Download presentation
Presentation is loading. Please wait.

1
A Risk-Benefit Analysis of the use of NSAIDs in the Management of Arthritis Anne-Barbara Mongey, MD, DCH, MRCPI Associate Professor of Internal Medicine University of Cincinnati

2
Risk of GI Complications and Death With Nonspecific NSAIDs GI Ulcers/Bleeding/Perforation (FDA Data) : 1% patients ≥ 6 months of NSAID use 2-4% patients ≥ I year of NSAID use 103,000 hospitalizations and 16,500 deaths annually related to nonspecific NSAID use (Wolfe et al. N Engl J Med 1999)
.")
3
GI Risks of NS-NSAIDs With at least 2 months of NSAID or ASA treatment :- 1 in 5 patients will have an ulcer verified by EGD 1 in 70 patients will have a symptomatic ulcer 1 in 150 patients will have a bleeding ulcer 1 in 1200 patients will die of a bleeding ulcer Tramer et al. Pain. 2000;85:169-182.

4
Odds Ratio (OR) of Subjects Taking Analgesics Developing UGI Bleeding* CI=confidence interval. *Analysis involved subjects with upper and lower GI bleeding. Blot et al. J Epidemiol Biostat. 2000;5:137-142. Analgesic (Prescription and OTC) % Cases (n=627) % Controls (n=590) OR 95% CI Over-the-counter (OTC) ASA ASA 27 27 12 122.71.9-3.8 Ibuprofen Ibuprofen10.1 5.8 5.82.41.5-3.9 Acetaminophen Acetaminophen 4.5 4.5 6.3 6.30.90.5-1.6 Total OTC NSAIDs 36.217.5 32.2-4.1 Rx NS-NSAIDs 9.3 9.3 5.9 5.92.11.2-3.4 Total NSAIDs 42.9 22 223.12.3-4.1
 % Cases (n=627) % Controls (n=590) OR 95% CI Over-the-counter (OTC) ASA ASA Ibuprofen Ibuprofen Acetaminophen Acetaminophen Total OTC NSAIDs Rx NS-NSAIDs Total NSAIDs")
5
Without symptoms With symptoms Majority of Nonselective NSAID-Related GI Complications Are Asymptomatic Armstrong CP, Blower AL. Gut. 1987;28:527-532. Singh G et al. Arch Intern Med. 1996;156:1530-1536

6
Introduction of COX-2–Specific Inhibitors CH 3 F3CF3C N N S O O NH 2 S CH 3 O O O O Celecoxib Rofecoxib Valdecoxib N O Sulfone-based Sulfonamide-based S O O NH 2

7
Study Design: CLASS Trial vs VIGOR Trial CLASS Trial OA and RA patients Allowed aspirin use Minimum duration: 6 months Celecoxib 400mgs BID Comparators: Ibuprofen 800 mg TID Ibuprofen 800 mg TID Diclofenac 75 mg BID Diclofenac 75 mg BID VIGOR Trial RA patients No aspirin allowed Minimum duration: 6 months Rofecoxib 50mgs qd Comparator: Naproxen 500 mg BID Naproxen 500 mg BID

8
Silverstein FE et al. JAMA. 2000;284:1247-1255. Annualized incidence (%) (per No. of patient-years) 0 1 2 3 4 Upper GI ulcer complications Complications and symptomatic ulcers P=.09 P=.02 0.76% 1.45% 2.08% 3.54% CLASS: UGI Ulcer Complications and Symptomatic Ulcers at 6 Months—All Patients Nonspecific NSAIDs* (n=3981) Celecoxib 400 mg BID (n=3987)
 Upper GI ulcer complications Complications and symptomatic ulcers P=.09 P= % 1.45% 2.08% 3.54% CLASS: UGI Ulcer Complications and Symptomatic Ulcers at 6 Months—All Patients Nonspecific NSAIDs* (n=3981) Celecoxib 400 mg BID (n=3987).")
9
0 1 2 3 4 P=.04 P=.02 0.44% 1.27% 1.40% 2.91% CLASS: Ulcer Complications and Symptomatic Ulcers at 6 Months—Nonusers of ASA Nonspecific NSAIDs (n=3981) Celecoxib 400 mg BID (n=3987) Upper GI ulcer complications Complications and symptomatic ulcers Annualized incidence (%) (per No. of patient-years) Silverstein FE et al. JAMA. 2000;284:1247-1255.
 Silverstein FE et al. JAMA. 2000;284:")
11
SUCCESS=Successive Celecoxib Efficacy and Safety Study in OA. *Celecoxib 200 mg/day or 400 mg/day; † Diclofenac 50 mg BID or naproxen 500 mg BID. Singh G et al. Presented at: EULAR; June 13-16, 2001; Prague, Czech Republic. SUCCESS-1: UGI Ulcer Complications and Symptomatic Ulcers 0.1 0.8 1.0 2.1 0 1 2 3 4 Ulcer complicationsComplications and symptomatic ulcers RRR=87.5% P<.05 RRR=51.5% P<.05 Annualized rate (events per 100 patient-years) Nonspecific NSAIDs † (n=4394) Celecoxib* (n=8800)
 Nonspecific NSAIDs † (n=4394) Celecoxib* (n=8800).")
12
GI Healthcare Resource Utilization SUCCESS-1 –100 –80 –60 –40 –20 0 Physician visits Specialist visits GI hospitalizations ICU hospitalizations Blood transfusions *Celecoxib 200 mg/day or 400 mg/day; † Diclofenac 50 mg BID or naproxen 500 mg BID. Goldstein JL et al. Arthritis Rheum. 2001;44:S136. Abstract 503. 75% 52% 86% 34% 45% Fewer events Celecoxib* vs Pooled Comparator NSAIDs † Visits for upper GI complications %

