery may increase risk of infarct (combine hypercoagulable state+ poorly endothelialised stent) Stopping antiplatelet Rx before surgery may increase risk of infarct (combine hypercoagulable state+ poorly endothelialised stent) Weigh benefit of epidural (and less surgical bleeding) v ischaemia/infarct Weigh benefit of epidural (and less surgical bleeding) v ischaemia/infarct ? Combine the two ? After platelet function ? Combine the two ? After platelet function

25
? Platelet function monitoring Spectrum of response to Rx Spectrum of response to Rx Can we identify which patients are higher risk? Can we identify which patients are higher risk? Bleeding time Bleeding time Optical light transmission aggregometry Optical light transmission aggregometry Platelet function analyser Platelet function analyser Modified TEG (Agarwal; Anaesthesiology 2006) Modified TEG (Agarwal; Anaesthesiology 2006)
 Modified TEG (Agarwal; Anaesthesiology 2006).")
26
Anti Xa fondaparinux Synthetic pentasaccharide, pure anti Xa Synthetic pentasaccharide, pure anti Xa 15hr half life 15hr half life Less venous thromboembolic events than with LMWH in orthopaedic patients Less venous thromboembolic events than with LMWH in orthopaedic patients Increased bleeding Increased bleeding Administered post-op (6hrs) Administered post-op (6hrs) No studies with indwelling epidural catheters No studies with indwelling epidural catheters Haematoma risk unclear Haematoma risk unclear
 Administered post-op (6hrs) No studies with indwelling epidural catheters No studies with indwelling epidural catheters Haematoma risk unclear Haematoma risk unclear")
27
Thrombin inhibitors Recombinant hirudin dreivatives. Recombinant hirudin dreivatives. Inhibit free and clot bound thrombin Inhibit free and clot bound thrombin Argatobatran (L arginine derivative) similar action Argatobatran (L arginine derivative) similar action No case reports spinal haematoma No case reports spinal haematoma Reports of spontaneous intracerebral bleed Reports of spontaneous intracerebral bleed No risk assessment statement given! No risk assessment statement given!
 similar action Argatobatran (L arginine derivative) similar action No case reports spinal haematoma No case reports spinal haematoma Reports of spontaneous intracerebral bleed Reports of spontaneous intracerebral bleed No risk assessment statement given. No risk assessment statement given!.")
28
For each individual patient a clear drug history is needed, an assessment of medical and surgical risk for their procedure, and an assessment of the additional benefit of a regional anaesthetic technique versus the risk of an epidural haematoma. In every patient undergoing a regional technique, rigorous post-op neurological monitoring is essential.

29
Questions?

Similar presentations


 of these drugs should be the one(s) I use, and for what?>")
 KSMC 8 May 2012. TURP gold standard in BPH Using of A-Cog & A-Plt is increasing. 4% on A-Cog 37% on A-plt.>")















