Download presentation
Presentation is loading. Please wait.

1
Dr. Sharda Jain Director: Global Institute of Gynaecoloy at Pushpanjali Crosslay Hospital Secretary general: Delhi Gynaecologist Forum Recurrent Pregnancy Loss

2
Learning Objectives n Identify possible causes of early pregnancy loss n Outline basic evaluation for recurrent pregnancy loss (RPL) n Review current treatment approaches for these patients
 n Review current treatment approaches for these patients")
3
Definition n Classical: 3 or more consecutive pregnancy losses before 20 weeks gestation n Expanded: 2 or more consecutive losses u Risk of further loss similar for 2 versus 3 consecutive losses u Initiation of evaluation appropriate after 2 losses based on patient age and desire Hill Curr Prob Obstet Gynecol Fertil 1994;37:693-704

4
Recurrent Loss Epidemiology n 5% of couples attempting pregnancy have 2 or more consecutive losses n 1% have 3 or more consecutive losses n Most clinicians consider RPL even if losses are not consecutive Lee Semin Reprod Med 2000;18(4):433-40
:433-40")
5
SPAB Epidemiology n 34% pregnancy loss in prospective cohort of healthy women u 22% unrecognized - detected by assay only u 12 % clinically recognized n Obstetrical history predictive u prior success: 4-6 % chance of loss u prior loss: 19-24%chance of loss Wilcox NEJM 1988;319:189-194

6
SPAB or RPL? n A single SAB, unless a successful pregnancy intervenes, increases the risk for the next pregnancy n Distinction between “sporadic” and “recurrent” loss blurred n Effect of maternal age: SAB risk approaches 50% by age 40 for both aneuploid and euploid losses Cramer Semin Reprod Med 2000;18(4):331-9
:")
7
Miscarriage Recurrence Risk Outcome Prior Losses Recurrence Risk % Liveborn012 124 226 332 426 No Live Births 119 235 347 454 Warburton D, Fraser FC: Am J Human Genet 16:1, 1964

8
PCOS & Pregnancy Loss n Pregnancy loss ↑ with PCOS n n Franks S, Ann Int Med 93, Jacobs HS BRJOBGYN 93 n GnRH-a ↓ miscarriage in PCOS women n n Homburg R, et al: Fertil Steril 59:527, 1993 n RSA patients with ↑ LH, DHEAS or T more likely to miscarry n n Tulpalla M, et al: BrJOBGYN 100:348, 1993 n GnRH-a ↓ miscarriages in RSA patients with PCOS compared to clomid (10% vs 55%) Johnson P, et al: BMJ 300:154, 1990
 Johnson P, et al: BMJ 300:154, 1990")
9
Metformin Reduces Pregnancy Loss in PCOS n Retrospective study of PCOS women who became pregnant u Group 1: metformin during pregnancy (n=101) u Group 2: control (n=31) n Early loss rate 12.9% vs 41.9% (p=0.001) n Prior SPAB: 15.7% vs 58.3% (p=0.005) Jakubowicz DJ, et al: abstract P2-427, Endocrine Society, 2001
 u Group 2: control (n=31) n Early loss rate 12.9% vs 41.9% (p=0.001) n Prior SPAB: 15.7% vs 58.3% (p=0.005) Jakubowicz DJ, et al: abstract P2-427, Endocrine Society, 2001")
10
Etiology Anatomic Factors n 10-15% recurrent 1 st trimester losses have congenital anomaly n Variations of the double uterus the most common n Septate loss rates 25-90% - usually amenable to resection n Bicornuate loss rates 40% - uncertain benefit of surgery Propst & Hill Semin Reprod Med 2000;18(4):341-50
:341-50")
11
Etiology Anatomic Factors n Unicornuate uteri 50% loss n Uterus didelphys 40% loss n DES exposure - many have abnormal uterine structure n Cervical incompetence n Intrauterine synechiae