13
Upper GI Safety of COX-2 specific Inhibitor & Nonspecific NSAIDs An Ontario, Canada, population-based, retrospective cohort study: - Celecoxib (n=18,908) - Rofecoxib (n=14,583) - Nonspecific NSAIDs (n=5391) - Diclofenac + misoprostol (n=5087) - Control (NSAID-naïve; n=100,000) Patients 66 years of age Main outcome measure: Rate of hospitalization for upper GI hemorrhage Mamdani M et al. BMJ. 2002;325:624-627.

14
Adjusted Hazard Estimates for Hospitalization for UGI Hemorrhage Among Elderly Patients Using Prescribed NSAIDs Patients Hospitalized (%) 0.35 0.30 0.25 0.20 0.15 0.10 0.05 0.00 060120180240295 Time From index Date (days) Nonselective NSAIDs4.0 (2.3 to 6.9) Diclofenac + misoprostol3.0 (1.7 to 5.6) Rofecoxib1.9 (1.3 to 2.8) Celecoxib1.0 (0.7 to 1.6) Controls1.0 Rate ratio (95% CI) Mamdani et al. BMJ. 2002;325:624-627.

15
Celecoxib vs Diclofenac + Omeprazole in Reducing the Risk of Recurrent Bleeding Ulcer in Patients with Arthritis Design Prospective, double-blind randomized control trial comparing celecoxib 200mgs BID with diclofenac 75mgs BID plus omeprazole 20mgs qd Patient Population: Patients with arthritis who presented with ulcer bleeding confirmed by EGD Outcome: Recurrence of a bleeding ulcer Chan et al. N Engl J Med. 2002;347:2104-2110.

16
Probability of Recurrent Bleeding Ulcer in 6 Months Celecoxib 4.9% (3.1-6.7) Celecoxib 4.9% (3.1-6.7) Omeprazole + Diclofenac 6.4% (4.3-8.4) Celecoxib 4.5% (2.7-6.3) Omeprazole + Diclofenac 5.6% (3.6-7.7) Without concomitant ASA All patients Percent (95% CI) 0246810
 Celecoxib 4.9% ( ) Omeprazole + Diclofenac 6.4% ( ) Celecoxib 4.5% ( ) Omeprazole + Diclofenac 5.6% ( ) Without concomitant ASA All patients Percent (95% CI)")
17
Therapeutic Arthritis Research and Gastrointestinal Event Trial (TARGET) Randomization Screening Randomization Baseline Week 52 Week 56 Final visit Follow-up Ibuprofen 800 mg tid n=4415 n=4399 Lumiracoxib400 mg qd Lumiracoxib 400 mg qd Naproxen 500 mg bid n=4754 n=4757 Lumiracoxib 400 mg qd
 Randomization Screening Randomization Baseline Week 52 Week 56 Final visit Follow-up Ibuprofen 800 mg tid n=4415 n=4399 Lumiracoxib400 mg qd Lumiracoxib 400 mg qd Naproxen 500 mg bid n=4754 n=4757 Lumiracoxib 400 mg qd")
18
Therapeutic Arthritis Research and Gastrointestinal Event Trial (TARGET) 52 week study of 18,325 Patients, aged ≥ 50 years, randomized for low-dose ASA use and age: 9,156 Lumiracoxib 400 mgs qd 4,754 Naproxen 500 mgs BID 4,415 Ibuprofen 800 mgs TID Primary end point: difference in time-to-event distribution of upper GI ulcer complications Incidence of ulcer complications among non ASA users: NSAIDS: 1.09% (64 events) Lumiracoxib: 0.25% (14 events) * p<0.0001
 52 week study of 18,325 Patients, aged ≥ 50 years, randomized for low-dose ASA use and age: 9,156 Lumiracoxib 400 mgs qd 4,754 Naproxen 500 mgs BID 4,415 Ibuprofen 800 mgs TID Primary end point: difference in time-to-event distribution of upper GI ulcer complications Incidence of ulcer complications among non ASA users: NSAIDS: 1.09% (64 events) Lumiracoxib: 0.25% (14 events) * p<0.0001")
19
Risk Factors for NSAID Induced GI Adverse Events The National Institute for Clinical Excellence Age > 65 years History of Peptic Ulcer Disease History of GI Bleed Concomitant Anticoagulant Usage Concomitant Steroid Usage High Dose NSAID Usage Comorbid Medical Conditions Available at: http://www.nice.org.uk//. Accessed September 22, 2005.

