Download presentation
Presentation is loading. Please wait.

1
Femur and Tibia Fractures
Kevin E. Coates, M.D., M.P.T.

2
Worker’s Compensation?

3
Femoral Neck Fractures
Epidemiology 250,000 Hip fractures annually Expected to double by 2050 At risk populations Elderly: poor balance&vision, osteoporosis, inactivity, medications, malnutrition incidence doubles with each decade beyond age 50 higher in white population Other factors: smokers, small body size, excessive caffeine & ETOH Young: high energy trauma

4
Classification I Valgus impacted or incomplete II Complete
Garden I Valgus impacted or incomplete II Complete Non-displaced III Complete Partial displacement IV Complete Full displacement ** Portends risk of AVN and Nonunion I II III IV

5
Treatment Goals Improve outcome over natural history
Minimize risks and avoid complications Return to pre-injury level of function Provide cost-effective treatment

6
Treatment Decision Making Variables
Patient Characteristics Young (arbitrary physiologic age < 65) High energy injuries Often multi-trauma Elderly Lower energy injury Comorbidities Pre-existing hip disease
 High energy injuries. Often multi-trauma. Elderly. Lower energy injury. Comorbidities. Pre-existing hip disease.")
7
Treatment Young Patients (Arbitrary physiologic age < 65)
Non-displaced fractures At risk for secondary displacement Urgent ORIF recommended Displaced fractures Patients native femoral head best AVN related to duration and degree of displacement Irreversible cell death after 6-12 hours Emergent ORIF recommended

8
Hemi ORIF THR

9
Non-displaced Fractures
ORIF standard of care Predictable healing Nonunion < 5% Minimal complications AVN < 8% Infection < 5% Relatively quick procedure Minimal blood loss

10
Displaced Fractures Hemiarthroplasty vs. ORIF
ORIF is an option in elderly Surgical emergency in young patients Complications Nonunion % AVN 15 – 33% AVN related to displacement Early ORIF no benefit Loss of reduction / fixation failure 16%

11
Displaced Fractures Hemiarthroplasty vs. ORIF
Hemi associated with Lower reoperation rate (6-18% vs %) Improved functional scores Less pain More cost-effective Slightly increased short term mortality
 Improved functional scores. Less pain. More cost-effective. Slightly increased short term mortality.")
12
Femoral Neck Nonunion Definition: not healed by one year
0-5% in Non-displaced fractures 9-35% in Displaced fractures Increased incidence with Posterior comminution Initial displacement Inadequate reduction Non-compressive fixation

13
Femoral Neck Fractures Complications
Failure of Fixation Inadequate / unstable reduction Poor bone quality Poor choice of implant Treatment Elderly: Arthroplasty Young: Repeat ORIF Valgus-producing osteotmy Arthroplasty

14
Femoral Neck Fractures Complications
Post-traumatic arthrosis Joint penetration with hardware AVN related Blood Transfusions THR > Hemi > ORIF Increased rate of post-op infection DVT / PE Multiple prophylactic regimens exist One-year mortality 14-50%

15
Intertrochanteric Femur Fractures
Extra-capsular femoral neck To inferior border of the lesser trochanter

16
Etiology Osteoperosis Low energy fall Common High Energy Rare

17
Radiographs Plain Films AP Pelvis Cross Table Lateral

18
Goals of Treatment Obtain a Stable Reduction Internal Fixation
Good Position Mechanically Adequate Permit Immediate Transfers & Early Ambulation

19
Rehabilitation Mobilize Weight Bearing As Tolerated
Cognitive Intact Patients Auto Protect Unstable Fractures = Less WB Stable Fractures = More WB No 6 weeks Post op

20
Femoral Shaft Fractures
Common injury due to major violent trauma 1 femur fracture/ 10,000 people More common in people < 25 yo or >65 yo Femur fracture leads to reduced activity for 107 days Motor vehicle, motorcycle, auto-pedestrian, aircraft, and gunshot wound accidents are most frequent causes

21
Femur Fracture Management
Initial traction with portable traction splint or transosseous pin and balanced suspension Evaluation of knee to determine pin placement Timing of surgery is dependent on: Resuscitation of patient Other injuries - abdomen, chest, brain Isolated femur fracture

22
Femur Fracture Management
Antegrade nailing is still the gold standard Antegrade nailing problems: Varus alignment of proximal fractures Trendelenburg gait Can be difficult with obese or multiply injured patients

