Download presentation
Presentation is loading. Please wait.

1
Clifford W. Barlow (FRCS, DPhil) Southampton General Hospital Southampton, UK
 Southampton General Hospital Southampton, UK")
2
Quality and Outcomes differ for different individuals Are you operating for survival or symptoms Short-term:Survival (30 day or ‘in-hospital’) Complications (bleeding, stroke, peri-operative MI) Length of Stay Long-term:Survival Major Adverse Clinical Events (MI, stroke) Re-intervention (PCI or CABG)
 Complications (bleeding, stroke, peri-operative MI) Length of Stay Long-term:Survival Major Adverse Clinical Events (MI, stroke) Re-intervention (PCI or CABG)")
3
Evidence is a two way street Syntax Study (evidence ‘in’) Syntax Study (evidence ‘in’) -provides best evidence about which patients need CABG - ‘forgotten’ aspect arising from Syntax is Heart Team role Should surgeons be expected to provide evidence? Should surgeons be expected to provide evidence? -what we do and how well we do it? (evidence ‘out’) -current UK practice of publication of Outcome data (Hospital and Surgeon Specific Data (SSD)) Innovation and Research are not contra –indicated but potentially can be enhanced by both ‘in and out’ evidence Innovation and Research are not contra –indicated but potentially can be enhanced by both ‘in and out’ evidence
 -current UK practice of publication of Outcome data (Hospital and Surgeon Specific Data (SSD)) Innovation and Research are not contra –indicated but potentially can be enhanced by both ‘in and out’ evidence Innovation and Research are not contra –indicated but potentially can be enhanced by both ‘in and out’ evidence.")
4
-Appropriate referral is essential for quality -Syntax Study provides undisputable evidence that a majority of 3 vessel disease patients benefit from CABG (survival, MACCE events, re-intervention) -Emphasis should not solely focus on CABG vs PCI debate but stimulate further investigation into the debate about who needs revascularization (ischemic myocardium)
 -Emphasis should not solely focus on CABG vs PCI debate but stimulate further investigation into the debate about who needs revascularization (ischemic myocardium)")
5
-Role of Heart Team - ‘forgotten’ Syntax recommendation (incl. Surgeon/Interventional Cardiologist) -Syntax Score provides angiographic evidence -Individual patient needs differ -Number of publications emphasize the importance of individual patient factors/frailty scores (eg Syntax II) -Treatment recommendation by Heart Team, rather than individual practitioner, to ensure most appropriate intervention strategy for individual patient