20
Utilization of Gastroprotective Strategies by Presence of GI Risk Factors Among New NSAID Users Sturkenboom et al. Rheumatology. 2003;42(suppl 3):iii23-iii31. ≥2 Risk Factors 1 Risk Factor 86.6%81.2% 0.1%2.5%10.8%0.2%4.0%14.7% Coxib alone NSAID+GPA Coxib+GPA No gastroprotection
:iii23-iii31. ≥2 Risk Factors 1 Risk Factor 86.6%81.2% 0.1%2.5%10.8%0.2%4.0%14.7% Coxib alone NSAID+GPA Coxib+GPA No gastroprotection.")
21
Cardiovascular Thromboembolic Data: Coronary Artery Disease

22
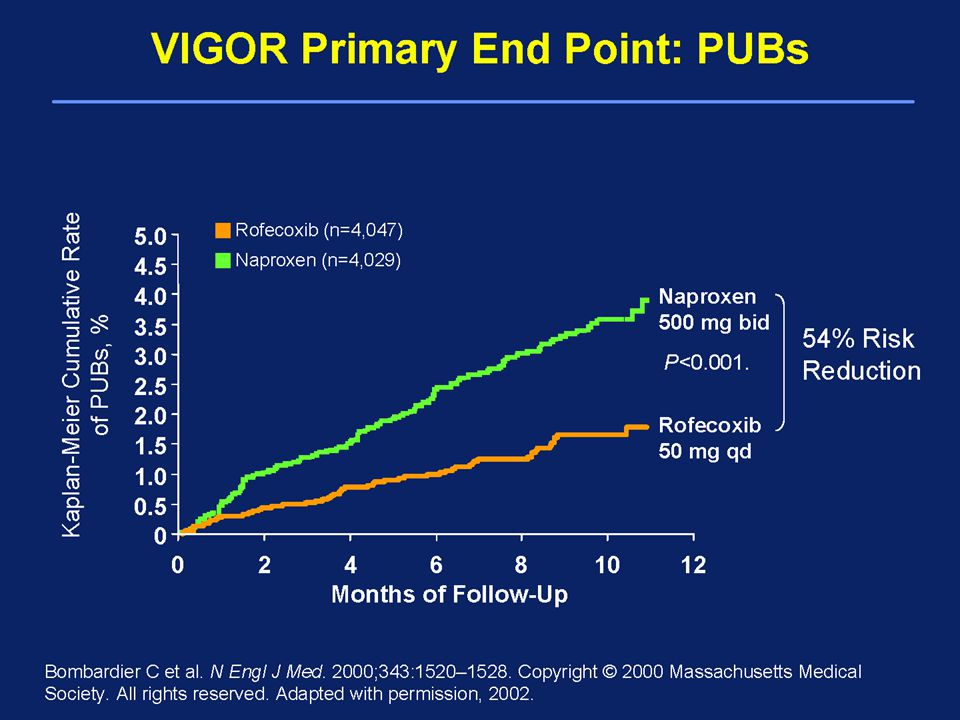
Serious Thromboembolic CV Adverse Events in ASA Nonusers Days 04080120160200240280320360 0.0 0.5 1.0 1.5 2.02.5 P <.05 Rofecoxib 50 mg (n=4047) Naproxen 500 mg bid (n=4029) RR=2.38 Incidence of Thromboembolic SAEs (%) Mukherjee et al. JAMA. 2001;286:954-959. VIGOR

23
CLASS: Thromboembolic CV AEs ASA Nonusers ASA Users* P=.899 P=.947 0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.55.04.0 04080120160200240280320360 Days Celecoxib 400 mg bid (n=3105) NS-NSAIDs (n=3124) Celecoxib 400 mg bid (n=882) NS-NSAIDs (n=857) Patients (%) 04080120160200240280320360Days 0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.55.04.0 White et al. Am J Cardiol. 2002;89:425-430. Data on file. Pfizer Inc., New York, NY; FDA Advisory Committee Briefing Document. Available at: http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4090B1_03_Pfizer-Celebrex-Bextra.pdf. Accessed January 12, 2005.

