Download presentation
Presentation is loading. Please wait.

1
Neoplasms of Lung and Pleura William K. Funkhouser, M.D. Ph.D. –x 3-1069 –Bill_Funkhouser@med.unc.edu

2
Neoplasms of Lung and Pleura Primary Neoplasms of Lung Primary Neoplasms of Pleura Metastatic Neoplasms to Lung and/or Pleura

3
Neoplasms of Lung and Pleura: Classification by Lineage Epithelial – most common Melanocytic Stromal Mesothelial

4
Benign Lung Neoplasms Hamartoma Squamous papillomatosis Pleomorphic adenoma (ENT)
")
5
Hamartoma Clin: Adolescence adulthood None in newborns - not congenital Rad: Solitary nodule +/- popcorn calcification Peripheral > central Path: Gross: solitary, lobulated, cartilagenous Micro: normal tissues in excess/disarray

6
Hamartoma Solitary Pulmonary Nodule

7
Bivalved Hamartoma

8
Cartilage in excess and disarray

9
Malignant epithelial neoplasms (Carcinomas) Squamous cell carcinoma Adenocarcinoma Large cell undifferentiated carcinoma Small cell undifferentiated carcinoma
 Squamous cell carcinoma Adenocarcinoma Large cell undifferentiated carcinoma Small cell undifferentiated carcinoma")
12
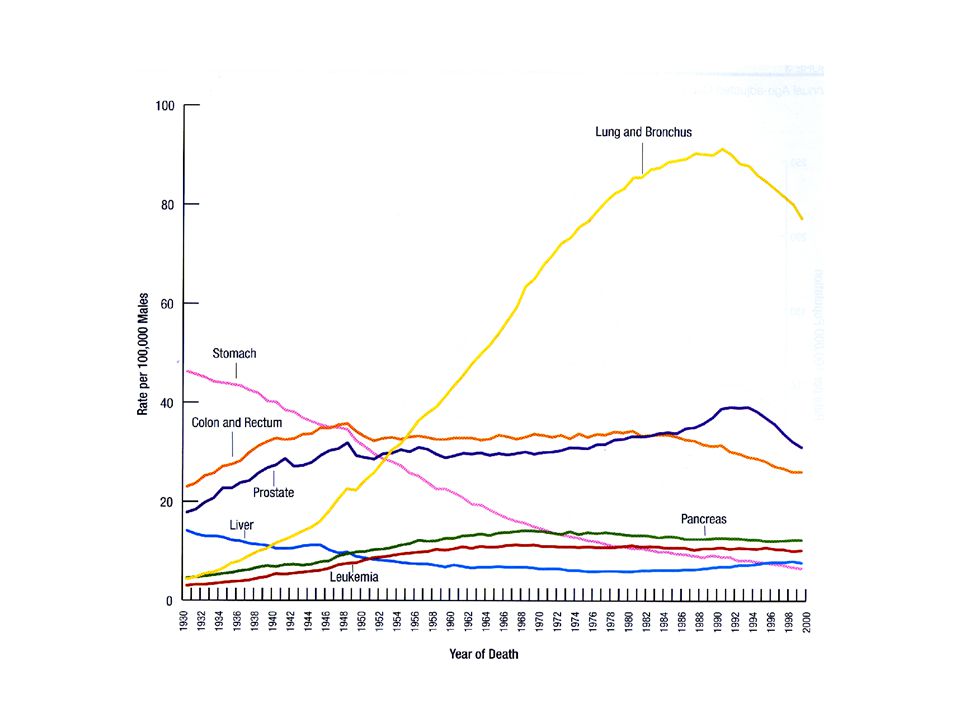
Lung Carcinomas: Epidemiology Estimated Incidence (2003): 172,000 (US) Estimated Mortality (2003): 157,000 (US) >85% of lung carcinoma deaths (and 30% of all cancer deaths) occur in cigarette smokers Risk = f(# cigarettes smoked), 15-30X in heavy smokers, 50-60X in asbestos workers who smoke Risk decreases with cessation of cigarette smoking: baseline after 15 years
: 172,000 (US) Estimated Mortality (2003): 157,000 (US) >85% of lung carcinoma deaths (and 30% of all cancer deaths) occur in cigarette smokers Risk = f(# cigarettes smoked), 15-30X in heavy smokers, 50-60X in asbestos workers who smoke Risk decreases with cessation of cigarette smoking: baseline after 15 years")
13
USA Tobacco Use 25% of US adults smoke cigarettes M=F US adults consume 2,400 cigs/person/year 36% of US high school students smoke est. 1.8 million new smokers/year (65% < 18 yo)
.")
14
Tobacco: Morbidity and Mortality Premature ASVD: major risk factor Emphysema: Linear with exposure: 7%/10 years Chronic bronchitis Carcinomas of pharynx, larynx, lung, esophagus, bladder, kidney Fetal tobacco syndrome