 -Syntax Score provides angiographic evidence -Individual patient needs differ -Number of publications emphasize the importance of individual patient factors/frailty scores (eg Syntax II) -Treatment recommendation by Heart Team, rather than individual practitioner, to ensure most appropriate intervention strategy for individual patient.")
6
- Trigger: Children’s Heart Surgery, Bristol UK, 1984- 1995 - Kennedy Enquiry emphasized importance of transparency, openness and honesty in cardiac surgical practice and outcomes -Gradual evolution, from 2002, of hospital and, more controversially, surgeon specific data (SSD) release in UK -Intention two fold: Improve quality of care Inform patients that care safe
 release in UK -Intention two fold: Improve quality of care Inform patients that care safe")
7
-Society for Cardiothoracic Surgery in the UK and Ireland (SCTS) has taken lead in hospital and surgeon specific data (SSD) release -Bristol events/ Sir Bruce Keogh, Medical Director of NHS, initiated process (individual surgeon data collection commenced 2003) -Process in evolution but ‘CABG came first’ -Advantages and disadvantages -ongoing debate and controversy -Motivation remains to improve quality by providing understandable, uniform, appropriate outcome data to patients and physicians
 has taken lead in hospital and surgeon specific data (SSD) release -Bristol events/ Sir Bruce Keogh, Medical Director of NHS, initiated process (individual surgeon data collection commenced 2003) -Process in evolution but ‘CABG came first’ -Advantages and disadvantages -ongoing debate and controversy -Motivation remains to improve quality by providing understandable, uniform, appropriate outcome data to patients and physicians")
10
Surgeon (Dimitrios – case mix

16
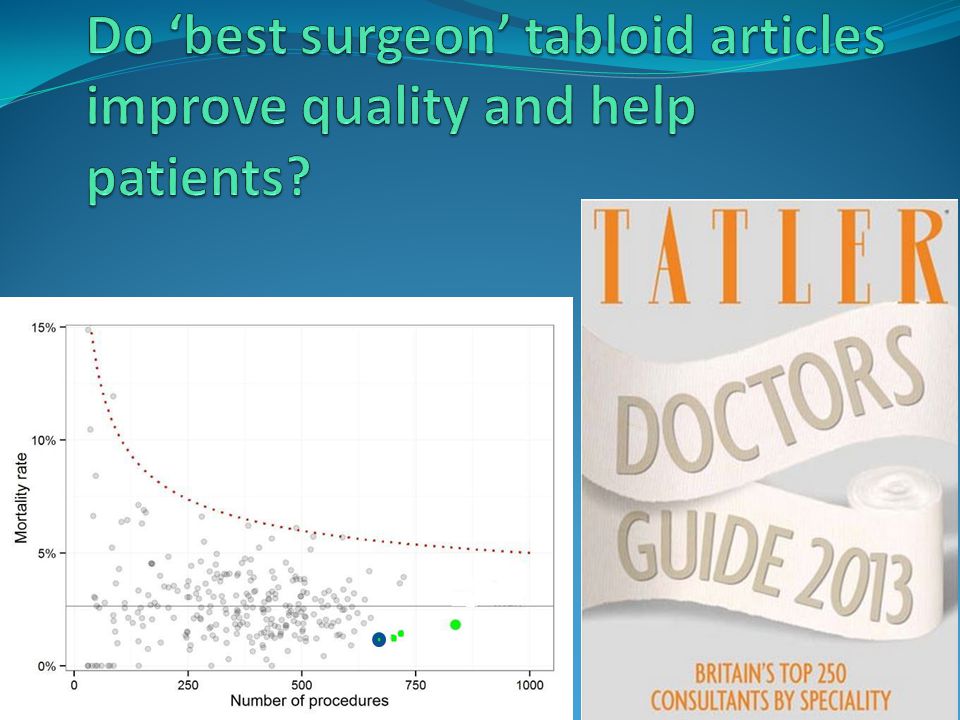
Strongly conflicting views within all surgical specialties but led by Cardiac Surgeons about publication of SSD Controversy about advantages and disadvantages of SSD Also, is early mortality the best primary measure of quality? Further changes in both content and mode of data release are proposed

18
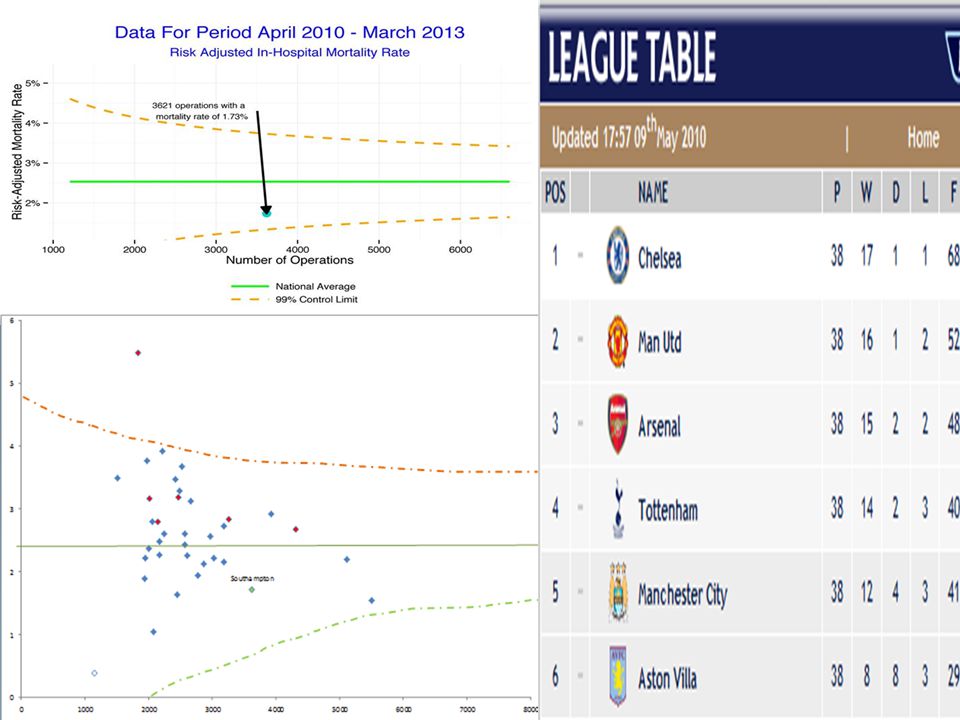
-Recent reported drop in mortality after CABG is not causally related to SSD -UK practice currently publishes All Case mortality data (not isolated procedures eg. CABG) -Time periods (3 years released annually) do not show continuity -Poor quality data and ‘gaming’ alters standard deviations and impacts ‘honest’ units -Creation of League Tables
 -Time periods (3 years released annually) do not show continuity -Poor quality data and ‘gaming’ alters standard deviations and impacts ‘honest’ units -Creation of League Tables.")