24
COX-2–Specific Inhibitors, Nonselective NSAIDs, and Risk of Serious CHD Design Retrospective observational study of Tennessee Medicaid data Matched for age, sex, and date NSAID use began Patient Population 202,916 nonusers (patients who had not used an NSAID within 365 days of enrollment) and 251,046 NSAID current users Patients aged 50-84 years without noncardiovascular life-threatening illnesses Outcome Serious CHD, defined as hospital admission for AMI or death from CHD, in patients taking rofecoxib, celecoxib, ibuprofen, and naproxen Ray WA et al. Lancet. 2002;360:1071-1073.

25
COX-2–Specific Inhibitors, NS-NSAIDs, and Risk of Serious CHD † P = 0.024 vs reference; Ray WA et al. Lancet. 2002;360:1071-1073. 10 1 Better than nonuserWorse than nonuser 0.1 Reference: Nonusers IRR = 1.0 Celecoxib (n = 4509) 0.88 (0.67-1.16) Rofecoxib >25 mg/day (n = 500) 1.93 (1.09-3.43) † Naproxen (n = 6489) 0.92 (0.73-1.16) Ibuprofen (n = 4319) 1.01 (0.77-1.33) Rofecoxib 25 mg/day (n = 3430) 1.02 (0.76-1.37)
 0.88 ( ) Rofecoxib >25 mg/day (n = 500) 1.93 ( ) † Naproxen (n = 6489) 0.92 ( ) Ibuprofen (n = 4319) 1.01 ( ) Rofecoxib 25 mg/day (n = 3430) 1.02 ( ).")
26
Risk of CV Events for Rofecoxib, Celecoxib relative to Placebo & NSAIDs Design Population-based, retrospective cohort analysis of health records in Ontario, Canada Patient Population: Patients aged ≥66 years with a prescription for celecoxib, rofecoxib, naproxen or non-naproxen NSAIDs Control group was NSAID-naïve Outcome: Hospitalization for acute myocardial infarction (AMI) Mamdani et al. Arch Interrn Med 2003; 163: 481-486

27
Decreased IncidenceIncreased Incidence Risk of AMI with COX-2–Specific Inhibitors and NS-NSAIDs Compared With Nonusers 0.9 1.0 1.2 1.0 Mamdani et al. Arch Intern Med 2003; 163: 481-486 Celecoxib (n = 15,271) Rofecoxib (n = 12,156) Naproxen (n = 5669) Non-naproxen NSAIDs (n = 33,868) Nonusers (n = 100,000) 0.5 1.0 1.5 2.0
 Rofecoxib (n = 12,156) Naproxen (n = 5669) Non-naproxen NSAIDs (n = 33,868) Nonusers (n = 100,000)")
28
Risk for Myocardial Infarction in NSAID and Coxib Users ≥ 65 Years Observational, matched case-control, population-based study: - 54,475 patients 65 years of age -received their medications through 2 state- sponsored pharmaceutical benefits program -matched for age, gender, and month of index date Main outcome measure: Relative risk of acute myocardial infarction Solomon et al. Circulation. 2004;109:2068-2073

29
Relative risk of AMI With COX-2–Specific Inhibitors † p<0.05. Solomon et al. Circulation. 2004;109:2068-2073 Decreased Incidence Rofecoxib all doses (vs no NSAID users) Increased Incidence Celecoxib all doses (vs no NSAID users) Current Users Rofecoxib >25mg (vs no NSAID users) Rofecoxib <25mg (vs no NSAID users) Rofecoxib all doses (vs celecoxib all doses ) Rofecoxib >25 mg (vs celecoxib >200 mg) Rofecoxib <25 mg (vs celecoxib <200 mg) 0.511.522.5 0.93 1.14 1.58 † 1.11 1.24 † 1.70 † 1.21 †
 Increased Incidence Celecoxib all doses (vs no NSAID users) Current Users Rofecoxib >25mg (vs no NSAID users) Rofecoxib <25mg (vs no NSAID users) Rofecoxib all doses (vs celecoxib all doses ) Rofecoxib >25 mg (vs celecoxib >200 mg) Rofecoxib <25 mg (vs celecoxib <200 mg) † † 1.70 † 1.21 †.")
30
Risk of Acute Cardiac Events among Patients treated with Coxibs & non-selective NSAIDs All patients, aged 18-84 years, who received at least one NSAID prescription between 1/99 - 12/01: Celecoxib (n= 40,405); Rofecoxib (n= 27,248) Ibuprofen (n= 991,261); Naproxen (n= 435,492) Nested Case Control study Matched with living controls for index date,age,gender,region Conditional logistic regression analysis Mean Age: 66.8 years; 61.8% were males No. of Acute Cardiac Events: 8,143 (6635 AMI; 1508 SCD) Graham et al. Lancet 2005; 365:475-481
 Graham et al. Lancet 2005; 365:")
31
Risk of AMI and SCD With Current Use of COX-2 Selective and NS-NSAIDs 0.0 0.5 1.0 1.5 2.0 2.5 3.03.5 Control (remote use) CelecoxibIbuprofenNaproxen Rofecoxib >25 mg Other NSAIDs IndomethacinDiclofenac Adjusted † Odds Ratio (95% CI) 1.00 (reference) 0.86 (0.69-1.07) 1.09 (0.99-1.21) 1.18 (1.04-1.35) 3.15 (1.14-8.75) 1.16 (1.04-1.30) 1.33 (1.09-1.63) 1.69 (0.97-2.93) P =.01 P <.01 P =.005 Rofecoxib 25 mg 1.29 (0.93-1.79) P <.01 P =.06 Adjusted for age, sex, health plan region, medical history, smoking, and medication use. Adapted from Graham et al. Lancet. 2005;365:475-481.