12
Etiology Anatomic Factors n Unclear relationship between uterine leiomyomata and RPL u Large submucosal fibroids distort the cavity or occupy a large subendometrial area u ? Mechanism(s) - mechanical constriction or inadequate placentation resulting from poorly vascularized endometrium
 - mechanical constriction or inadequate placentation resulting from poorly vascularized endometrium.")
13
Acquired Uterine Defects

14
Etiology Infection n No infectious agent has been proven to cause recurrent pregnancy loss u ? Colonization with Ureaplasma urealyticum leading to empiric antibiotics n Certain infections have been associated with spontaneous loss u Toxoplasma gondii, rubella, HSV, CMV, measles, coxsackie Lee Semin Reprod Med 2000;18(4):433-40
:")
15
Etiology Genetic Factors n Trisomy (50%) u #16 all lethal 1/3 of all trisomies u #21 Down Syndrome usually due to meiotic non- disjunction 80% maternatal n Monsomy X (20%) u 45X Turner Syndrome most common n Triploidy (15%) u 90% from father n Tetraploidy (5%) n Mosaicism (2%) % Chromosomal Abnormal by Gestational Age % abnormal Gestational age 6012 4516 1220 624 ~140
 u #16 all lethal 1/3 of all trisomies u #21 Down Syndrome usually due to meiotic non- disjunction 80% maternatal n Monsomy X (20%) u 45X Turner Syndrome most common n Triploidy (15%) u 90% from father n Tetraploidy (5%) n Mosaicism (2%) % Chromosomal Abnormal by Gestational Age % abnormal Gestational age ~140")
16
Etiology Genetic Factors n Parental abnormalities in 3-5% of couples with recurrent loss n Balanced translocation most common u Reciprocal (60%) or Robertsonian (40%) u 25-50% risk of pregnancy loss u May eventually produce normal offspring
 or Robertsonian (40%) u 25-50% risk of pregnancy loss u May eventually produce normal offspring")
17
Etiology Genetic Factors

18
n Homologous Robertsonian translocation u 1/2500 couples u precludes successful reproduction n Heterozygous may lead to partial monosomy or trisomy; “milder” phenotypical expression Ward Semin Reprod Med 2000;18(4):425-32
:425-32")
20
Etiology Genetic Factors n Speculation about single gene mutations u Blastocyst formation u Implantation u Morphogenesis of vital organs

21
Etiology Genetic Factors n Skewed X inactivation u Preferential inactivation(>90%) of one of the X alleles u May be lethal to a male offspring u May result in X-autosome translocations u Trisomy mosaicism in the germline
 of one of the X alleles u May be lethal to a male offspring u May result in X-autosome translocations u Trisomy mosaicism in the germline")
22
Etiology Genetic Factors n Advanced maternal age u Impact on risk for pregnancy loss cannot be over-emphasized u Increased rates of maternally- derived trisomies u Probable “natural selection” of better quality oocytes earlier in reproductive life u Oocytes recruited later in life more likely to be abnormal or experience meiotic error

23
Lobo, R. A. N Engl J Med 2005;353:64-73 Decline in the Number of Oocytes from Birth to Menopause

24
Heffner, L. J. N Engl J Med 2004;351:1927-1929 Fertility and Miscarriage Rates as a Function of Maternal Age

25
Etiology Thrombophilia n Pregnancy is a hypercoagulable state n Women with heritable or acquired thrombophilic disorders have significantly increased risks of pregnancy loss Kutteh Semin Reprod Med 2006;24(1):54-65
:54-65")
26
Etiology Thrombophilia Venous n Most common inherited: u Heterozygous Factor V Leiden (G1691A) u Factor II-prothrombin mutation (G20210A) u Hyperhomocysteinemia (MTHFR C677T and A1298C)
 u Factor II-prothrombin mutation (G20210A) u Hyperhomocysteinemia (MTHFR C677T and A1298C)")
27
Etiology Thrombophilia Venous n Most common acquired: u Anti-phospholipid antibodies (APAs) u Activated Protein C resistance u Hyperhomocysteinemia (MTHFR C677T and A1298C) n Other possible abnormalities u Anti-thrombin deficiency u Protein C or S deficiency u Elevated Factor VIII
 u Activated Protein C resistance u Hyperhomocysteinemia (MTHFR C677T and A1298C) n Other possible abnormalities u Anti-thrombin deficiency u Protein C or S deficiency u Elevated Factor VIII")
28
Etiology Thrombophilia Arterial n Hyperhomocysteinemia n APAs n Lupus anticoagulant