23
Femur Fracture Management
Retrograde nailing has advantages Easier in large patients to find starting point Better for combined fracture patterns (ipsilateral femoral neck, tibia,acetabulum) Retrograde nailing has its problems: Intra-articular starting point
 Retrograde nailing has its problems: Intra-articular starting point.")
24
Femur Fracture Complications
Hardware failure Nonunion - less than 1-2% Malunion - shortening, malrotation, angulation Infection Neurologic, vascular injury Heterotopic ossification

25
Ipsilateral Femoral Neck & Shaft Fractures
Optimum fixation of the femoral neck should be the goal Varus malunion of the femoral neck is not uncommon, osteotomies can lead to poor results Vertical femoral neck fracture seen in 26-59% of cases Rate of avascular necrosis is low, 3%, even when missed

26
Tibial Plateau Fractures
Mechanism of Injury Mean age in most series of tibial plateau fractures is about 55 years Large percentage over age 60 Elderly population is increasing in numbers

27
Mechanism of Injury Mechanism of injury is fall from standing height in most patients MVA is increasing as % of fractures Most common fracture pattern is split- depressed fracture of lateral tibial plateau (80% of fractures)
")
28
Physical Exam Neurologic exam Vascular exam peroneal nerve!
popliteal artery and medial plateau injuries beware the of the knee dislocation posing as a fracture beware of posteriorly displaced fracture fragments ABI <0.9 urgent arterial study

29
Physical Exam Compartment syndrome KNEE STABILITY
varus/valgus in full extension may require premedication aspiration of knee effusion/hematoma replace with lidocaine+marcaine

30
Evaluation of Soft Tissues
Proximal and distal tibia subcutaneous Soft tissue remains compromised for at least 7 days Early ORIF risks wound sloughexposed hardware

31
AP and Lateral Radiographs

32
Pre-traction

33
Post-traction

34
Computed Tomography Indications
Fracture in an active patient for which you are considering nonsurgical care Complex fracture To aid surgical planning of approach, technique, screw position, etc.

35
Computed Tomography

36
Computed Tomography

37
Classification: Schatzker
III II

38
Classification: Schatzker
IV VI V

39
Surgical Indicatons Open Fracture – I&D, spanning ex-fix
Extensive soft tissue contusion – spanning ex-fix Closed fracture Varus/valgus instability of the knee Varus or valgus tilt of the proximal tibia Meniscal injury/previous mensicectomy Articular displacement or gapping???

40
Angular Malalignment of the Proximal Tibia
Incidence of arthrosis: Valgus < 10o 14% Valgus > 10o 79% Any amount of varus angulation was bad Independent of articular congruity

41
Meniscectomy Higher rate of arthrosis in patients who had undergone meniscectomy at surgery 70% arthrosis in patients who had undergone meniscectomy results independent of the amount of articular incongruity

42
Postoperative Management
Immediate PROM/AROM of knee Routine Pin site care (if ex-fix) TDWB for 8-12 weeks
 TDWB for 8-12 weeks.")
43
Outcomes Outcome depends on: Varus valgus stability of the knee
Varus/valgus alignment of the proximal tibia Presence of an intact meniscus Articular congruity (to a lesser extent)
")
44
Treatment Goals Focus on restoring stability and proximal tibial alignment to the knee, rather than restoring anatomic alignment of the articular surface at all costs Use minimally invasive techniques, when possible Other techniques are preferable to hybrid ex-fix MOVE THE KNEE EARLY IN ALL PATIENTS!

45
Tibial Shaft Fractures
Mechanism of Injury Can occur in lower energy, torsional type injury (eg, skiing) More common with higher energy direct force (eg car bumper)
 More common with higher energy direct force (eg car bumper)")
46
Physical Exam Soft tissue injury with high-energy crush mechanism may take several days to fully declare itself Repeated exam often necessary to follow compartment swelling

47
Associated Injuries Up to 30% of patients with tibial fractures have multiple injuries* Fracture of the ipsilateral fibula common Ligamentous injury of knee common in high energy tibia fractures

48
Associated Injuries Ipsilateral femur fx, so called “floating knee”, seen in high energy injuries Neuro/vascular injury less common than in proximal tibia fx or knee dislocation Foot and ankle injury should be assessed on physical exam and x-ray if needed

49
Compartment Syndrome 5-15% History of high energy or crush injury

50
Nerve is the Tissue most Sensitive to Ischemia
PAIN first Symptom PAIN with Passive Stretch first Sign

51
Each Compartment has Specific Innervation
Ant Comp Deep- - Peroneal Lateral -Sup Peroneal N. Deep Post. - Tibial N. Sup Post. - Sural N.

