Download presentation
Presentation is loading. Please wait.

1
Thin Blood Department of Clinical Toxicology and Pharmacology Newcastle Mater Hospital

2
Case 1 37 year old male Presented to JHH Emergency Department Drug overdose –120 mg warfarin Activated charcoal Bloods sent Transfer to MMH after d/w Toxicology

3
Background Precipitating incident : –Brother suicided recently –Planned overdose for 2 days Psychiatric background : –No previous deliberate self harm –Amphetamine dependence

4
Medical History Endocarditis 2º to IVDU Valve replacement x 2 –mitral and aortic valve replacements –St. Judes : bileaflet –Complicated by AMI and CVA Lifelong anticoagulation Nil attendance with cardiology follow up

5
On arrival HR 80 BP 144/88 Temp 36.2 Alert and Cooperative No bruising or evidence of bleeding Dysarthric with mild cognitive impairment HSD, metallic sounds No signs of cardiac failure

6
Initial Management INR 2.0 Appropriate Management ? –FFP –Vitamin K

7
Initial Management Haematology consult –4 units FFP –10 mg vitamin K IVI Neurological observation 2-3 daily INR

8
INR Results Vitamin K 10 mg IVI 4 Units FFP

9
INR Results Heparin 5,000 U Infusion 1000 U/hr

10
INR Results Heparin ceased Warfarin recommenced, normal dose 5 mg/d

11
Time course of INR FFP Vit K HeparinHeparin Ceased Warfarin Restarted

12
Optimal Management - Issues Perfect dose of vitamin K ! Normalised INR with FFP; then therapeutic Required heparinisation for 2 days No active bleeding

13
Case 2 43 year old male Drug overdose 1 hour previously –25 x 5 mg warfarin –40 x 5 mg oxycodone Multiple lacerations to left forearm Vomited in transit to MMH

14
Background Precipitating incident : –Argument with wife, asked to leave Psychiatric background : –Narcotic dependence; 7 year history –No previous deliberate self harm

15
Medical History Thromboembolic disease –Pulmonary embolus (definite diagnosis) –Recurrent DVTs, mainly on symptoms –Not thrombophilic ; testing negative Chronic back pain Gastro-oesophageal reflux Hypertension
 –Recurrent DVTs, mainly on symptoms –Not thrombophilic ; testing negative Chronic back pain Gastro-oesophageal reflux Hypertension")
16
On arrival HR 66 BP 155/91 RR 14 Decreased LOC, just rousable Small and sluggish pupils Multiple lacerations on left forearm Nil else on examination

17
Initial Management Response to naloxone; infusion commenced (2mg/50 mL) at 15 mL/hr Lacerations sutured Bloods sent including Group + Save
 at 15 mL/hr Lacerations sutured Bloods sent including Group + Save")
18
Initial Management 2 INR 3.7 Appropriate management ? –FFP –Vitamin K

19
Initial Management 2 Haematology consult –6 units FFP –10 mg vitamin K IVI Neurological observation 2-3 daily INR

20
Progress - Day 2 Clinical : no bleeding complications Naloxone infusion continued INR Results

21
Progress - Day 3 Haematology review : –commenced on daily enoxaparine 1 mg/kg –TED stockings –Daily INR Naloxone infusion ceased Psychiatric assessment Drug and Alcohol review

22
Progress - Day 2 - 6 Day 4 : Warfarin recommenced 14 mg daily (normal dose) Day 5 : Enoxaparin increased to twice daily Warfarin recommenced
 Day 5 : Enoxaparin increased to twice daily Warfarin recommenced")
23
Progress - Day 5 - 12 Transferred to inpatient psychiatric unit Normal warfarin dose Continue enoxaparin until therapeutic INR

24
Time course of INR Warfarin Vitamin K

25
Comments / Problems What dose of vitamin K is appropriate ? Patient still has a non-therapeutic INR two weeks after vitamin K

26
Case 3 44 year old male Drug overdose 3 hours previously –150 mg warfarin –2 g chlorpromazine Aortic valve replacement 8 years previously Asthma, OCD, pathological gambling

27
Initial Assessment Drowsy but easily roused Normal observations No active bleeding or bruising INR 1.9

28
Plan No haematology consult Q3H INR Research: –Intermittent factor levels –Serial warfarin determination Vitamin K 1 mg if INR > 5.0

29
100%

30
Excessive Anticoagulation Situation : –Therapeutic dose : drug interaction, other –Acute Overdose Thromboembolic Risk –None –Low-medium : previous DVT/PE/thrombophilia –High : mechanical heart valve

