Download presentation
Presentation is loading. Please wait.

1
Acute pulmonary embolism review of diagnostic modalities DR
Acute pulmonary embolism review of diagnostic modalities DR.BASHAR REDA orthopedic demonstrator

3
Objectives -Definitions -pathophysiology -prognosis -risk factors -clinical presentation -diagnistic tests

4
Introduction Acute pulmonary embolism (PE) is a common and often fatal disease. Mortality can be reduced by prompt diagnosis and therapy. Unfortunately, the clinical presentation of PE is variable and nonspecific, making accurate diagnosis difficult.
 is a common and often fatal disease. Mortality can be reduced by prompt diagnosis and therapy. Unfortunately, the clinical presentation of PE is variable and nonspecific, making accurate diagnosis difficult.")
5
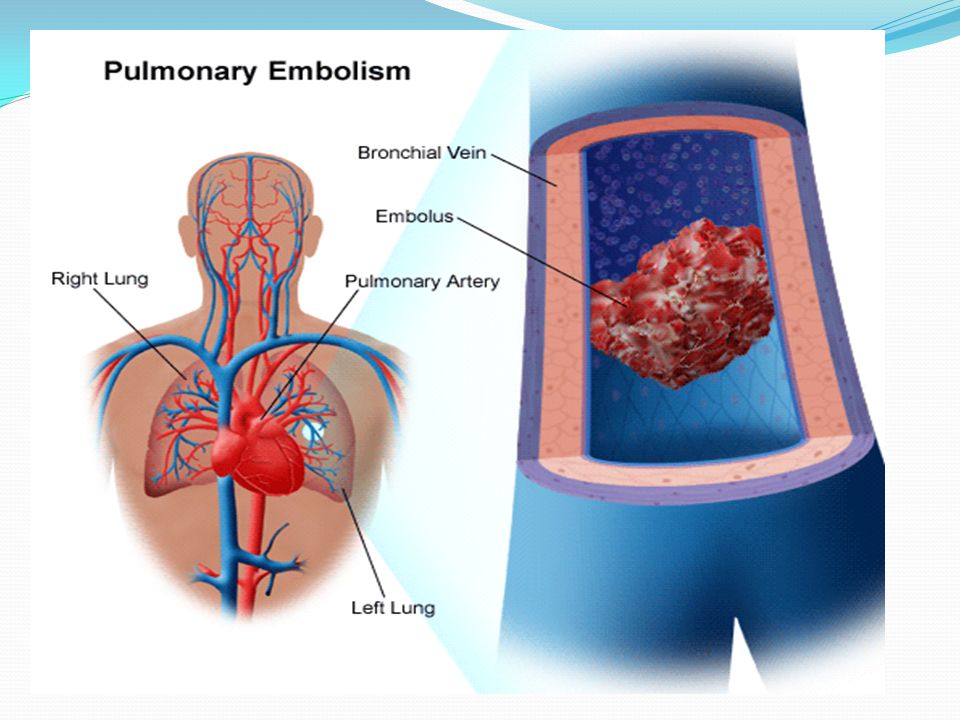
Definition PE refers to obstruction of the pulmonary artery or one of its branches by material (eg, thrombus, tumor, air, or fat ). PE can be classified as acute or chronic. Patients with acute PE typically develop symptoms and signs immediately after obstruction of pulmonary vessels. In contrast, patients with chronic PE tend to develop slowly progressive dyspnea over a period of years due to pulmonary hypertension.
. PE can be classified as acute or chronic. Patients with acute PE typically develop symptoms and signs immediately after obstruction of pulmonary vessels. In contrast, patients with chronic PE tend to develop slowly progressive dyspnea over a period of years due to pulmonary hypertension.")
6
Definition Massive PE causes hypotension, defined as a systolic blood pressure <90 mmHg or a drop in systolic blood pressure of ≥40 mmHg from baseline for a period >15 minutes. It should be suspected anytime there is hypotension accompanied by an elevated central venous pressure (or neck vein distension)
")
7
pathophysiology Most PE arise from thrombi in the deep venous system of the lower extremities. However, they may also originate in the right heart or the pelvic, renal, or upper extremity veins. Iliofemoral veins are the source of most clinically recognized PE After traveling to the lung, large thrombi may lodge at the bifurcation of the main pulmonary artery or the lobar branches and cause hemodynamic compromise. Smaller thrombi continue traveling distally and are more likely to produce pleuritic chest pain, presumably by initiating an inflammatory response adjacent to the parietal pleura. Only about 10 percent of emboli cause pulmonary infarction