21
-Politically driven not evidence based -Anecdotal evidence risk averse behaviour by surgeons -’Outlier’ Surgeon is ‘second victim’ if wrongly identified (worsens performance) -Recent UK release all specialties – only 3 of 5000 judged underperforming (meaningless)
 -Recent UK release all specialties – only 3 of 5000 judged underperforming (meaningless)")
22
-Is a 0% mortality desirable or achievable? -Can this mechanism of unit and SSD release be extrapolated and meaningful in different healthcare systems? (different revalidation, case mix, resources, means improving quality)
.")
24
-Team Working -Sharing information drives improvement -Transparency – guides decision making patients/physicians -Incumbent on surgeon to be able to describe what he does and how well

25
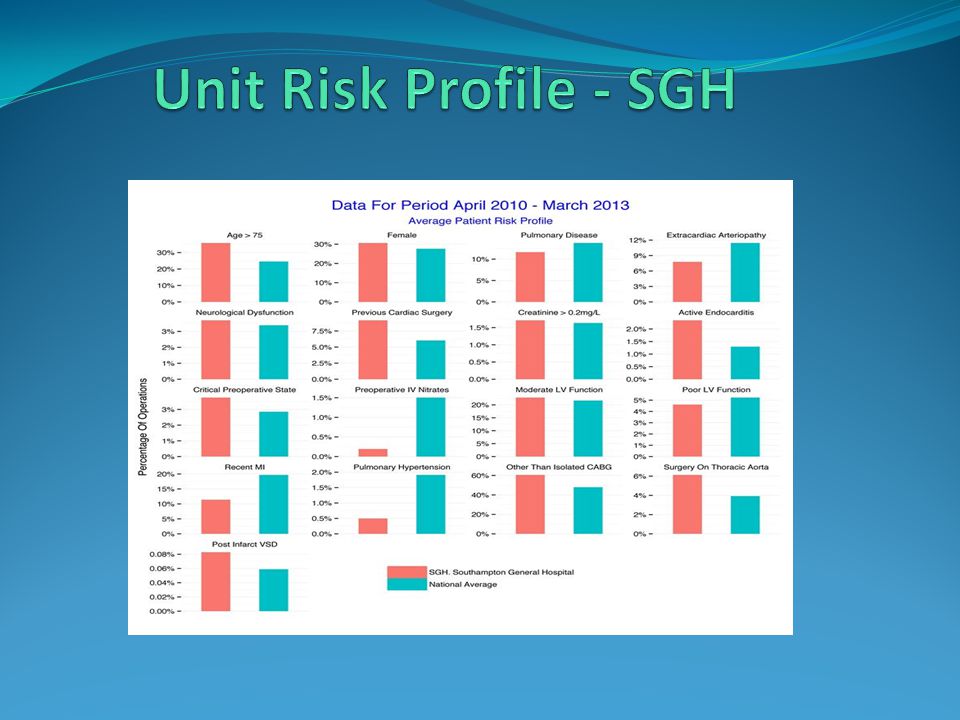
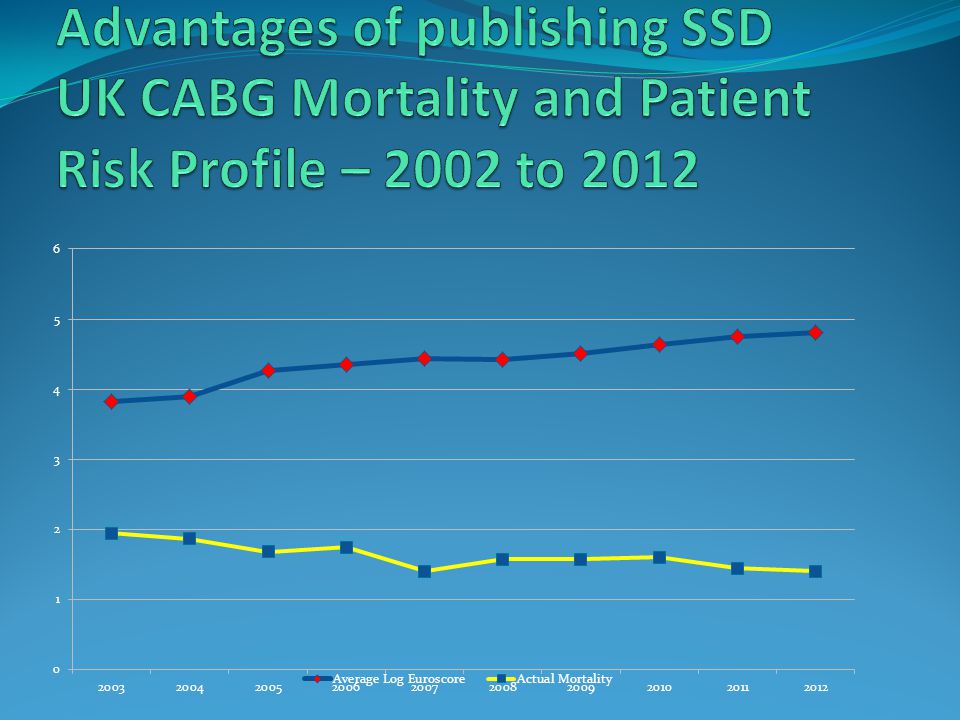
-No evidence risk-averse behaviour (overall patient risk profiles have increased) -Early identification of problems allows early corrective measures for hospitals and surgeons -Professional Cardiac Surgical Society driven SSD release ‘armours’ surgeons against potentially devastating newspaper tabloid scandals