15
Tobacco: Chemistry 80% air, 20% gases and particulates Gases: CO, CO 2, formaldehyde, acrolein, methanol, phenol, anthracenes, pyrenes Nicotine: 1% of smoke 85% absorbed in lung equivalent to 1 mg IV

16
Tobacco: Chemistry Particulates: –resin cores in 0.5 M diameter water droplets –est. 10 9 particles/ml –50% deposited in and cleared by cilia – remainder: phagocytosis, lymphatic transport Overall: 4,000 chemical compounds, of which 43 are considered carcinogenic

17
Squamous cell carcinoma Clin: Smokers (98%) 20-30% of common carcinomas May secrete PTH-like compound Rad: central > > peripheral Path: Bronchi > Larynx > Trachea +/- Desmosomes (intercellular bridges) +/- Keratin production, e.g. keratin pearls

18
Normal

20
Squamous cell carcinoma

21
Squamous cell carcinoma in situRespiratory mucosa

22
Invasive Squamous Carcinoma Keratin Desmosomes

23
Metastatic squamous cell carcinoma to lymph node Normal lymph node lymphocytes Mets in subcapsular sinuses

24
Adenocarcinoma Clin: 30-40% of common carcinomas Most common carcinoma in non-smokers, but 80% of adenoCAs occur in smokers Rad: peripheral > central Path: +/- glands +/- mucin Bronchiolo-alveolar carcinoma subset