8
pathophysiology Impaired gas exchange due to PE cannot be explained solely on the basis of mechanical obstruction of the vascular bed and alterations in the ventilation to perfusion ratio. Gas exchange abnormalities are also related to the release of inflammatory mediators, resulting in surfactant dysfunction, atelectasis, and functional intrapulmonary shunting Hypotension is due to diminished cardiac output (CO) which results from increased pulmonary vascular resistance (PVR) impeding right ventricular outflow and reducing left ventricular preload
 which results from increased pulmonary vascular resistance (PVR) impeding right ventricular outflow and reducing left ventricular preload")
9
Prognostic factors PE is associated with a mortality rate of approximately 30 percent without treatment. However, accurate diagnosis followed by effective anticoagulant therapy decreases the mortality rate to 2 to 8 percent Prognostic factors determining the mortality and morbidity of PE includes:

10
RV dysfunction RV dysfunction due to PE results in increased PE-related mortality. This was illustrated by a meta-analysis of seven studies (3395 normotensive or hypotensive patients with PE), which found that RV dysfunction was associated with a two-fold increase in PE-related mortality(determined ehocardiographically) RV dysfunction may also predict recurrent PE or DVT
, which found that RV dysfunction was associated with a two-fold increase in PE-related mortality(determined ehocardiographically) RV dysfunction may also predict recurrent PE or DVT")
11
Brain natriuretic peptides
An elevated brain natriuretic peptide (BNP) or N-terminal pro-brain natriuretic peptide (NT-proBNP) predicts RV dysfunction and mortality In an observational study of 73 patients diagnosed with acute PE, serum BNP levels >90 pg/mL were associated with cardiopulmonary resuscitation, mechanical ventilation, vasopressor therapy, thrombolysis, and embolectomy, as well as death . Serum BNP levels <50 pg/mL was associated with a benign clinical course.
 or N-terminal pro-brain natriuretic peptide (NT-proBNP) predicts RV dysfunction and mortality In an observational study of 73 patients diagnosed with acute PE, serum BNP levels >90 pg/mL were associated with cardiopulmonary resuscitation, mechanical ventilation, vasopressor therapy, thrombolysis, and embolectomy, as well as death . Serum BNP levels <50 pg/mL was associated with a benign clinical course.")
12
RV thrombus Patients with PE and a right ventricular (RV) thrombus have a higher short term and long term mortality than patients without an RV thrombus
 thrombus have a higher short term and long term mortality than patients without an RV thrombus.")
13
Serum troponins Elevated serum troponin levels identify patients with PE who are at increased risk for death. In a meta-analysis of 20 observational studies (1985 patients), an elevated troponin I or troponin T level was associated with an increased risk of short-term mortality or death due to PE Troponin levels can be combined with BNP levels to derive more precise prognostic information
, an elevated troponin I or troponin T level was associated with an increased risk of short-term mortality or death due to PE. Troponin levels can be combined with BNP levels to derive more precise prognostic information.")
14
Risk factors These include immobilization, surgery within the last three months, stroke, paresis, paralysis, history of venous thromboembolism, malignancy, central venous instrumentation within the last three months, and chronic heart disease .Additional risk factors identified in women include obesity (BMI ≥29 kg/m2), heavy cigarette smoking (>25 cigarettes per day), and hypertension .
, heavy cigarette smoking (>25 cigarettes per day), and hypertension .")
15
Clinical presentation
Specific symptoms and signs are not helpful diagnostically because their frequency is similar among patients with and without PE Symptoms : -dyspnea at rest or with exertion (73 percent) -pleurtic chest pain (44 percent ) -cough (34 percent) -orthopnea (28 percent), -calf or thigh pain (44 percent) -calf or thigh swelling (41 percent) -wheezing (21 percent)
 -pleurtic chest pain (44 percent ) -cough (34 percent) -orthopnea (28 percent), -calf or thigh pain (44 percent) -calf or thigh swelling (41 percent) -wheezing (21 percent)")
16
cont’d Signs : -tachypnea (54 percent) -tachecardia (24 percent) -rales (18 percent) -decreased breath sounds (17 percent) -an accentuated pulmonic component of the second heart sound (15 percent) -jugular venous distension (14 percent) -Circulatory collapse (8 percent)
 -tachecardia (24 percent) -rales (18 percent) -decreased breath sounds (17 percent) -an accentuated pulmonic component of the second heart sound (15 percent) -jugular venous distension (14 percent) -Circulatory collapse (8 percent)")
17
Diagnostic tests Many of the symptoms and signs detected in patients with acute PE are also common among patients without PE, emphasizing the need for additional evaluation. These include lab tests and imaging studies