31
Acute Overdose - not own No thromboembolic risk Treatment : –vitamin K 5 - 10 mg IVI or oral –FFP if actively bleeding –Monitor INR –Straight-forward Complicated in cases of long-acting agents

32
Overdose or Therapeutic Low-Medium Risk of Thromboembolism Requirements : –decrease INR to prevent bleeding complications –can tolerate normalisation of INR for a period –need to be restarted and reach therapeutic INR Issues : –Use of FFP –Use of vitamin K and dose –requirement for heparin and hospital stay

33
Overdose or Therapeutic High Risk of Thromboembolism Requirements : –decrease INR to prevent bleeding complications –risk of thromboembolic complications with normalisation of INR for any period of time Issues : –Use of FFP –Use of vitamin K and dose –requirement for heparin and hospital stay

34
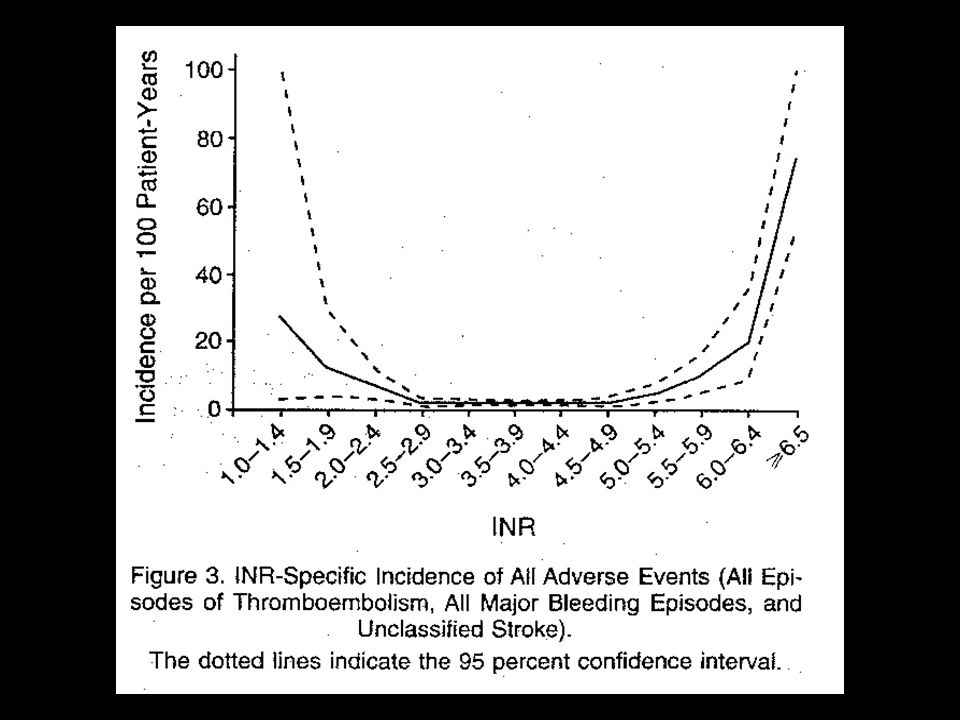
Increased INR & Risk of bleeding INR > 4.5, 5.0 and 6.0 Exponential increase in bleeding –Br J. Haem 1998 (Guidelines); –Cannegieter NEJM 1995 –Pal
; –Cannegieter NEJM 1995 –Pal.")
36
Increased INR and Risk of bleeding Palareti et al. Prospective cohort study –2745 patients on anticoagulants –F/U for a mean of 267 days –temporally related INRs Multivariate analysis: patients with an INR > 4.5 had an increased risk of bleeding, RR 5.96 (3.68- 9.67, p<0.0001), compared to INR < 4.5
, compared to INR < 4.5.")
37
Increased INR and Risk of bleeding INR > 6.0 : Hylek Arch Intern Med 2000 –Abnormal bleeding 8.8% –Major bleeding 4.4% cf. 0% INR < 6.0 (P<0.001) INR > 7.0 : Panneerselvam Br J Haem 1998 –Total bleeding 12/31 vs. 13/100 O.R. 5.4 –5 major bleeds vs. none
 INR > 7.0 : Panneerselvam Br J Haem 1998 –Total bleeding 12/31 vs. 13/100 O.R. 5.4 –5 major bleeds vs. none.")
38
Increased INR and Risk of bleeding INR > 8.0 Baglin Blood Rev 1998; –12.9% major bleeding Murphy Clin Lab Haematol 1998 Severe anticoagulation : Hung Br J Haematol 2000 –INR > 9.5 –APTT ratio > 2.0 –Required additional vitamin K doses