29
Etiology Thrombophilia n Factor V Leiden u Abnormal factor V resistant to anticoagulant effects of activated protein C u Majority of patients resistant to activated protein C will be heterozygous for Factor V Leiden u Present in 3-8% of the White population u Rare in Blacks, Asians, Native Americans

30
Etiology Thrombophilia n Factor V Leiden u Autosomal dominant u Acquired activated protein C resistance in pregnancy, OCP use and in presence of APAs u Heterozygotes: 7X increase lifetime risk thrombosis; 15X increase during pregnancy or OCP use u Homozygotes: 50-100X increase lifetime risk thrombosis

31
Etiology Thrombophilia n Prothrombin G20210A Mutation u Higher plasma prothrombin concentrations, augmented thrombin generation u Heterozygotes: 2-3% Whites u Conflicting prevalence studies among RPL u Recent critical review suggests an association

32
Etiology Thrombophilia n Hyperhomocysteinemia polymorphisms u C677T thermolabile MTHFR F Heterozygous 10-20% Whites Normal or slightly elevated homocysteine Increased homocysteine when combined with B vitamin deficiencies F Homozygous 10% Whites Significantly increased homocysteine

33
Etiology Thrombophilia n Hyperhomocysteinemia polymorphisms u A1298C often occurs with thermolabile C677T F 33% frequency in Dutch population F Combined heterozygosity results in hyperhomocysteinemia and decreased plasma folate levels

34
Etiology Thrombophilia n Hyperhomocysteinemia polymorphisms u Significant association between hyperhomocysteinemia and RPL u ? Mechanism: interference in embryonic development through defective chorionic villous vascularization u Known association with later pregnancy-related complications

35
Etiology Thrombophilia n Anti-thrombin Deficiency u Physiologic inhibitor of coagulation F Type I: quantitative; decreased antigen and function; caused by gene deletions, nucleotide changes F Type II: qualitative; normal antigen levels, decreased function; caused by point mutations with single amino acid changes leading to a dysfunctional protein

36
Etiology Thrombophilia n Anti-thrombin Deficiency u Autosomal dominant u Prevalence Type I heterozygous carriers: 1/2000 – 1/5000 u Prevalence Type II heterozygous carriers: 3/1000 u Most thrombogenic of inherited thrombophilia: 20-50% lifetime risk u Associated increased risk stillbirth and fetal loss

37
Etiology Thrombophilia n Protein C Deficiency u Down-regulates coagulation cascade; deficiencies lead to unregulated fibrin formation u Autosomal dominant: > 160 mutations u Type I: quantitative u Type II: decreased function u Associated with 2 nd trimester losses

38
Etiology Thrombophilia n Protein S Deficiency u Principal cofactor of activated Protein C; mimics C deficiency: questionable association with pregnancy loss u Autosomal dominant: > 160 mutations: prevalence 0.15-0.8% general population; acquired forms in multiple disease states u Type I: quantitative u Type II: decreased function u Type III: low free protein, normal antigen, reduced activity

39
Etiology Luteal Phase Defect n Luteal phase defect is a controversial cause of RPL u Studies proving LPD as a cause of RPL lacking u No convincing studies showing LPD treatment improves pregnancy outcome Lee Semin Reprod Med 2000;18(4):433-40 u 80% of women with low midluteal progesterone proceed to term u 20% of fertile women have abnormal endometrial biopsies u P4 drops after meals & standing
: u 80% of women with low midluteal progesterone proceed to term u 20% of fertile women have abnormal endometrial biopsies u P4 drops after meals & standing")
40
Etiology Endocrine Factors n Poorly controlled diabetes n Overt hyperthyroidism n Overt hypothyroidism n No evidence that asymptomatic systemic endocrinologic or metabolic disorders are a cause of RPL