18
Arterial blood gases Arterial blood gas (ABG) measurements and pulse oximetry have a limited role in diagnosing PE .ABGs usually reveal hypoxemia, hypocapnia, and respiratory alkalosis. Patients with room air pulse oximetry readings <95 percent at the time of diagnosis are at increased risk of in-hospital complications, including respiratory failure, cardiogenic shock, and death The typical arterial blood gas findings are not always seen. As an example, massive PE with hypotension and respiratory collapse can cause hypercapnia and a combined respiratory and metabolic acidosis (the latter due to lactic acidosis). In addition, hypoxemia can be minimal or absent
 measurements and pulse oximetry have a limited role in diagnosing PE .ABGs usually reveal hypoxemia, hypocapnia, and respiratory alkalosis. Patients with room air pulse oximetry readings <95 percent at the time of diagnosis are at increased risk of in-hospital complications, including respiratory failure, cardiogenic shock, and death The typical arterial blood gas findings are not always seen. As an example, massive PE with hypotension and respiratory collapse can cause hypercapnia and a combined respiratory and metabolic acidosis (the latter due to lactic acidosis). In addition, hypoxemia can be minimal or absent")
19
Brain natriuretic peptide (BNP)
Brain natriuretic peptide (BNP) levels are typically greater in patients with PE compared to patients without PE; however, many patients with PE do not have elevated BNP levels (ie, it is insensitive) and there are many alternative causes of an elevated BNP level (ie, it is nonspecific) .These features limit its usefulness as a diagnostic test. BNP and NT-proBNP may have a prognostic role in PE. Their elevation is associated with increased rate of complication and prolonged hospitalization
 levels are typically greater in patients with PE compared to patients without PE; however, many patients with PE do not have elevated BNP levels (ie, it is insensitive) and there are many alternative causes of an elevated BNP level (ie, it is nonspecific) .These features limit its usefulness as a diagnostic test. BNP and NT-proBNP may have a prognostic role in PE. Their elevation is associated with increased rate of complication and prolonged hospitalization")
20
troponins Serum troponin I and troponin T are elevated in 30 to 50 percent of patients who have a moderate to large pulmonary embolism .The presumed mechanism is acute right heart overload .The troponin elevations usually resolve within 40 hours following pulmonary embolism, in contrast to the more prolonged elevation after acute myocardial injury Serum troponins are not useful for diagnosis, but are associated with adverse outcomes. This suggests that they may be useful for prognosis.