52
Advantages of IM Nail Advantages include less malunion and less shortening than closed treatment or ex-fix Earlier weight bearing may be allowed with insertion large nail

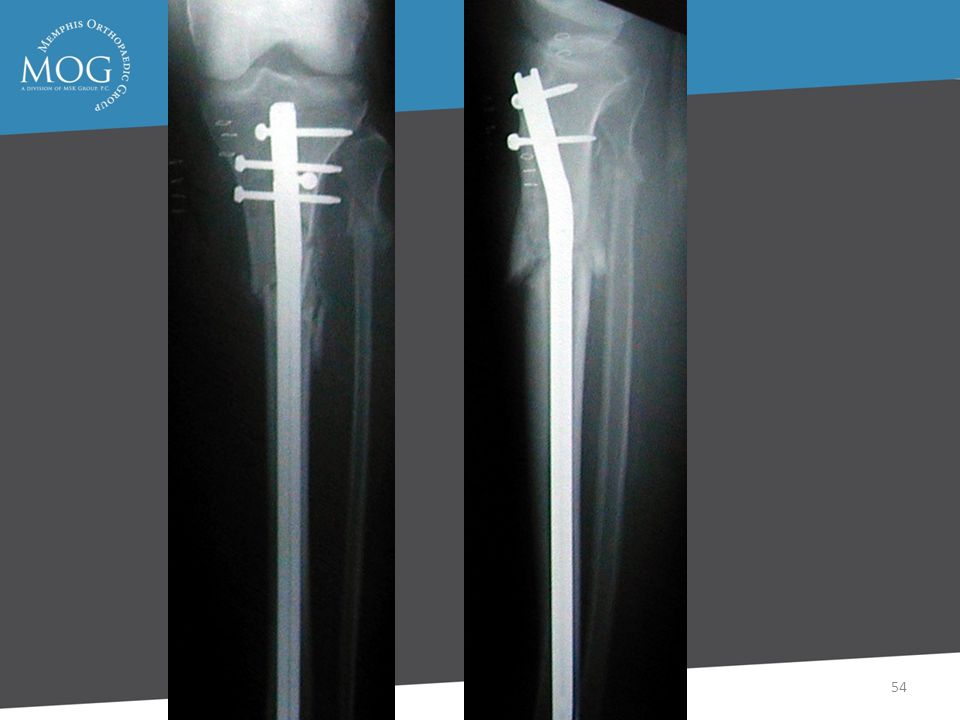
53
Proximal Fractrues are technically more challenging
Prone to Valgus & Pro-curvatum deformities

55
Complications Infection 1-5% Union >90% Knee Pain Common

56
Knee Pain Severe 9% Kneeling 92% Moderate 22% Running 57% Mild 68%
Rest 37%

57
Nail Removal Resolved 27% No - 20%

58
Disadvantages of IM Nail
Disadvantages include anterior knee pain (up to 56.2% *), risk of infection
, risk of infection.")
59
External Fixator External fixation generally reserved for open tibia fractures or periarticular fractures

60
Disadvantages of External Fixator
Increased incidence of malunion compared to IM nail Risk of pin tract infection, cellulitis

61
Outcomes of External Fixation
95% union rate has been reported for group of closed and open tibia fractures, but 20% malunion rate* Most common complications are pin track infections and malunion Loss of reduction associated with removing frame prior to union

62
Open Tibia Fractures Open fractures of the tibia are more common than in any other long bone Rate of tibial diaphysis fractures reported from 2 per 1000 population to 2 per 10,000 and of these approximately one fourth are open tibia fractures*

63
Associated Injuries Neurovascular structures require repeated assessment Foot fractures also common Compartment syndrome must be looked for