25
Adenocarcinoma Primary Pleural effusion

26
Adenocarcinoma Gland formation

27
Adenocarcinoma Mucin production (red on PASd stain)
")
28
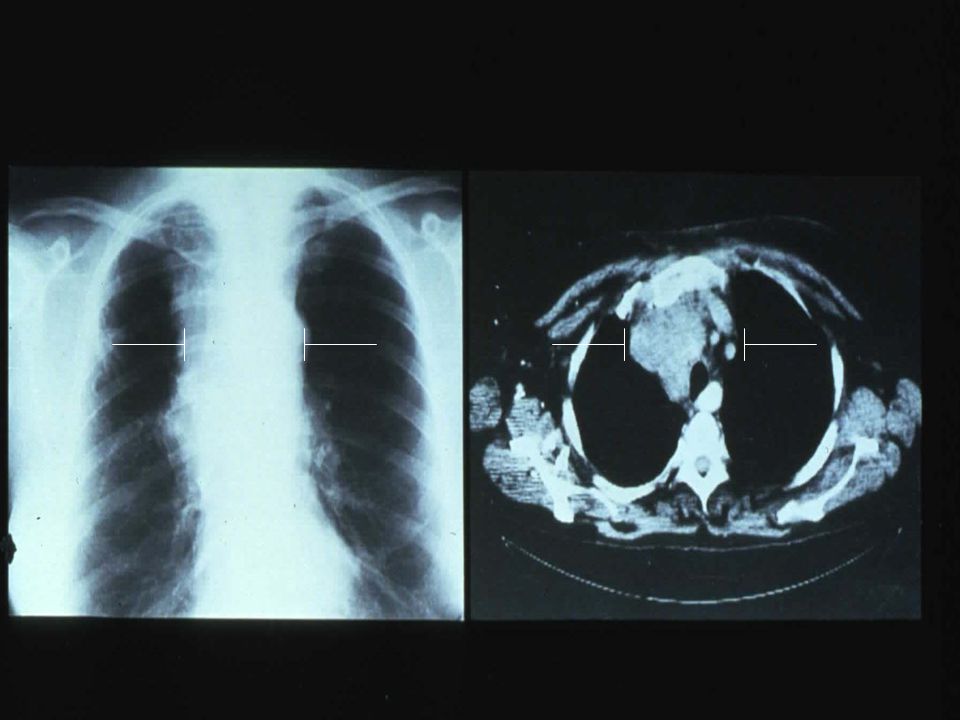
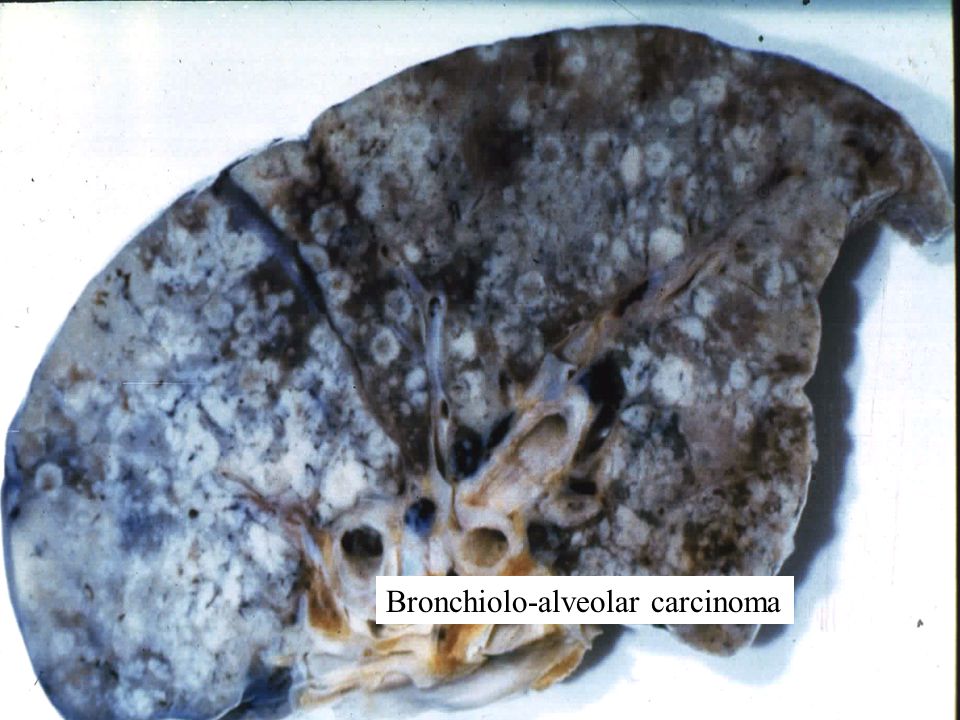
Bronchioloalveolar carcinoma (BAC) Clin: Rising incidence (presently 20-25%) Not associated with cigarette smoking Rad: Peripheral, can be multifocal and bilateral Path: Lepidic (butterfly-like) growth pattern Mucinous or non-mucinous Unifocal or multifocal Distinction of multifocal primary from mets
 Clin: Rising incidence (presently 20-25%) Not associated with cigarette smoking Rad: Peripheral, can be multifocal and bilateral Path: Lepidic (butterfly-like) growth pattern Mucinous or non-mucinous Unifocal or multifocal Distinction of multifocal primary from mets")
29
Bronchiolo-alveolar carcinoma

32
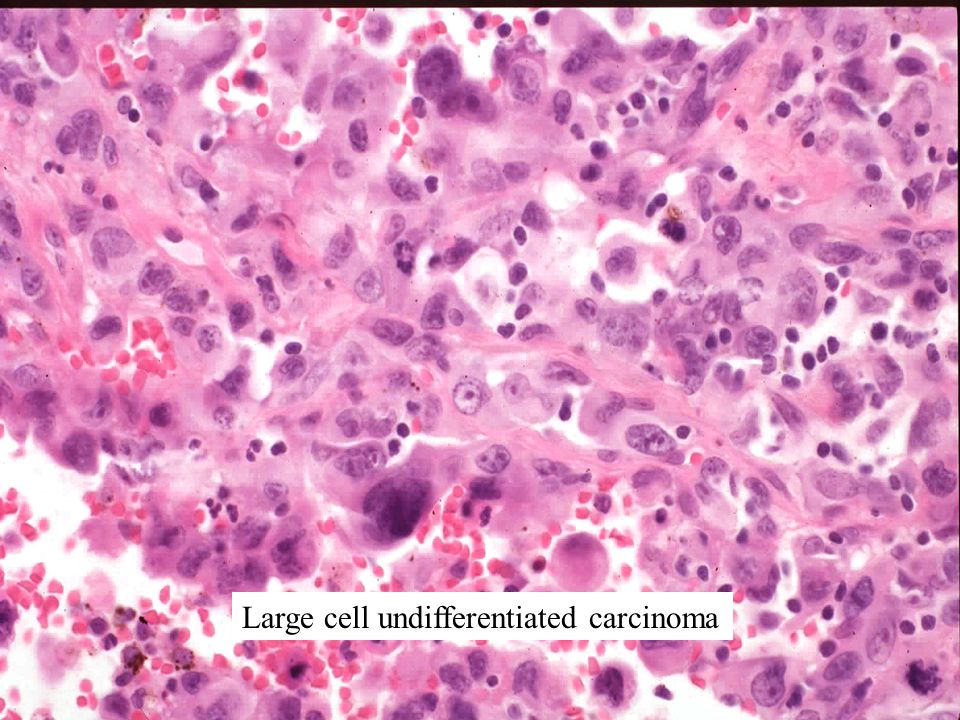
Large cell undifferentiated carcinoma Clin: 10% of common carcinomas Rad: non-specific Path: H&E: Undifferentiated EM: ? adenocarcinomas cDNA microarrays: distinct disease