21
ECG Electrocardiogram (ECG) abnormalities exist in many patients with PE who do not have preexisting cardiovascular disease. However, ECG abnormalities are also common in patients without PE, limiting the diagnostic usefulness of the ECG Electrocardiographic abnormalities historically considered to be suggestive of PE (S1Q3T3 pattern, right ventricular strain, new incomplete right bundle branch block) . The following ECG abnormalities are associated with a poor prognosis : Atrial arrhythmias Right bundle branch block Inferior Q-waves Precordial T-wave inversion and ST-segment changes
 abnormalities exist in many patients with PE who do not have preexisting cardiovascular disease. However, ECG abnormalities are also common in patients without PE, limiting the diagnostic usefulness of the ECG Electrocardiographic abnormalities historically considered to be suggestive of PE (S1Q3T3 pattern, right ventricular strain, new incomplete right bundle branch block) . The following ECG abnormalities are associated with a poor prognosis : Atrial arrhythmias Right bundle branch block Inferior Q-waves Precordial T-wave inversion and ST-segment changes")
22
Chest x-ray Radiographic abnormalities are common in patients with PE; however, they are not helpful diagnostically because they are similarly common in patients without PE. Findings include : atelectasis , lung parenchymal changes and pleural effusion Only 12 percent of the chest radiographs in patients with PE were interpreted as normal.

23
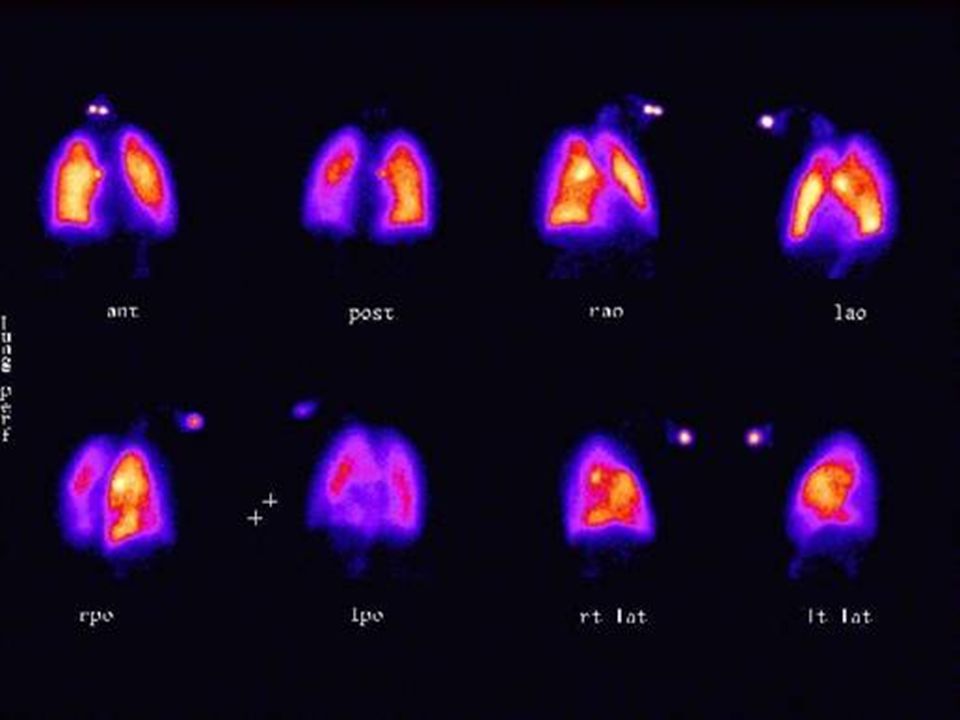
V/Q scan Diagnostic accuracy was greatest when the V/Q scan was combined with clinical probability, (Well’s score) -Patients with high clinical probability of PE and a high-probability V/Q scan had a 95 percent likelihood of having PE -Patients with low clinical probability of PE and a low-probability V/Q scan had only a 4 percent likelihood of having PE -A normal V/Q scan virtually excluded PE