41
Etiology Autoimmune Factors n Certain autoimmune diseases are associated with pregnancy loss u Systemic lupus erythematosis F 1 st trimester loss: 10% risk F 2 nd and 3 rd trimester loss: 6% u Anti-phospholipid syndrome F 2 nd trimester loss: 38% Fausett & Branch Semin Reprod Med 2000;18(4):379-392
:")
42
Etiology Autoimmune Factors n Anti-phospholipid antibodies (aPL) u autoantibodies recognizing various combinations of phospholipids, phospholipid- binding proteins, or both n Anti-phospholipid syndrome (APS) - clinical association between aPL and syndrome of hypercoagulability Levine NEJM 2002;346:752-63
 u autoantibodies recognizing various combinations of phospholipids, phospholipid- binding proteins, or both n Anti-phospholipid syndrome (APS) - clinical association between aPL and syndrome of hypercoagulability Levine NEJM 2002;346:752-63")
43
Etiology Autoimmune Factors n APS diagnostic criteria: u Clinical features F Vascular thrombosis or F Loss of fetus at or after 10 weeks or F Preterm delivery at or before 34 weeks or F 3 or more consecutive SAB before 10 weeks

44
Etiology Autoimmune Factors n APS diagnostic criteria: u Laboratory features F Anti-cardiolipin (aCL) antibodies: IgG or IgM at moderate or high levels on 2 or more occasions at least 6 weeks apart F Lupus anticoagulant (LA) antibodies: detected on 2 or more occasions at least 6 weeks apart
 antibodies: IgG or IgM at moderate or high levels on 2 or more occasions at least 6 weeks apart F Lupus anticoagulant (LA) antibodies: detected on 2 or more occasions at least 6 weeks apart")
45
Etiology Autoimmune Factors n Other anti-phospholipid antibodies u Anti-phosphatidylserine: nearly always associated with APS, highly correlated to cardiolipin binding u Other antibodies have less correlation F No consistency among reported studies F No independence from aCL Fausett Semin Reprod Med 2000;18(4):379-92
:379-92")
46
Etiology Autoimmune Factors n Low levels of aPL are not associated with RPL n Assays for non-aCL aPL are not standardized n Studies thus far are contradictory

47
Etiology Autoimmune Factors n Other auto-antibodies NOT associated with RPL u Anti-nuclear antibodies may be more common among women with RPL but their presence or absence do not predict subsequent pregnancy outcome

48
Etiology Autoimmune Factors n Other auto-antibodies NOT associated with RPL u Anti-thyrogobulin and anti-thyroid peroxidase are markers of increased risk for pregnancy loss if identified early in pregnancy u Some small studies suggest a slight association in RPL; other larger studies do not u Subsequent pregnancy outcomes not affected

49
Etiology Alloimmune Factors n Immune response to non-self components of pregnancy u Cytotoxic antibodies u Absence of maternal blocking antibodies u Inappropriate sharing of HLA u Disturbances in natural killer cell function and distribution Porter Semin Reprod Med 2000;18(4):393-400
:")
50
Etiology Alloimmune Factors n Cytotoxic antibodies u Maternal response to paternal antigens u Present in normal pregnancies u More common in fertile couples than those with RPL u No bearing on subsequent pregnancy outcome

51
Etiology Alloimmune Factors n Blocking antibodies u Theory: maternal anti-fetal antibodies block maternal cell- mediated response; if absent, then fetal rejection occurs

52
Etiology Alloimmune Factors n Blocking antibodies u Not present in normal pregnancies, yet are often present in RPL u Detected by the non-specific mixed lymphocyte response assay