32
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 Adjusted * Odds Ratio Control (no use) 1.00 (reference) Naproxen 1.27 P =.04 Other ns-NSAIDs 1.21 P =.03 Other Selective NSAIDS 1.27 P =.046 Diclofenac 1.55 P <.001 Data for drugs prescribed within 3 months of the index date. * Adjusted for smoking, comorbidity, socioeconomic deprivation, ASA use, & comcomitant medication. Hippisley-Cox et al. BMJ. 2005. Observational Case-control Study Risk of MI among Patients receiving COX-2 Selective Inhibitors & ns-NSAIDs Celecoxib 1.21 P =.11 Rofecoxib 1.32 P =.005 Ibuprofen 1.24 P <.001 p value of.01 was prespecified as significant

33
Cox-2 inhibitors & non-selective NSAIDs increase the risk of AMI in patients with Arthritis: Selectivity is with the patients, not with the drug class Patients > 18 years with physician-diagnosed arthritis treated with a NSAID between 1/1/99 - 6/30/04 Nested case control study Cases of acute myocardial infarction were risk-set matched with 4 controls for age, gender and index date Analyses were adjusted for 38 confounding risk factors as well as concomitant aspirin treatment. Singh G et al. Abstract - EULAR 2005

34
Medi-Cal: NSAIDs and Risk for AMI 2,356,885 person-years of follow-up; 15,343 cases of AMI OR for AMI (95% CI) Singh et al. EULAR. 2005. 0.83 (0.60-1.14); P =.26 0.99 (0.72-1.37); P =.97 1.08 (0.95-1.22); P =.22 1.09 (1.02-1.15); P <.008 1.11 (1.01-1.22); P <.02 1.32 (1.22-1.42); P <.0001 1.37 (1.05-1.78); P <.02 1.41 (1.01-1.96); P <.04 1.71 (1.35-2.17); P <.0001 1.00 (reference) Nabumetone Valdecoxib Naproxen Celecoxib Ibuprofen Rofecoxib Meloxicam Sulindac Indomethacin Remote use
; P = ( ); P = ( ); P = ( ); P < ( ); P < ( ); P < ( ); P < ( ); P < ( ); P < (reference) Nabumetone Valdecoxib Naproxen Celecoxib Ibuprofen Rofecoxib Meloxicam Sulindac Indomethacin Remote use.")
35
APPROVe Study Multicenter, randomized, placebo-controlled, double-blinded 3 year study of Rofecoxib 25 mgs qd. (2/2000-11/2001) Primary End point: Recurrence of colorectal adenomas of the large bowel in patients with a history of colorectal adenomas Inclusion criteria: ≥ 1 adenomas; ≥ 40 years; Exclusion criteria: angina; CHF; uncontrolled HTN; MI, PTCA or CABG within 1 yr or CVA/TIA within 2 yrs of study entry Low dose ASA allowed in up to 20% Bresalier et al. N Engl J Med. 2005;352
 Primary End point: Recurrence of colorectal adenomas of the large bowel in patients with a history of colorectal adenomas Inclusion criteria: ≥ 1 adenomas; ≥ 40 years; Exclusion criteria: angina; CHF; uncontrolled HTN; MI, PTCA or CABG within 1 yr or CVA/TIA within 2 yrs of study entry Low dose ASA allowed in up to 20% Bresalier et al. N Engl J Med. 2005;352.")
36
APPROVe Study 2586 Patients: 62% male; mean age = 59 years; 72 confirmed thrombotic events: Rofecoxib (n=46) : 1.5 events/100 patient years Placebo (n=26) : 0.78 events/100 patient years Relative risk: 1.92 (95% CI 1.19, 3.11; p=0.008) 52 events by APTC criteria: Relative risk: 2.06 (95% CI 1.16, 3.64; p=0.008) Increased relative risk occurred after 18 months of therapy No difference in overall Mortality
 : 1.5 events/100 patient years Placebo (n=26) : 0.78 events/100 patient years Relative risk: 1.92 (95% CI 1.19, 3.11; p=0.008) 52 events by APTC criteria: Relative risk: 2.06 (95% CI 1.16, 3.64; p=0.008) Increased relative risk occurred after 18 months of therapy No difference in overall Mortality")
37