 -Patients with high clinical probability of PE and a high-probability V/Q scan had a 95 percent likelihood of having PE -Patients with low clinical probability of PE and a low-probability V/Q scan had only a 4 percent likelihood of having PE -A normal V/Q scan virtually excluded PE")
25
ultrasound Lower extremity venous ultrasound is sometimes performed during the diagnostic evaluation of PE. The rationale is that venous thrombosis detected by ultrasound is treated similar to confirmed PE,However, there are draw backs to this approach: -False positive venous ultrasound studies (3 percent in one report) will result in the anticoagulation of some patients who do not have DVT or PE, thus subjecting them to unnecessary risk -Many patients with PE are likely to be missed. In one report, only 29 percent of patients with PE (determined by V/Q scan or pulmonary angiogram) had venous thrombosis detected by compression ultrasound
 will result in the anticoagulation of some patients who do not have DVT or PE, thus subjecting them to unnecessary risk -Many patients with PE are likely to be missed. In one report, only 29 percent of patients with PE (determined by V/Q scan or pulmonary angiogram) had venous thrombosis detected by compression ultrasound")
26
Cont’d Studies have shown that Imaging the entire venous system (ie, complete lower extremity venous ultrasound), including calf veins, or if six serial lower extremity venous ultrasounds were performed over a two week period increase the accuracy of the ultrasound testing in detecting PE.
, including calf veins, or if six serial lower extremity venous ultrasounds were performed over a two week period increase the accuracy of the ultrasound testing in detecting PE.")
27
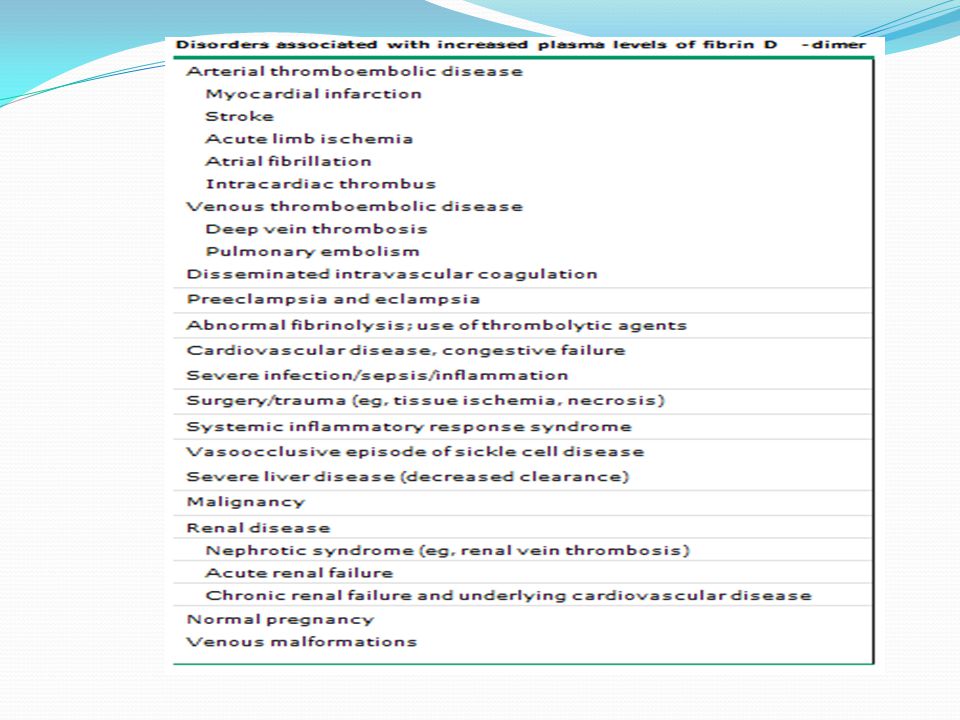
D-dimer Use of D-dimer assays for the diagnosis of PE has been extensively studied and is best characterized as having good sensitivity and poor specificity . Abnormal D-dimer levels are common among hospitalized patients, especially those with malignancy or recent surgery