53
Etiology Alloimmune Factors n Blocking antibodies u Animal model: B-cell deficient (agammaglobulinemic) mice have normal pregnancy outcomes u Human agammaglobulinemics have successful pregnancies u Presence or absence not predictive of subsequent outcome
 mice have normal pregnancy outcomes u Human agammaglobulinemics have successful pregnancies u Presence or absence not predictive of subsequent outcome")
54
Etiology Alloimmune Factors n Parental HLA sharing u Theory: if parents are antigenically similar, mother is less likely to develop blocking antibodies u Studies contradictory: some show increased sharing in HLA-B and HLA-DR loci u Most show no associations

55
Etiology Alloimmune Factors n Natural killer cells Theory: CD56+ NK-like cells secrete a transforming growth factor- -like substance crucial to the maintenance of pregnancy u Present in endometria and early gestational decidua of women with RPL

56
Etiology Alloimmune Factors n Natural killer cells u Murine models show activation of NK cells increases the rate of abortion; depletion of NK cells has opposite effect u Human studies show no association of testing and successful pregnancy

57
Etiology Alloimmune Factors n T helper (Th1) immunodystrophism u Theory: aberrant or inappropriate Th1 stimulation may result in overproduction of cytokines that have deleterious effect on conceptus u Dichotomous Th1 versus Th2 cytokine profile associated with human pregnancy loss and success Hill Semin Reprod Med 2000;18(4):401-405
 immunodystrophism u Theory: aberrant or inappropriate Th1 stimulation may result in overproduction of cytokines that have deleterious effect on conceptus u Dichotomous Th1 versus Th2 cytokine profile associated with human pregnancy loss and success Hill Semin Reprod Med 2000;18(4):")
58
Etiology Male Factor n No significant difference in semen parameters among men whose partners have RPL compared to WHO standards and men fathering successful pregnancies n No difference in incidence of anti-sperm antibodies n Aside from cytogenetic abnormalities, male factor contribution to RPL unknown Hill ASRM 2002 Course 6 p.56 n DNA Fragmentation may result in early embryo loss Hum Reprod. 2006 Nov;21(11):2876-81; Check JH: Arch Androl. 2005 Mar-Apr;51(2):121-4
: ; Check JH: Arch Androl Mar-Apr;51(2):")
59
Etiology Male Factor n RPL males have higher incidence of sperm aneuploidy: u Oligoasthenoteratospermia 35-74% u Fertile donor sperm 4-7%

60
Etiology - Environmental Factors n Confirmed association u Ionizing irradiation u Organic solvents u Alcohol u Mercury u Lead Gardella & Hill Semin Reprod Med 2000;18(4):407-424 n Suspected association u Caffeine (> 300 mg/day) u Hyperthermia/fever u Cigarette smoking n Unknown association u Pesticides
: n Suspected association u Caffeine (> 300 mg/day) u Hyperthermia/fever u Cigarette smoking n Unknown association u Pesticides")
61
Etiology - Environmental Factors n Diagnostic x- rays n Air travel n Microwave ovens n Diagnostic ultrasounds n Electromagnetic fields n Video display terminals n Aspartame n Chocolate n Drinking water n BGH n Phytoestrogens n Phthalates n Herbicides n Hair dyes n Nail polish n Saccharin

62
Etiology - Idiopathic n More than 50% of couples with RPL have no explanation despite extensive evaluation(s) n Informative and sympathetic counseling appears to play an important role u 70% live birth rates reported in couples with unexplained RPL who undertake an untreated subsequent pregnancy Lee Semin Reprod Med 2000;18(4):433-40
 n Informative and sympathetic counseling appears to play an important role u 70% live birth rates reported in couples with unexplained RPL who undertake an untreated subsequent pregnancy Lee Semin Reprod Med 2000;18(4):433-40")
63
Evaluation n History u Pattern and trimester of pregnancy losses and whether a live embryo or fetus was present u Exposure to environmental,toxins or drugs u Known gynecological or obstetrical infections u Features associated with APS

64
Evaluation n History u Family history of RPL or syndrome associated with embryonic or fetal loss u Previous diagnostic tests and treatments