39
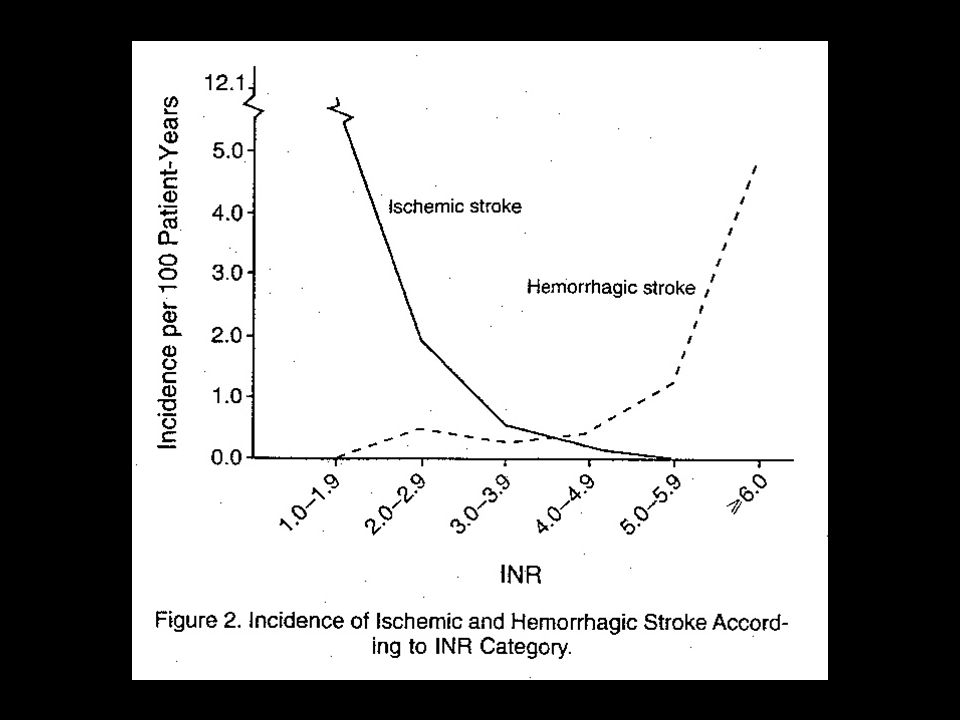
Low INR and Risk of Embolism for High risk patients Patients with mechanical heart valves Risk of embolism rises with INR < 2.5 Sub-groups with higher risk : –> 70 years age –Both > mitral > aortic –Caged ball/disk > tilting disk > bileaflet

41
Therapeutic Options Fresh frozen plasma Vitamin K –oral –intravenous Heparinisation –intravenous unfractionated –low molecular weight