64
Gustilo and Anderson Classification
Grade 1- skin opening of 1cm or less, minimal muscle contusion, usually inside out mechanism Grade 2- skin laceration 1-10cm, extensive soft tissue damage Grade 3a- extensive soft tissue laceration(10cm) but adequate bone coverage Grade 3b- extensive soft tissue injury with periosteal stripping requiring flap advancement or free flap Grade 3c- vascular injury requiring repair
 but adequate bone coverage. Grade 3b- extensive soft tissue injury with periosteal stripping requiring flap advancement or free flap. Grade 3c- vascular injury requiring repair.")
65
Objectives Prevent Sepsis Union Function

66
Soft Tissue Coverage Definitive coverage should be performed within 7 days if possible Most type 1 wounds will heal by secondary intent or can be closed primarily Delayed primary closure usually feasible for type 2 and type 3a fractures

67
Soft Tissue Coverage Type 3b fractures require either local advancement or rotation flap, split-thickness skin graft, or free flap STSG suitable for coverage of large defects with underlying viable muscle

68
Soft Tissue Coverage Proximal third tibia fractures can be covered with gastrocnemius rotation flap Middle third tibia fractures can be covered with soleus rotation flap Distal third fractures usually require free flap for coverage

69
Amputation In general amputation performed when limb salvage poses significant risk to patient survival, when functional result would be better with a prosthesis, and when duration and course of treatment would cause intolerable psychological disturbance

70
Complications Nonunion Malunion Infection- deep and superficial
Compartment syndrome Fatigue fractures Hardware failure

71
Nonunion Time limits vary from 6 months to one year
Fracture shows no radiologic progress toward union over 3 month period Important to rule out infection

72
Malunion In general varus malunion more of a problem than valgus
For symptomatic patients with significant deformity treatment is osteotomy

73
Deep Infection Often presents with increasing pain, wound drainage, or sinus formation Treatment involves debridement, stabilization (often with ex-fix), coverage with healthy tissue including muscle flap if needed, IV antibiotics, delayed bone graft of defect if needed
, coverage with healthy tissue including muscle flap if needed, IV antibiotics, delayed bone graft of defect if needed.")
74
Superficial Infection
Most superficial infections respond to elevation of extremity and appropriate antibiotics (typically gram + cocci coverage) If uncertain whether infection extends deeper and/or it fails to respond to antibiotic treatment, then surgical debridement with tissue cultures necessary
 If uncertain whether infection extends deeper and/or it fails to respond to antibiotic treatment, then surgical debridement with tissue cultures necessary.")
75
Hardware Failure Usually due to delayed union or nonunion
Important to rule out infection as cause of delayed healing Treatment depends on type of failure- plate or nail breakage requires revision, whereas breakage of locking screw in nail may not require operative intervention

76
Outcomes Outcome most affected by severity of soft tissue and neurovascular injury Most studies show major change in results between type 3a and 3b/c fractures For type 3b and 3c fractures early soft tissue coverage gives best results

77
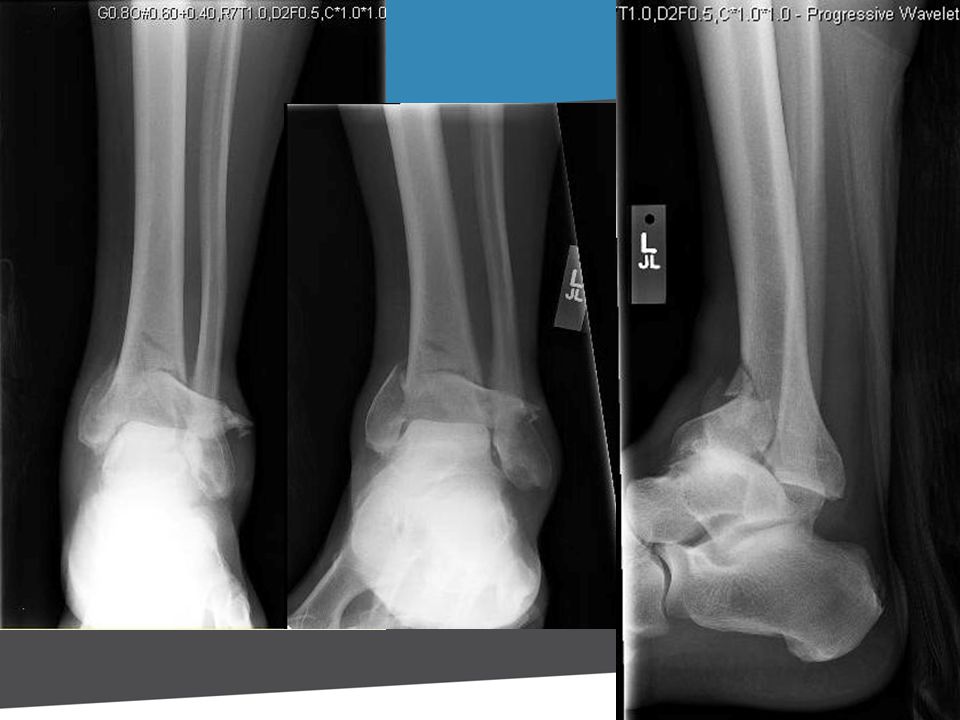
Tibial Plafond Fractures
Terrible Injuries “Excellent Results” rarely achieved Fair to Good Results are the Norm Outcomes are Impossible to Predict Avoid Treatment Complications