65
Evaluation n Physical u General physical exam u Pelvic exam

66
Evaluation n Tests u Saline Sonogram or hysteroscopy u Hysterosalpingogram u ?? Luteal phase endometrial biopsy; repeat in next cycle if abnormal u Placental FISH analysis u Parental karyotypes u Lupus anticoagulant u Anticardiolipin antibodies IgG and IgM

68
Evaluation n Tests u Antiphosphatidylserine antibody IgG and IgM u Platelet count u Thrombophilia mutations and functional assays u Thyroid stimulating hormone

69
Evaluation n Tests NOT useful u Other anti-phospholipid antibodies u ANA u Maternal anti-paternal leukocyte antibodies u Mixed lymphocyte maternal-paternal cell cultures u HLA genotyping u Mouse embryotoxicity assays u Immunophenotype panels (CD56, CD16) Hill ASRM 2002 Course 6 p.58-59
 Hill ASRM 2002 Course 6 p.58-59")
70
Treatment - Thrombophilia n For heritable or acquired thrombophilia: heparin anticoagulation n For bonafide APS, multiple studies support use of heparin and aspirin

71
Treatment - APS n Aspirin 81 mg po/day n Subcutaneous heparin 10K-20K units/day divided doses n Alternative: low-molecular- weight heparin 2500-5000 units/day single dose n Calcium supplementation

72
Treatment - Thrombophilia n For elevated homocysteinemia without thrombosis history u Supplementation with Vitamin B6, B12 and folic acid n Heparin anticoagulation for history of thrombosis or homozygous MTHFR mutation or pregnancy outcomes unresponsive to vitamin supplementation

73
Empiric Treatment n Use of aspirin alone attractive because of ease of use and relative safety profile, barring contraindication to low-dose aspirin use n Supporting data lacking

74
Treatment - Immunotherapy n “Blocking antibody” hypothesis u Paternal leukocyte immunization or desensitization F Efficacy disproven F May increase risk of loss F Potential adverse effects: transfusion reaction, immunization, infection, IUGR, GVH, thrombocytopenia

75
Treatment - Immunotherapy n “Blocking antibody” hypothesis u Intravenous immunoglobulin F Studies and meta-analyses show no benefit F Extremely expensive $7-14,000 F Side effects: headache, hypotension, nausea F Potential anaphylaxis in IgA deficient patients F Potential for prion disease transmission due to large pool of donors

76
Treatment - Immunotherapy n Progesterone called “nature’s immunosuppressant” due to inhibition of immune cells at maternal-fetal interface n No verification yet through RCT n Safe and inexpensive n Dose: 100 mg BID vaginal suppositories, beginning 3 days after ovulation

77
Supportive Treatment n 60-90% chance of pregnancy success with supportive care and... u Timed intercourse for genetic and idiopathic RPL u Surgery for selected anatomic factors u P 4 and/or ovulation induction for LPD

78
Supportive Treatment n 60-90% chance of pregnancy success with supportive care and... u Immunosuppresive P 4 for presumed alloimmune factors u Thyroid replacement for hypothyroidism u Appropriate anticoagulation for APS/thrombophilias