APPROVe: Cumulative Incidence of Confirmed Serious Thrombotic CV Events* Bresalier et al. N Engl J Med. 2005;352:1092-1102.061218243036 P =.008 Cumulative Incidence of Confirmed Thrombotic Events (%) 0 1 2 3 4 56Month Rofecoxib Placebo129911951156107910421001835 128711291057989938896727 No. at Risk Rofecoxib 25 mg qd 1.92 (1.19-3.11) Placebo * Fatal and nonfatal MI, unstable angina, sudden death due to cardiac causes, fatal and nonfatal ischemic stroke, transient ischemic attack, peripheral arterial thrombosis, peripheral venous thrombosis, and pulmonary embolism Bars represent 95% CI.
 Month Rofecoxib Placebo No. at Risk Rofecoxib 25 mg qd 1.92 ( ) Placebo * Fatal and nonfatal MI, unstable angina, sudden death due to cardiac causes, fatal and nonfatal ischemic stroke, transient ischemic attack, peripheral arterial thrombosis, peripheral venous thrombosis, and pulmonary embolism Bars represent 95% CI..")
38
Adenoma Prevention with Celecoxib (APC) Trial Prospective, randomized, placebo-controlled, double-blinded multicenter trial comparing the efficacy and safety of celecoxib Primary End point: Recurrence of adenomatous polyps of the large bowel in patients who had undergone polypectomy Participants: 2035 patients, aged 32-88 years Follow-up: 2.8-3.1 years Solomon et al. N Engl J Med. 2005;352-362.

39
Adenoma Prevention with Celecoxib (APC) Trial Solomon et al. N Engl J Med. 2005;352-362. Agentn/N % of patients Relative risk compared with placebo 95% confidence intervals Placebo6/6790.9%------ Celecoxib 200 mgs bid 15/6852.2%2.3*0.9-5.5 Celecoxib 400 mgs bid 20/6713.0%3.4*1.4-7.8 Average duration of treatment = 33 months * Statistically significant Fatal and nonfatal cardiovascular events

40
Celecoxib Colon Polyp Prevention Trials: Composite End Point (Death From CV Causes, MI, Stroke, or Heart Failure) 061218243036 0.000 0.010 0.020 0.030 0.0400.050 Estimated Probability of Cumulative Composite End Point P =.01 Solomon et al. N Engl J Med. 2005;352:1071-1080; Levin. February 17, 2005. Gaithersburg, Md. Adenoma Prevention with Celecoxib trial Months After First Dose Celecoxib 400 mg bid Celecoxib 200 mg bid Placebo679677675672668667585 685681676675673670595 671669665655651648576 No. at Risk Celecoxib 400 mg bid 3.4 (1-4-7.8) Placebo Celecoxib 200 mg bid 2.3 (0.9-5.5) 0.9% 2.2% 3.0%
 Placebo Celecoxib 200 mg bid 2.3 ( ) 0.9% 2.2% 3.0%.")
41
Prevention of Spontaneous Adenomatous Polyposis (PreSAP) Trial Agentn/N % of patients Relative risk compared with placebo 95% confidence interval Placebo12/6281.9%------ Celecoxib 400 mg qd 20/9332.1%1.10.6-2.3 Fatal and nonfatal cardiovascular events Average duration of treatment = 33 months Average duration of treatment = 33 months
 Trial Agentn/N % of patients Relative risk compared with placebo 95% confidence interval Placebo12/6281.9% Celecoxib 400 mg qd 20/9332.1% Fatal and nonfatal cardiovascular events Average duration of treatment = 33 months Average duration of treatment = 33 months")
42
Celecoxib Colon Polyp Prevention Trials: Composite End Point (Death From CV Causes, MI, Stroke, or Heart Failure) 061218243036 0.000 0.010 0.020 0.030 0.0400.050 Estimated Probability of Cumulative Composite End Point P =.10 Solomon et al. N Engl J Med. 2005;352:1071-1080; Levin. February 17, 2005. Gaithersburg, Md. Prevention of Spontaneous Adenomatous Polyps trial Months After First Dose Celecoxib 400 mg qd Placebo828823620618618453 929925923917914688 No. at Risk Celecoxib 400 mg qd 1.1 (0.6-2.3) Placebo 2.1% 1.9%
 Placebo 2.1% 1.9%.")
43
TARGET—Study Design Randomization Screening Randomization Baseline Week 52 Week 56 Final visit Follow-up Ibuprofen 800 mg tid n=4415 n=4399 Lumiracoxib400 mg qd Lumiracoxib 400 mg qd Naproxen 500 mg bid n=4754 n=4757 Lumiracoxib 400 mg qd TARGET=the Therapeutic Arthritis Research and Gastrointestinal Event Trial.

