Download presentation
Presentation is loading. Please wait.

1
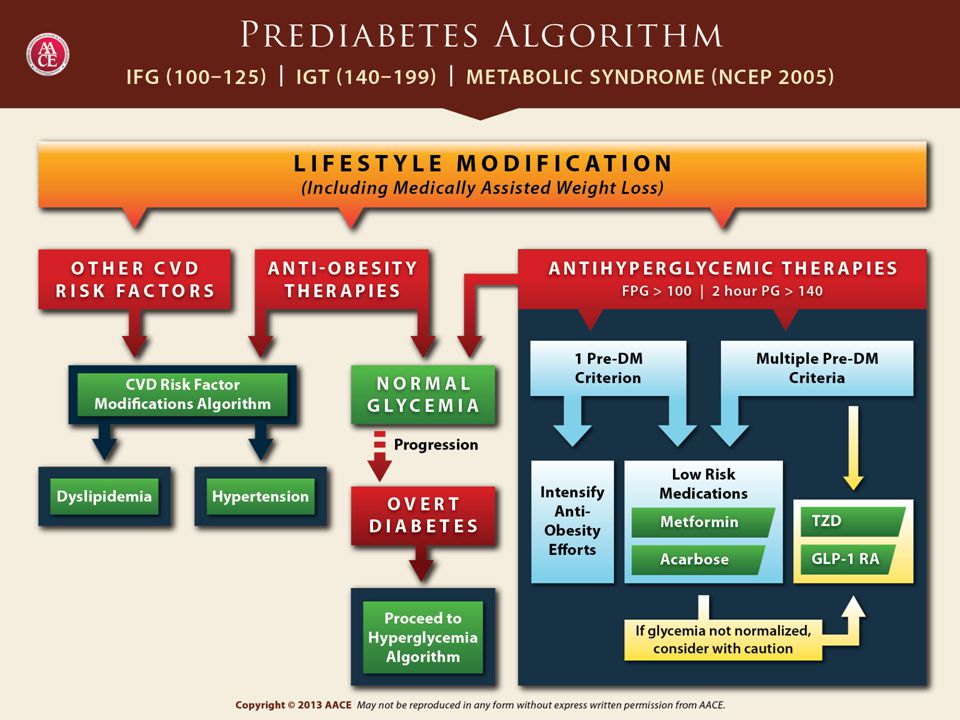
Prediabetes Management

2
AACE Prediabetes Consensus Statement: Summary
Untreated individuals with prediabetes are at increased risk for diabetes as well as for micro- and macrovascular complications Treatment goals are to prevent deterioration in glucose levels and modify other risk factors such as obesity, hypertension, and dyslipidemia The same blood pressure and lipid goals are suggested for prediabetes and diabetes Intensive lifestyle management is the cornerstone of all prevention efforts; pharmacotherapy targeted at glucose may be considered in high-risk patients Handelsman Y, et al. Endocr Pract. 2011;17(Suppl 2):1-53. Garber AJ, et al. Endocr Pract. 2008;14:
:1-53. Garber AJ, et al. Endocr Pract. 2008;14:")
3
Prediabetes Epidemiologic evidence suggests that the complications of T2DM begin early in the progression from NGT to frank diabetes Prediabetes and diabetes are conditions in which early detection is appropriate, because Duration of hyperglycemia is a predictor of adverse outcomes There are effective interventions to prevent disease progression and to reduce complications NGT, normal glucose tolerance ; T2DM , type 2 diabetes mellitus. Garber AJ, et al. Endocr Pract. 2008;14:

4
Policy Paradigm Shifts Needed to Stem Global Tide of T2DM
Integrating primary and secondary prevention along a clinical continuum Early detection of prediabetes and undiagnosed diabetes Implementing cost-effective prevention and control by integrating community and clinical expertise/resources within affordable service delivery systems Sharing and adopting evidence-based policies at the global level T2DM , type 2 diabetes mellitus. Narayan KM, et al. Health Aff (Millwood). 2012;31:84-92.
. 2012;31:")
6
Feasibility of Preventing T2DM
There is a long period of glucose intolerance that precedes the development of diabetes Screening tests can identify persons at high risk There are safe, potentially effective interventions that can address modifiable risk factors: Obesity Body fat distribution Physical inactivity High blood glucose T2DM, type 2 diabetes mellitus. Garber AJ, et al. Endocr Pract. 2008;14:

7
Interventions to Reduce Risks Associated With Prediabetes
Therapeutic lifestyle management is the cornerstone of all prevention efforts No pharmacologic agents are currently approved for the management of prediabetes Pharmacotherapy targeted at glucose may be considered in high-risk patients after individual risk-benefit analysis Garber AJ, et al. Endocr Pract. 2008;14:

8
Lifestyle Intervention in Prediabetes
Persons with prediabetes should reduce weight by 5% to 10%, with long-term maintenance at this level A diet that includes caloric restriction, increased fiber intake, and (in some cases) carbohydrate intake limitations is advised. A program of regular moderate-intensity physical activity for minutes daily, at least 5 days a week, is recommended Garber AJ, et al. Endocr Pract. 2008;14:
 carbohydrate intake limitations is advised. A program of regular moderate-intensity physical activity for minutes daily, at least 5 days a week, is recommended. Garber AJ, et al. Endocr Pract. 2008;14:")
9
Primary Care-Based Counseling for T2DM Prevention: ADAPT
ADAPT, Avoiding Diabetes Thru Action Plan Targeting; T2DM , type 2 diabetes mellitus. Mann DM, Lin JJ. Implement Sci. 2012;23:6.

10
Self-Reported Risk Reduction Activities in Patients With Prediabetes
National Health and Nutrition Examination Survey Patients CDC. MMWR Morb Mortal Wkly Rep. 2008;57:

11
Prevention of Diabetes: Lifestyle Studies
Prediabetes Management Prevention of Diabetes: Lifestyle Studies

12
Prevention of T2DM: Selected Lifestyle Modification Trials
Study Country N Baseline BMI (kg/m2) Intervention period (years) RRR (%) NNT Diabetes Prevention Program USA 3234 34.0 2.8 58 21 Diabetes Prevention Study Finland 523 31 4 39 22 Da Qing China 577 25.8 6 51 30 BMI, body mass index; NNT, number needed to treat; RRR, relative risk reduction; T2DM, type 2 diabetes mellitus. DPP Research Group. N Engl J Med. 2002;346: Eriksson J, et al. Diabetologia. 1999;42: Li G, et al. Lancet. 2008;371: Lindstrom J, et al. Lancet. 2006;368:
 Intervention period. (years) RRR. (%) NNT. Diabetes Prevention Program. USA Diabetes Prevention Study. Finland Da Qing. China BMI, body mass index; NNT, number needed to treat; RRR, relative risk reduction; T2DM, type 2 diabetes mellitus. DPP Research Group. N Engl J Med. 2002;346: Eriksson J, et al. Diabetologia. 1999;42: Li G, et al. Lancet. 2008;371: Lindstrom J, et al. Lancet. 2006;368:")
13
T2DM Incidence in the Diabetes Prevention Program
31% 58% per 100 person-years T2DM incidence Intensive lifestyle intervention* (n=1079) Metformin 850mg BID (n=1073) Placebo (n=1082) *Goal: 7% reduction in baseline body weight through low-calorie, low-fat diet and ≥150 min/week moderate intensity exercise. IGT, impaired glucose tolerance; T2DM, type 2 diabetes mellitus. DPP Research Group. N Engl J Med. 2002;346:
 Metformin 850mg BID. (n=1073) Placebo. (n=1082) *Goal: 7% reduction in baseline body weight through low-calorie, low-fat diet and ≥150 min/week moderate intensity exercise. IGT, impaired glucose tolerance; T2DM, type 2 diabetes mellitus. DPP Research Group. N Engl J Med. 2002;346:")
14
Effect of Age on Incidence of T2DM in the DPP
48% per 100 person-years T2DM incidence 59% 71% Age (years) *Goal: 7% reduction in baseline body weight through low-calorie, low-fat diet and ≥150 min/week moderate intensity exercise. DPP, Diabetes Prevention Program;. DPP Research Group. N Engl J Med. 2002;346:
 *Goal: 7% reduction in baseline body weight through low-calorie, low-fat diet and ≥150 min/week moderate intensity exercise. DPP, Diabetes Prevention Program;. DPP Research Group. N Engl J Med. 2002;346:")
15
Effect of Weight on T2DM Incidence in the DPP
51% per 100 person-years T2DM incidence 65% 61% BMI (kg/m2) *Goal: 7% reduction in baseline body weight through low-calorie, low-fat diet and ≥150 min/week moderate intensity exercise. DPP, Diabetes Prevention Program. DPP Research Group. N Engl J Med. 2002;346:
 *Goal: 7% reduction in baseline body weight through low-calorie, low-fat diet and ≥150 min/week moderate intensity exercise. DPP, Diabetes Prevention Program. DPP Research Group. N Engl J Med. 2002;346:")
16
10-Year Weight Loss in the DPP Outcomes Study
3 2 5 4 7 6 8 10 9 Years DPP, Diabetes Prevention Program; T2DM, type 2 diabetes mellitus. DPP Research Group. Lancet. 2009;374:

17
10-Year Incidence of T2DM in the DPP Outcomes Study
3 2 5 4 7 6 8 10 9 Placebo Metformin Lifestyle Years DPP, Diabetes Prevention Program; T2DM, type 2 diabetes mellitus. DPP Research Group. Lancet. 2009;374:

18
10-Year Incidence of T2DM in the DPP Outcomes Study
DPP, Diabetes Prevention Program; DPPOS, Diabetes Prevention Program Outcomes Study; T2DM, type 2 diabetes mellitus. DPP Research Group. Lancet. 2009;374:

19
T2DM Prevention in Women With a History of GDM: Effect of Metformin and Lifestyle Interventions
Findings from the DPP: Progression to diabetes is more common in women with a history of GDM vs those without, despite equivalent degrees of IGT at baseline Both intensive lifestyle and metformin are highly effective in delaying or preventing diabetes in women with IGT and a history of GDM DPP, Diabetes Prevention Program; GDM, gestational diabetes mellitus; IGT, impaired glucose tolerance; T2DM, type 2 diabetes mellitus. Ratner RE, et al. J Clin Endocrinol Metab. 2008;93:

20
T2DM Prevention in Women With a History of GDM: Effect of Metformin and Lifestyle Interventions
Findings from the DPP: Progression to diabetes is more common in women with a history of GDM vs those without, despite equivalent degrees of IGT at baseline Both intensive lifestyle and metformin are highly effective in delaying or preventing diabetes in women with IGT and a history of GDM DPP, Diabetes Prevention Program; GDM, gestational diabetes mellitus; IGT, impaired glucose tolerance; T2DM, type 2 diabetes mellitus. Ratner RE, et al. J Clin Endocrinol Metab. 2008;93:

21
The Finnish Diabetes Prevention Study: Lifestyle Modifications
Change from baseline P<0.001 P<0.001 P=0.007 P=0.02 DBP, diastolic blood pressure; SBP, systolic blood pressure. Tuomilehto J, et al. N Engl J Med. 2001;344:

22
The Finnish Diabetes Prevention Study: Lifestyle Modifications
Change from baseline P=0.003 P=0.001 (mg/dL) (mg/dL) (mg/mL) (g/mL) DBP, diastolic blood pressure; SBP, systolic blood pressure. Tuomilehto J, et al. N Engl J Med. 2001;344:
 (mg/dL) (mg/mL) (g/mL) DBP, diastolic blood pressure; SBP, systolic blood pressure. Tuomilehto J, et al. N Engl J Med. 2001;344:")
23
(cases/1000 person-years)
The Finnish Diabetes Prevention Study: Cumulative Incidence of Diabetes Over 4 Years 58% (cases/1000 person-years) Incidence of diabetes DBP, diastolic blood pressure; SBP, systolic blood pressure. Tuomilehto J, et al. N Engl J Med. 2001;344:
 Incidence of diabetes. DBP, diastolic blood pressure; SBP, systolic blood pressure. Tuomilehto J, et al. N Engl J Med. 2001;344:")
24
Da Qing: Cumulative Incidence of Diabetes at 6-Year Evaluation
Patients with IGT (N=577) Patients with T2DM at Year 6 (%) IGT, impaired glucose tolerance. Pan XR, et al. Diabetes Care. 1997;20:
 Patients with T2DM at Year 6 (%) IGT, impaired glucose tolerance. Pan XR, et al. Diabetes Care. 1997;20:")
25
Cumulative T2DM Incidence During Follow-up in the Chinese Da Qing Diabetes Prevention Study
CI, confidence interval; DPP, Diabetes Prevention Program; T2DM, type 2 diabetes mellitus. Li G, et al. Lancet. 2008;371:

26
Group Lifestyle Balance Program Intervention
University of Pittsburgh Primary Care Practice and Diabetes Prevention Support Center DPP lifestyle intervention was adapted to a 12-session group-based program Implemented in a community setting in 2 phases using a nonrandomized prospective design Significant decreases in weight, waist circumference, and BMI were noted in both phases vs baseline Average combined weight loss for both groups over the 3-month intervention was 7.4 pounds (3.5% relative loss, P<0.001) DPP, Diabetes Prevention Program; mo, month. Kramer MK, et al. Am J Prev Med. 2009;37:
 DPP, Diabetes Prevention Program; mo, month. Kramer MK, et al. Am J Prev Med. 2009;37:")
27
Translating the DPP Into Community Intervention
The DEPLOY Pilot Study Pilot, cluster-randomized trial Group-based DPP lifestyle intervention vs brief counseling alone (control) among high-risk adults who attended a diabetes risk-screening event at one of two semi-urban YMCA facilities P=0.002 P<0.001 DEPLOY, Diabetes Education & Prevention with a Lifestyle Intervention Offered at the YMCA; DPP, Diabetes Prevention Program; YMCA, Young Men’s Christian Association. Ackermann RT, et al. Am J Prev Med. 2008;35:
 among high-risk adults who attended a diabetes risk-screening event at one of two semi-urban YMCA facilities. P= P< DEPLOY, Diabetes Education & Prevention with a Lifestyle Intervention Offered at the YMCA; DPP, Diabetes Prevention Program; YMCA, Young Men’s Christian Association. Ackermann RT, et al. Am J Prev Med. 2008;35:")
28
Montana CVD and DPP Mean weight and physical activity min/week among participants by lifestyle intervention session CVD, cardiovascular disease; DPP, Diabetes Prevention Program. Amundson HA, et al. Diabetes Educ. 2009;35:

29
Translation of the DPP’s Lifestyle Intervention
Four additional studies utilizing the DPP lifestyle interventions in community settings provided the following findings: Promising evidence of the prevention of diabetes by significantly decreasing glucose levels and adiposity Statistically significant improvements in many behavioral outcomes and anthropometrics, particularly at 6 months Decreased fasting glucose and weight in at-risk African Americans Approaches that improve recruitment of participants from underserved communities into research, especially research related to chronic disease risk factors DPP, Diabetes Prevention Program. Boltri JM, et al. J Natl Med Assoc. 2011;103: Katula JA, et al. Diabetes Care. 2011;34: Ruggiero L, et al. Diabetes Educ. 2011;37: Santoyo-Olsson J, et al. Gerontologist. 2011;51(Suppl 1):S82-93.
:S")
30
Prevention of Diabetes: Pharmacotherapy Studies
Prediabetes Management Prevention of Diabetes: Pharmacotherapy Studies