79
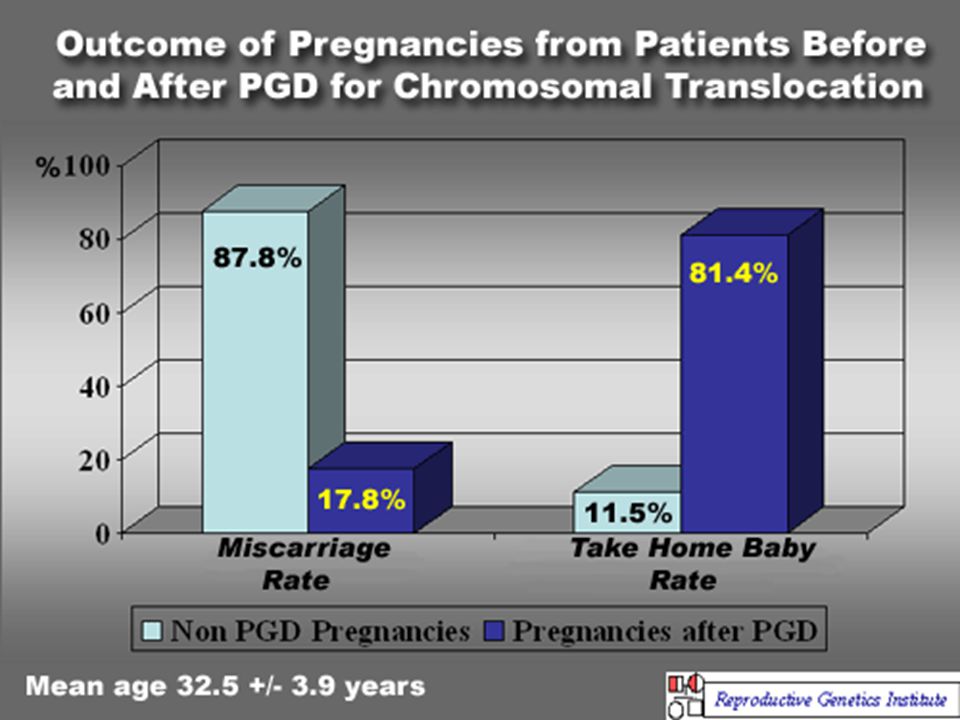
Management: Genetic Losses n Consider Preimplantation Genetic Diagnosis (PGD) u IVF u Day 3 blastomere biopsy (single cell) u FISH for most common aneuploidies or single gene defect (if probe available) u Blastocyst biopsy on day 5 allows detection of entire genome
 u IVF u Day 3 blastomere biopsy (single cell) u FISH for most common aneuploidies or single gene defect (if probe available) u Blastocyst biopsy on day 5 allows detection of entire genome")
80
Van Voorhis B. N Engl J Med 2007;356:379-386 The Process of IVF

81
Rebar, R. W. et al. N Engl J Med 2004;350:1603-1604 Embryos and Blastocysts during Assisted Reproduction (x20)
.")
82
Van Voorhis B. N Engl J Med 2007;356:379-386 Biopsy and Preimplantation Genetic Diagnosis of a 3-Day-Old (Eight-Cell) Embryo
 Embryo.")
83
Embryo Evaluation “omics” n GENomics u FISH – day 3 u Array CGH – day 5 u SNPs n TRANSCIPT omics u Gene transcription n PROTEomics u Proteins u Secretomics n METABOLomics u Metabolites u Amino Acids

84
Braude P. N Engl J Med 2006;355:541-543 In Vitro Fertilization and Preimplantation Genetic Haplotyping

85
Elias S. N Engl J Med 2001;345:1569-1571 Analysis by Comparative Genomic Hybridization of a Blastomere Obtained by Biopsy of a Six-to- Eight-Cell Embryo

86
Management: Genetic Losses n Drawbacks u Expense u Possibility of no transfer u 10-25% mosaicism and potential for misidentification u No large scale studies supporting benefit

87
Norwitz, E. R. et al. N Engl J Med 2001;345:1400-1408 Blastocyst Apposition and Adhesion

88
Norwitz, E. R. et al. N Engl J Med 2001;345:1400-1408 Blastocyst Implantation

89
Norwitz, E. R. et al. N Engl J Med 2001;345:1400-1408 Maintenance of Early Pregnancy

90
Summary n Early pregnancy loss is a frustrating entity for both patients and providers n Possibility of successful pregnancy outcome high, depending on maternal age and number of prior losses n Understanding the potential underlying mechanisms of loss along with empathetic supportive care decreases emotional stress and facilitates cost-effective evaluation and therapy

91
n Thank you all.

Similar presentations



 AND ITS RELATION TO COMBINED PARENTAL THROMBOPHILIC GENE MUTATIONS DOÇ. DR. A. GONCA İ M İ R YEN İ CESU CUMHUR İ YET ÜN.>")



 is produced by a shift in the balance between.>")