33
Large cell undifferentiated carcinoma

35
Non-Small Cell Lung Carcinomas: Prognostic variables Definitely: Stage, performance status, weight loss Possibly gender, ploidy, k-ras mutation, p53 protein accumulation Not age, histology

36
Small cell carcinoma Clin: Smokers 20 % of common carcinomas Ectopic ACTH, ADH, Eaton-Lambert, carcinoid s. Commonly high stage at presentation Responsive to chemo/RT, but low 5 yr survival Rad: Central in >90% Frequent metastases to LNs and distant sites Path: Malignant cytology No nucleoli High mitotic activity and necrosis

37
Small cell undifferentiated carcinoma At diagnosis Response to therapy

38
Small cell undifferentiated carcinoma Viable carcinoma Necrotic carcinoma

39
Small cell undifferentiated carcinoma

41
Metastatic small cell carcinomaNormal lymphocytes

42
Small Cell Lung Carcinoma: Prognostic variables Definitely: Stage, performance status Probably: Gender, age, # of metastatic sites

43
Neoplasms of Lung & Pleura: Classification by Lineage Epithelial Melanocytic Stromal Mesothelial Metastases

44
Mesothelioma Clin: Associated with asbestos exposure Rad: Diffuse pleural involvement May have associated effusion Path: Malignant Deeply invasive growth pattern Epithelial, spindle cell, or biphasic Immuno: Keratin (+) EM: long microvilli
 EM: long microvilli")
45
Mesothelioma: PA Chest Visible C-P Angle Loss of C-P Angle = Pleural effusion or mass

46
Mesothelioma: CT Thickened pleura Normal thickness pleura

47
Normal thin pleura

48
Deeply invasive mesothelioma (cytokeratin immunostain)
")
49
Epithelioid cytology of this mesothelioma mimics adenocarcinoma

50
Adenocarcinoma Mesothelioma N. Weidner

51
Asbestos body (Ferruginous body)
")
52
Neoplasms of Lung & Pleura: Metastases Most common malignant neoplasms involving the lung Multiple nodules favor metastases over primary neoplasms (except BAC) Carcinomas Sarcomas Melanoma
 Carcinomas Sarcomas Melanoma")
53
Metastatic carcinomas Breast adenoCA GI adenoCA Renal adenoCA Head/neck squamous cell CA

54
Metastatic Breast CA Pleural Thickening due to Metastases +/- Pleural Effusion

55
Metastatic breast carcinoma

56
Metastatic colon carcinoma

57
Metastatic renal cell carcinoma

58
Metastatic ENT carcinoma

59
Metastatic sarcomas Osteosarcomas Soft tissue sarcomas

60
Metastatic osteosarcoma

61
Metastatic melanoma Clin: Extrapulmonary 1 melanoma much more common than pulmonary 1 No known 1 in 5-10% of cases Path: Variable architecture & cytology May be pigmented Use immunohistochemistry to confirm

62
Metastatic melanoma

63
Neoplasms of Lung and Pleura 1 Lung Neoplasms - Most are carcinomas 1 Pleural Neoplasms - Mesotheliomas Mets to Lung and/or pleura – All lineages possible

64
Thanks for your time. Questions?

Similar presentations



>")



 SHEN JIN The First Affiliated Hospital of Kunming Medical College.>")












 l malignant (very common) r Metastatic (Very common)>")