78
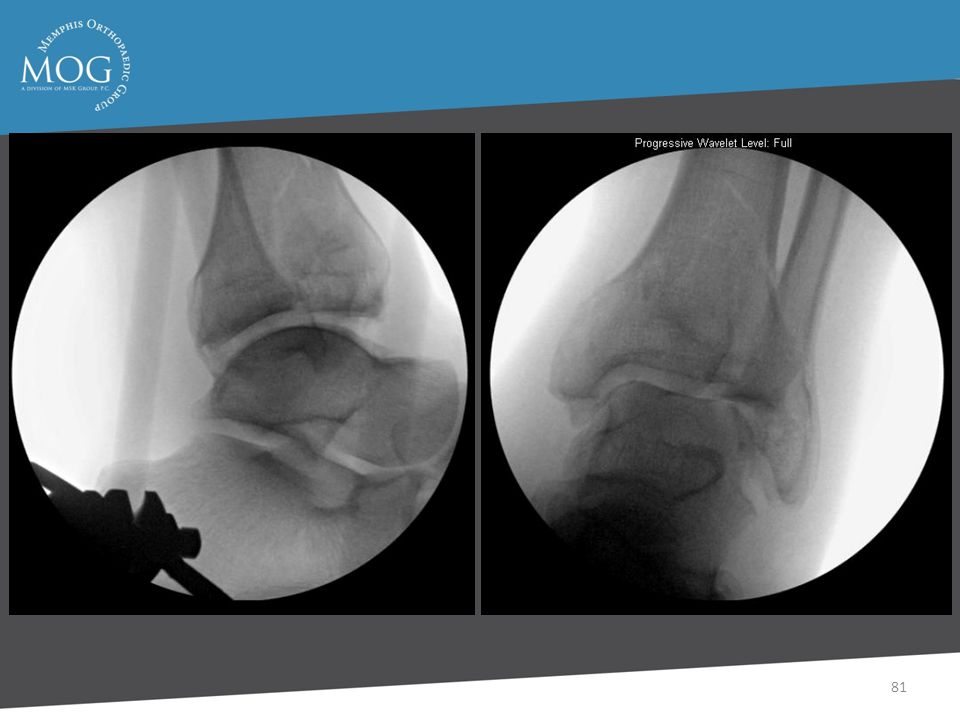
Treatment Principles Delay Until Definitive Surgery
Spanning External Fixation Pecutaneous and Limited Approaches Plating Fibula

85
Surgical Delay with External Fixation
Maintains Length and Aligment Better Imaging Studies Allows Mobilization Pre-Operative Planning Allows Soft Tissue Recovery

86
Plating of Fibula Fracture
Fibular length Articular reconstruction Early motion

87
Outcomes Most Have Some Pain Most Return to Work
Detectable Arthritis in 50%

88
Outcomes - Pain 50% Minimal 35% Pain with WB 15% Continuous

89
Long Term Outcome 5 - 11 Years Most Have Some Degree of Ankle Pain
Most Cannot Run or Play Sports 70% with Moderate to Severe Arthritis Most Rate Their Outcome as Good

90
Summary Bad Injuries with Unpredictable Outcomes
Complications in 10% or Less Results Generally not Great but not Bad if no Complications

Similar presentations









, F.R.C.S.(C )>")

Extension of traumatized wound to allow identification of zone of injury 2)Detection & removal of foreign material, especially.>")