44
Therapeutic Arthritis Research and Gastrointestinal Event Trial (TARGET) Primary end point: APTC endpoint (MI, CVA, CV death) NSAIDS: 0.55% (50 events) Lumiracoxib: 0.65% (59 events) (p=0.5074) Myocardial Infarction: Lumiracoxib: 0.38% (18) vs Naproxen: 0.21% (10) Lumiracoxib: 0.11% (5) vs Ibuprofen: 0.16% (7)
 Primary end point: APTC endpoint (MI, CVA, CV death) NSAIDS: 0.55% (50 events) Lumiracoxib: 0.65% (59 events) (p=0.5074) Myocardial Infarction: Lumiracoxib: 0.38% (18) vs Naproxen: 0.21% (10) Lumiracoxib: 0.11% (5) vs Ibuprofen: 0.16% (7)")
45
Lumiracoxib: APTC End Point in the Overall Population *Log-rank test for treatment group comparison based on a stratified test with the strata sub-study and low-dose ASA use. APTC=Antiplatelet Trialists’ Collaboration. Farkouh et al. Lancet. 2004;364:675-684. 0 1.0 60 Cumulative Incidence Rate (%) 0120180240360 Study Day Lumiracoxib 0.6 300420 0.8 0.4 NSAIDs 0.2 Kaplan-Meier Estimates
 Study Day Lumiracoxib NSAIDs 0.2 Kaplan-Meier Estimates.")
46
Does the use of NSAIDs affect the cardioprotective effect of Aspirin?

47
Effect of NSAIDs on the Anti-Platelet Effects of Aspirin Catella-Lawson et al. N Engl J Med 2001; 345:1809-1817

48
Pharmacodynamic Interaction of Naproxen with Low-Dose ASA Naproxen reversibly and competitively inhibited COX-1 This inhibition could be overcome by increasing concentrations of arachidonic acid Pretreatment of platelets with naproxen prevented inhibition of COX-1 by ASA Concurrent administration of a single dose of Naproxen with ASA prevented inhibition of platelet aggregration Chronic administration of Naproxen and ASA resulted in similar inhibition of TXB2 production and platelet aggregation Capone et al. J Am Coll Cardiol. 2005;45:1295-1301.

49
Effect of Nonselective NSAID Use on Aspirin Cardioprotection Subgroup analysis from the 5-year prospective Physician’s Health Study comparing ASA 325 mgs to placebo 22,071 male physicians, aged 40-84 years 378 MIs: 139 ASA group; 239 Placebo Kurth et al. Circulation 2003; 108: 1191-95. Kurth et al. Circulation 2003; 108: 1191-95.

50
Relative Risk (RR) of MI according to ASA use and time-varying NSAID use Medication MI (n) Age-adjusted RR (95% CI) Aspirin 1071.0 + 1-59 days/yr NSAIDs 261.21 (0.76-1.87) + ≥ 60 days/yr NSAIDs 62.86 (1.25-6.56)* Placebo1931.00 + 1-59 days/yr NSAIDs 441.14 (0.81-1.60) ≥ 60 days/yr NSAIDs 60.21 (0.03-1.48) * Positive association Kurth et al. Circulation 2003; 108: 1191-95

51
Relative Risk of MI in Men Taking ASA + Intermittent or Regular NSAID Use Drug Relative Risk of MI 95% CI Placebo alone 1.00NA ASA alone 0.560.44-0.72 ASA plus “intermittent” NSAID use 0.690.46-1.05 ASA plus “regular” NSAID use 1.570.70-3.56 Kurth et al. Circulation. 2003;108:1191-1195.