29
angiography Pulmonary angiography is the definitive diagnostic technique or "gold standard" in the diagnosis of acute PE. It is performed by injecting contrast into a pulmonary artery branch after percutaneous catheterization, usually via the femoral vein A negative pulmonary angiogram excludes clinically relevant PE Pulmonary angiography is generally safe and well tolerated in the absence of hemodynamic instability caused by acute, severe pulmonary hypertension . Mortality of the procedure is less than 2 percent. Morbidity occurs in approximately 5 percent of patients, and is usually related to catheter insertion, contrast reactions, cardiac arrhythmia, or respiratory insufficiency

30
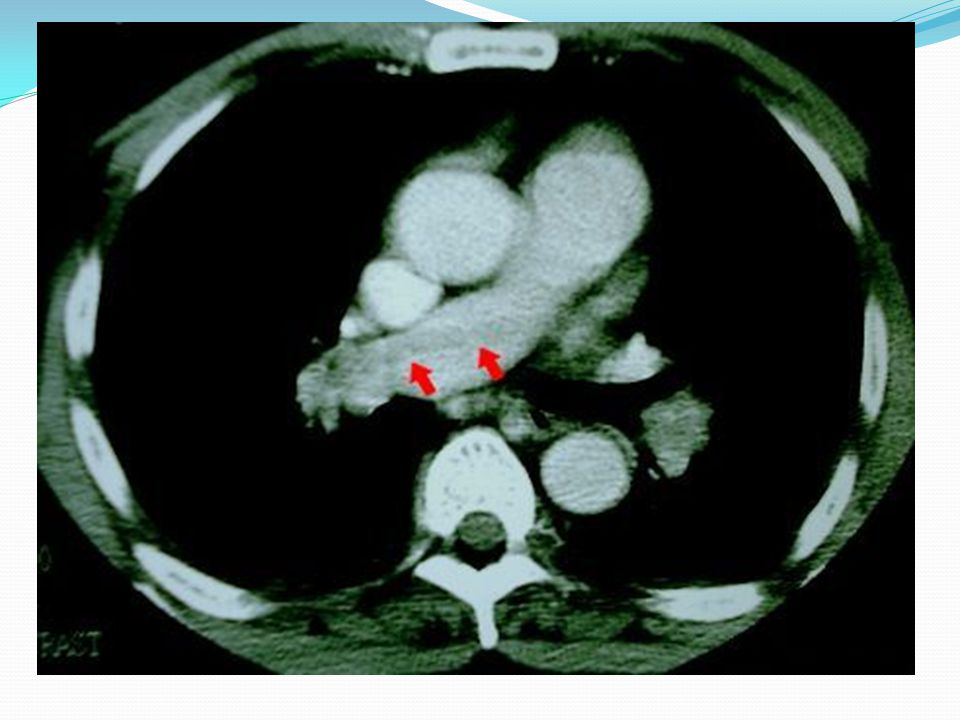
Spiral ct scan Due to its widespread availability, spiral (helical) CT scanning with intravenous contrast (ie, CT pulmonary angiography or CT-PA) is being used increasingly as a diagnostic modality for patients with suspected PE The largest study to date was PIOPED II (824 patients) had showed : 83 percent of patients with PE had a positive CT-PA (ie, sensitivity). Conversely, 96 percent of patients without PE had a negative CT-PA (ie, specificity). One of the most commonly cited benefits of CT-PA is the ability to detect alternative pulmonary abnormalities that may explain the patient's clinical presentation also its rapidity and safety .
 CT scanning with intravenous contrast (ie, CT pulmonary angiography or CT-PA) is being used increasingly as a diagnostic modality for patients with suspected PE The largest study to date was PIOPED II (824 patients) had showed : 83 percent of patients with PE had a positive CT-PA (ie, sensitivity). Conversely, 96 percent of patients without PE had a negative CT-PA (ie, specificity). One of the most commonly cited benefits of CT-PA is the ability to detect alternative pulmonary abnormalities that may explain the patient s clinical presentation also its rapidity and safety .")
32
echocardiography Only 30 to 40 percent of patients with PE have echocardiographic abnormalities suggestive of acute PE including : -Increased right ventricular (RV) size -Decreased RV function -Tricuspid regurgitation -RV thrombus -Regional wall motion abnormalities The presence of RV dysfunction or an RV thrombus detected by echocardiography has prognostic implications
 size -Decreased RV function -Tricuspid regurgitation -RV thrombus -Regional wall motion abnormalities The presence of RV dysfunction or an RV thrombus detected by echocardiography has prognostic implications")
33
Well’s criteria Is a clinical score applied to determine if PE is unlikely (score <4) or likely (score >4)
 or likely (score >4)")
34
algorithm Numerous algorithms using various combinations of diagnostic tests have been devised , this algorithm is one suggestion

35
CT experienced institutions

36
CT inexperienced institutions

37
Thank you

Similar presentations