31
Rate of Conversion to Normal Glucose Tolerance
Pharmacologic Interventions Proven to Delay or Prevent T2DM Development Intervention Rate of Conversion to Normal Glucose Tolerance Metformin (2 trials) 26%-31% Acarbose (1 trial) 25% Pioglitazone (1 trial) 48% T2DM, type 2 diabetes mellitus. Sherwin RS, et al. Diabetes Care. 2004;27,(Suppl 1): S47-S54. Eriksson K-F, Lindgärde F. Diabetologia. 1991;34: Ramachandran A, et al. Diabetologia 2006;49: Knowler WC, et al. N Engl J Med. 2002;346: Defronzo RA, et al. N Engl J Med. 2011;364:
 26%-31% Acarbose (1 trial) 25% Pioglitazone (1 trial) 48% T2DM, type 2 diabetes mellitus. Sherwin RS, et al. Diabetes Care. 2004;27,(Suppl 1): S47-S54. Eriksson K-F, Lindgärde F. Diabetologia. 1991;34: Ramachandran A, et al. Diabetologia 2006;49: Knowler WC, et al. N Engl J Med. 2002;346: Defronzo RA, et al. N Engl J Med. 2011;364:")
32
The Chinese Prevention Study
The Effect of Metformin on the Progression of IGT to Diabetes Mellitus (N=321) 65% Incidence of Diabetes (%/yr) Control Metformin IGT, impaired glucose tolerance; RRR, relative risk reduction. Yang W, et al. Chin J Endocrinol Metab. 2001;17:
 65% Incidence of Diabetes (%/yr) Control. Metformin. IGT, impaired glucose tolerance; RRR, relative risk reduction. Yang W, et al. Chin J Endocrinol Metab. 2001;17:")
33
Effect of Lifestyle Modification and Metformin on Cumulative Diabetes Incidence The Indian DPP (N=531) RRR (%) 26.4 P=0.029 28.5 P=0.018 28.2 P=0.022 Incidence (%) n=136 n=133 n=133 n=129 Control LSM MET LSM & MET DPP, Diabetes Prevention Program; LSM, lifestyle modification; MET, metformin; RRR, relative risk reduction. Ramachandran A, et al. Diabetologia 2006;49:
 P= P= P= Incidence (%) n=136. n=133. n=133. n=129. Control. LSM. MET. LSM & MET. DPP, Diabetes Prevention Program; LSM, lifestyle modification; MET, metformin; RRR, relative risk reduction. Ramachandran A, et al. Diabetologia 2006;49:")
34
Effect of Acarbose on Reversion of IGT to NGT
The Study to Prevent Non-Insulin Dependent Diabetes Mellitus (STOP-NIDDM) P<0.0001 n=241 (35.3%) Number of Patients n=212 (30.9%) Placebo Acarbose IGT, impaired glucose tolerance; NGT, normal glucose tolerance. Chiasson JL, et al. Lancet. 2002;359:
 P< n=241. (35.3%) Number of Patients. n=212. (30.9%) Placebo. Acarbose. IGT, impaired glucose tolerance; NGT, normal glucose tolerance. Chiasson JL, et al. Lancet. 2002;359:")
35
DREAM: Rosiglitazone and New-Onset Diabetes or Death
No. at risk Placebo Rosiglitazone 0.6 0.5 1 2 3 4 Follow-up (years) 0.4 0.3 0.2 0.1 0.0 Placebo Cumulative hazard rate Rosiglitazone 60% DREAM: Rosiglitazone prolongs time to occurrence of new-onset diabetes or death DREAM Trial Investigators. Lancet. 2006;368:
 Placebo. Cumulative hazard rate. Rosiglitazone. 60% DREAM: Rosiglitazone prolongs time to occurrence of new-onset diabetes or death. DREAM Trial Investigators. Lancet. 2006;368:")
36
Pioglitazone for T2DM Prevention in IGT: ACT NOW
Kaplan–Meier plot of hazard ratios for time to development of T2DM ACT NOW, Actos NOW for the Prevention of Diabetes; IGT, impaired glucose tolerance; T2DM, type 2 diabetes mellitus. Defronzo RA, et al. N Engl J Med. 2011;364:

37
Special Concerns for Thiazolidinedione Use in Patients With Prediabetes
Because of concerns about long-term safety, use of thiazolidinediones should be reserved for higher risk populations and those failing other, lower-risk strategies Garber AJ, et al. Endocr Pract. 2008;14:

38
Effects of Exenatide and Lifestyle Modification on Body Weight and Glucose Tolerance in Obese Patients With and Without Prediabetes Patients N=152, weight / kg, BMI /- 7.0 kg/m2 (IGT or IFG 25%) Design 24-week randomized controlled trial: exenatide or placebo plus lifestyle intervention Results: Exenatide-treated patients lost 5.1 kg from baseline vs 1.6 kg with placebo (P<0.001) Both groups reduced their daily caloric intake IGT or IFG normalized at end point in 77% and 56% of exenatide and placebo subjects, respectively BMI, body mass index; IFG, impaired fasting glucose; IGT, impaired glucose tolerance. Rosenstock J, et al. Diabetes Care. 2010;33:
 Design. 24-week randomized controlled trial: exenatide or placebo plus lifestyle intervention. Results: Exenatide-treated patients lost 5.1 kg from baseline vs 1.6 kg with placebo (P<0.001) Both groups reduced their daily caloric intake. IGT or IFG normalized at end point in 77% and 56% of exenatide and placebo subjects, respectively. BMI, body mass index; IFG, impaired fasting glucose; IGT, impaired glucose tolerance. Rosenstock J, et al. Diabetes Care. 2010;33:")
39
Medical Weight-Loss Strategies
Orlistat may prevent progression from prediabetes to diabetes Lorcaserin, a selective serotonin 2C agonist, is indicated for use in obese patients with at least 1 weight-related comorbid condition (eg, hypertension, dyslipidemia, CVD, glucose intolerance, sleep apnea) Low-dose, immediate-release phentermine and controlled-release topiramate is recommended for obese or overweight patients with weight-related comorbidities such as hypertension, T2DM, dyslipidemia, or central adiposity CVD, cardiovascular disease; obese, BMI ≥30 kg/m2; overweight, BMI ≥27 kg/m2; T2DM, type 2 diabetes mellitus. Garber AJ, et al. Endocr Pract. 2008;14:
 Low-dose, immediate-release phentermine and controlled-release topiramate is recommended for obese or overweight patients with weight-related comorbidities such as hypertension, T2DM, dyslipidemia, or central adiposity. CVD, cardiovascular disease; obese, BMI ≥30 kg/m2; overweight, BMI ≥27 kg/m2; T2DM, type 2 diabetes mellitus. Garber AJ, et al. Endocr Pract. 2008;14:")
40
Pharmacologic Weight-Loss Strategies
Drug name Placebo-subtracted mean % body weight loss from baseline Patients (N) in clinical program/ patients (n) with diabetes % of patients losing ≥5% of body weight Clinical trial withdrawal rates Orlistat 2.4% (following 4 years of treatment with orlistat 120 mg TID) 7504/321 35.5%-54.8% (following 1 year of treatment with orlistat 120 mg TID) 8.8% Lorcaserin 3.3% at 52 weeks 6888/510 47.1% 36%-50% Phentermine/ topiramate) 3.5%-6.4% 3678/808 45%-70% 31%-40% LOCF, last observation carried forward. Orlistat [package insert]. South San Francisco CA; Genentech USA; 2010. Belviq [package insert]. Woodcliff Lake, NJ; Eisai Inc.; 2012. Qsymia [package insert]. Mountain View, CA; VIVUS , Inc; 2012.
 in clinical program/ patients (n) with diabetes. % of patients losing ≥5% of body weight. Clinical trial withdrawal rates. Orlistat. 2.4% (following 4 years of treatment with orlistat 120 mg TID) 7504/ %-54.8% (following 1 year of treatment with orlistat 120 mg TID) 8.8% Lorcaserin. 3.3% at 52 weeks. 6888/ % 36%-50% Phentermine/ topiramate) 3.5%-6.4% 3678/ %-70% 31%-40% LOCF, last observation carried forward. Orlistat [package insert]. South San Francisco CA; Genentech USA; Belviq [package insert]. Woodcliff Lake, NJ; Eisai Inc.; Qsymia [package insert]. Mountain View, CA; VIVUS , Inc;")
41
Phentermine/Topiramate and Prevention of Type 2 Diabetes
76.6% 79.7% Annualized incidence of T2DM 48.6% 88.6% Garvey TW, et al. Diabetes Care. 2014;37:

Similar presentations








>")