52
Effect of Ibuprofen on Cardioprotective Effect of Aspirin Participants - patients who took ASA < 325 mgs/day and survived ≥ I month after D/C with CVD (n=7107). Groups: 1. ASA alone (n=6285) 2. ASA + Ibuprofen (mean = 1210 mg/d) (n=187) 3. ASA + Diclofenac (mean = 117 mgs/d) (n=206) 4. ASA + other NSAID (n=429) Cox’s regression models with time-dependent variables MacDonald TM and Wei L. Lancet 2003; 361:573-4
 2. ASA + Ibuprofen (mean = 1210 mg/d) (n=187) 3. ASA + Diclofenac (mean = 117 mgs/d) (n=206) 4. ASA + other NSAID (n=429) Cox’s regression models with time-dependent variables MacDonald TM and Wei L. Lancet 2003; 361:")
53
Mortality from CARDIOVASCULAR causes Group Number of deaths Mortality rate/ 1000 person-yrs Hazard ratio p value Aspirin alone (n=6285) 1350 1350 58.5 58.5 1.00 1.00- Aspirin + ibuprofen (n=187) 39 39 61.6 61.6 1.73 1.730.0305* Aspirin + diclofenac (n=206) 44 44 62.0 62.0 0.80 0.800.3749 Aspirin + other NSAIDs (n=429) 114 114 70.0 70.0 1.03 1.030.8337 MacDonald TM and Wei L. Lancet 2003; 361:573-4

54
FDA boxed warning for the potential of increased risk of CV events and GI bleeding associated with all prescription NSAIDs, including Celebrex. For all prescription NSAIDs, FDA has requested a contraindication for use in patients who have recently undergone CABG surgery. In light of the increased CV risk for all prescription NSAIDs, as well as the increased reporting rate of rare skin reactions with Bextra, the FDA requested Bextra’s withdrawal from the market. OTC manufacturers asked to include potential CV, GI and skin reaction risks in their labels April 7,2005: FDA Announcement

55
ANKYLOSING SPONDYLITIS

57
TREATMENT OF ANKYLOSING SPONDYLITIS NSAIDs Physical Therapy Sulfasalazine TNF Inhibitors

58
Celecoxib for Ankylosing Spondylitis Randomized, double-blind, placebo-controlled study of Celecoxib 200mgs qd and 400mgs qd. Randomized, active- (NSAID), placebo-controlled multicenter, 6-week study of Celecoxib 100mgs BID and Ketoprofen 100mgs BID.
, placebo-controlled multicenter, 6-week study of Celecoxib 100mgs BID and Ketoprofen 100mgs BID..")
59
Celecoxib Versus Ketoprofen in AS Celecoxib Versus Ketoprofen in AS Pain IntensityFunctional Impairment Mean Improvement in Patient-Reported Global Pain 30 25 20 15 10 5 0 13 27 21 Mean Improvement in BASFI 12 10 8 6 4 2 0 12 6 Celecoxib 100 mg bid (n=80) Placebo (n=76) Ketoprofen 100 mg bid (n=90) Dougados et al. Arthritis Rheum. 2001. P =.007 P =.001 P =.051 P =.043 -2

60
Celecoxib Versus Naproxen in AS Pain Intensity * Functional Impairment * Mean Improvement in Patients’ Assessment of Global Pain Intensity 40 35 25 20 15 5 0 9.9 30.0 36.3 30.4 30 10 30 35 20 15 5 0 4.0 21.1 27.9 † 22.5 10 16 12 10 6 0 -2 -3.3 8.5 15.8 ‡ 12.1 4 14 8 2 -4 Celecoxib 200 mg qd (n=137) Placebo (n=156) Naproxen 500 mg bid (n=157) Celecoxib 400 mg qd (n=161) Disease Activity * Mean Improvement in Patients’ Global Assessment of Disease Activity Mean Improvement in BASFI * P <.001 for all active treatments vs placebo † P <.05 vs celecoxib 200 mg qd ‡ P <.01 vs celecoxib 200 mg qd
 Placebo (n=156) Naproxen 500 mg bid (n=157) Celecoxib 400 mg qd (n=161) Disease Activity * Mean Improvement in Patients’ Global Assessment of Disease Activity Mean Improvement in BASFI * P <.001 for all active treatments vs placebo † P <.05 vs celecoxib 200 mg qd ‡ P <.01 vs celecoxib 200 mg qd")
61
Celecoxib Versus Naproxen in AS : Safety Analyses Celecoxib 200 mg qd (n=137) Placebo (n=156) Naproxen (n=157) Celecoxib 400 mg qd (n=161) 1 AE Withdrawal due to AE 1 SAE Data on file.
 Placebo (n=156) Naproxen (n=157) Celecoxib 400 mg qd (n=161) 1 AE Withdrawal due to AE 1 SAE Data on file.")
62
THANK YOU

Similar presentations


>")








 The LIPID Study Group N Engl J Med 1998;339:1349-57.>")






>")