 -Early identification of problems allows early corrective measures for hospitals and surgeons -Professional Cardiac Surgical Society driven SSD release ‘armours’ surgeons against potentially devastating newspaper tabloid scandals")
26
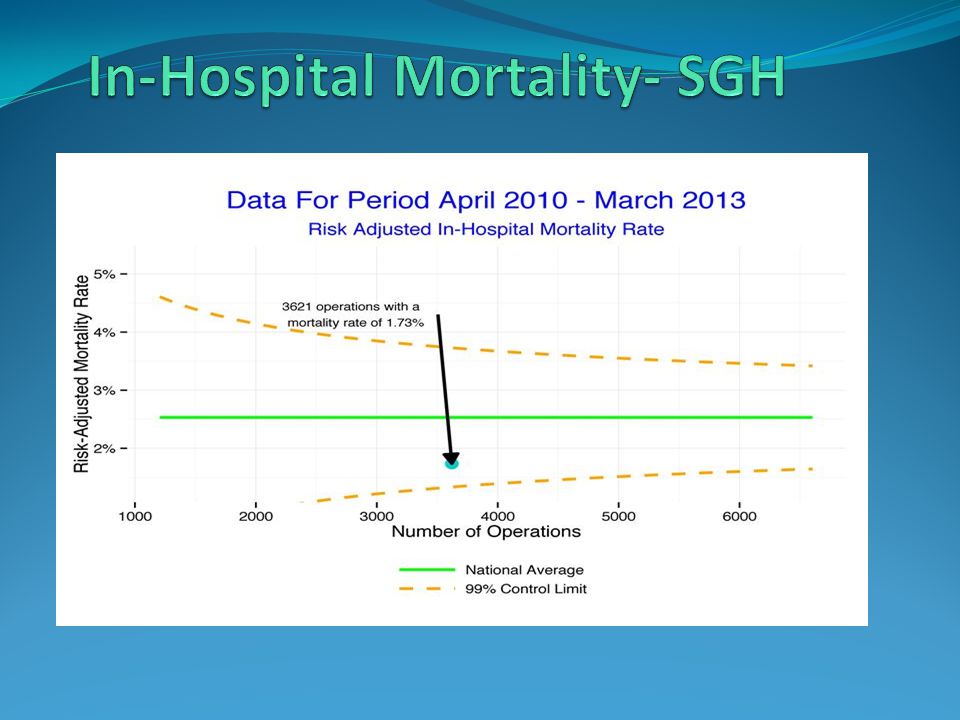
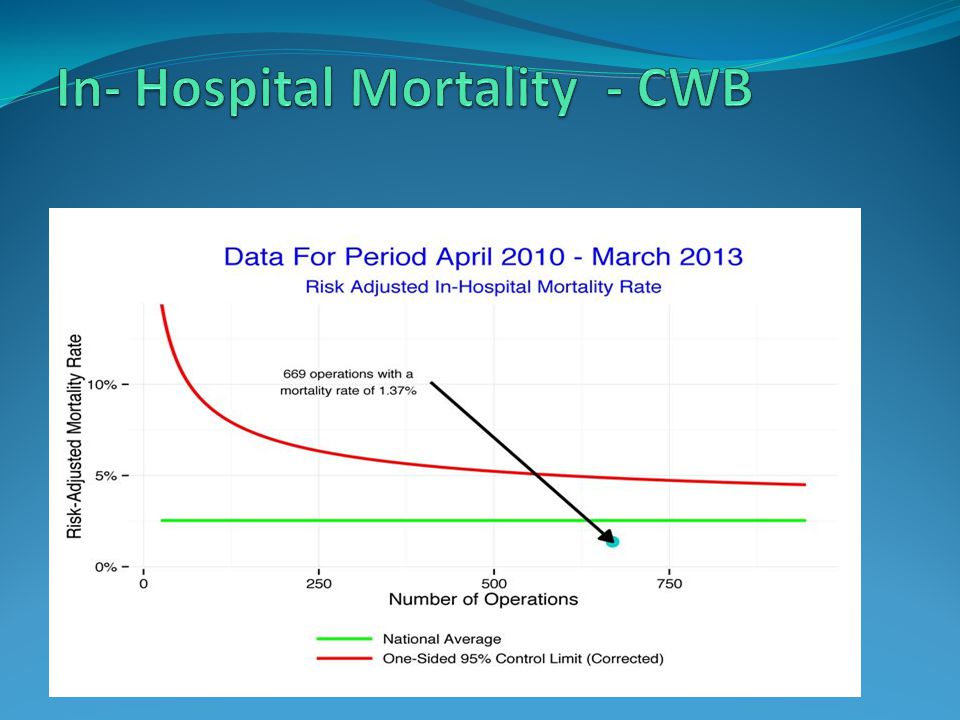
Elective and Urgent cases only – not Emergent Units/Hospitals must have resources to ensure data accuracy Internal/External ‘national sense checks’ Monitoring unit/surgeon outcomes against national ‘norms’

27
-Unit and Surgeon outcome divergence from expected is a statistical end point -Trigger to investigate accuracy of ‘outlier’ data and only then to publish -Some data will always be less accurate (eg age vs. unstable angina) -Identification of an outlier should trigger a process of support not punishment to improve quality
 -Identification of an outlier should trigger a process of support not punishment to improve quality.")
28
Essential that evidence from clinical studies (eg Syntax) should not entrench practice but encourage ongoing research (Evidence ‘in’) Similarly SSD release should not allow defensive practice (Evidence ‘out’) In CABG the major areas of future focus are: 1. The importance and means of establishing extent and location of ischemic myocardium (FAME Study) 2. Graft choice (RAPCO Study Update, ART Trial) 3. Technique (OPCAB),Exposure etc)
 2. Graft choice (RAPCO Study Update, ART Trial) 3. Technique (OPCAB),Exposure etc).")
29
Quality in CABG must be assessed with both: 1. Short-term outcomes (survival, LOS, complications) 2. Long-term outcomes (survival, MACCE events, re-intervention) There is growing evidence as to which patients need revascularisation and whether that should be CABG (Syntax) Future research (ART trial) will further define optimal CABG strategy in terms of conduit, technique and access Unit and Surgeon specific outcome data release can potentially improve transparency and drive quality (CABG specific, accurate, uniform, risk-adjusted, non-punitive)
 2. Long-term outcomes (survival, MACCE events, re-intervention) There is growing evidence as to which patients need revascularisation and whether that should be CABG (Syntax) Future research (ART trial) will further define optimal CABG strategy in terms of conduit, technique and access Unit and Surgeon specific outcome data release can potentially improve transparency and drive quality (CABG specific, accurate, uniform, risk-adjusted, non-punitive).")
Similar presentations