42
Fresh Frozen Plasma Major bleeding Minor bleeding; risk groups eg. age Guidelines Br J Haematol 1998

43
Vitamin K ? Appropriate dose Oral vitamin K RCT : Vit K, 1 mg vs. placebo (INR 4.5 - 10) –more rapid decrease in INR; 56% vs. 20 % with INR between 1.8 - 3.2 after 24 hrs (p< 0.001) –fewer patients had bleeding episodes during follow up 4% vs. 17% p = 0.05 ( 3 months) –Crowther Lancet 2000
 –more rapid decrease in INR; 56% vs. 20 % with INR between after 24 hrs (p< 0.001) –fewer patients had bleeding episodes during follow up 4% vs. 17% p = 0.05 ( 3 months) –Crowther Lancet")
44
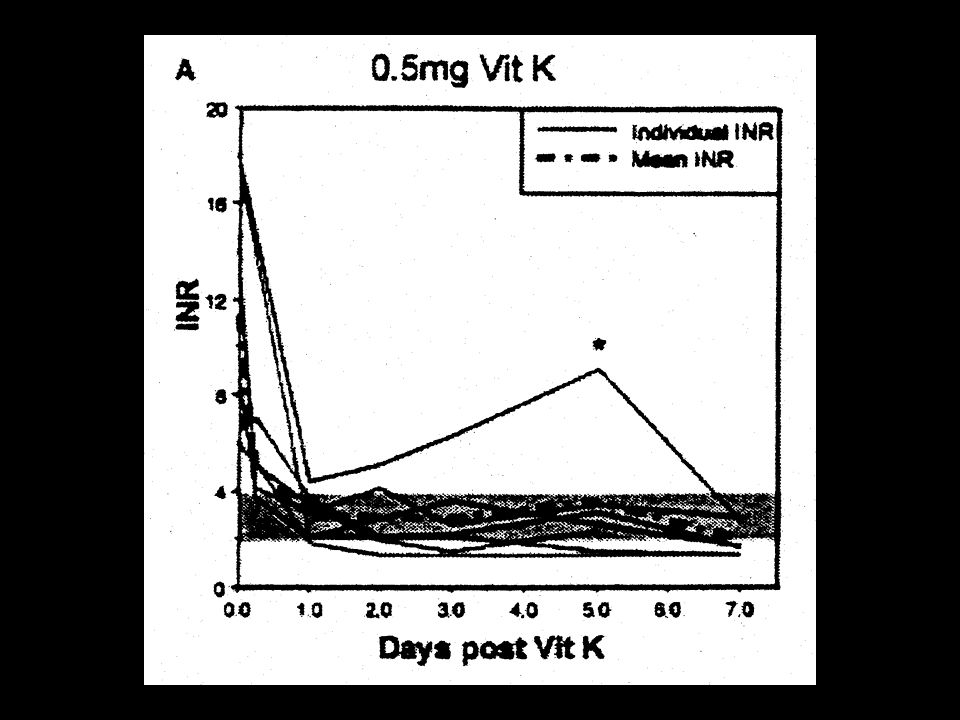
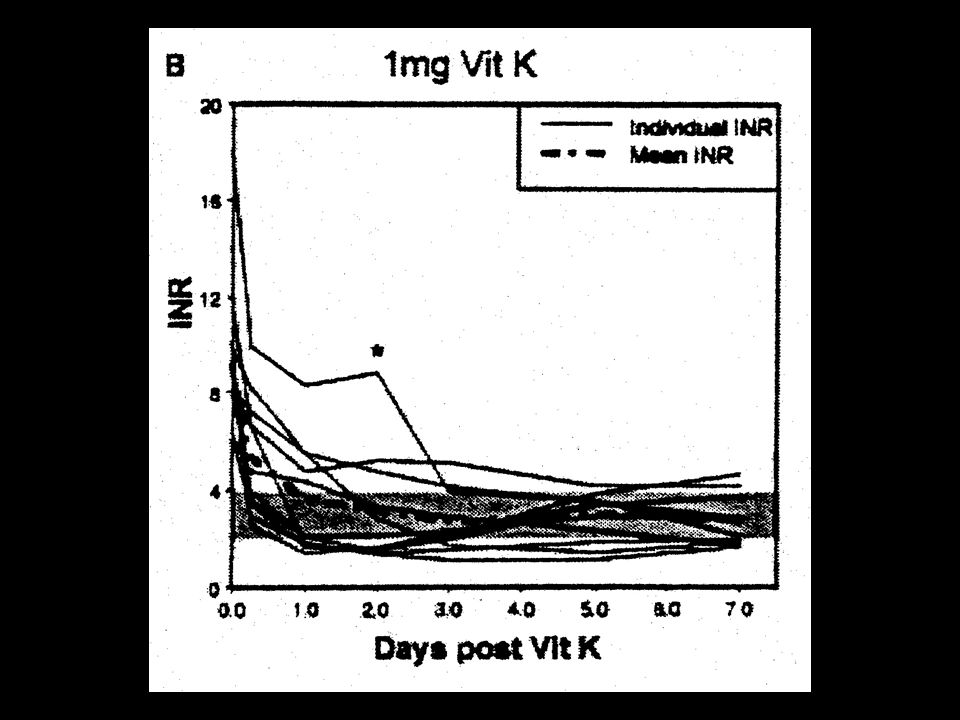
Vitamin K ? Appropriate dose Intravenous vitamin K; RCT : INR > 6.0 –asymptomatic 0.5 mg vs. 1 mg –symptomatic 1 mg vs. 2 mg INR fallen to 5 - 5.5 in all 3 groups by 6 hrs –Optimal INR (2-4) in 67% receiving 0.5 mg, but only in 33% receiving 1 or 2 mg –Over-correction in 16% (0.5 mg); 50% (1-2 mg) –no adverse effects Hung. Br J Haematol 2000
 in 67% receiving 0.5 mg, but only in 33% receiving 1 or 2 mg –Over-correction in 16% (0.5 mg); 50% (1-2 mg) –no adverse effects Hung. Br J Haematol")
48
Vitamin K - Suggested dosing INR > 5.0 ; asymptomatic, mild bleeding –0.5 mg IV –repeat INR 6 - 12 hours –titrate as required INR > 9.5; APTT ratio > 2.0 –1 mg IV –repeat 6 hours –more likely to require repeat doses

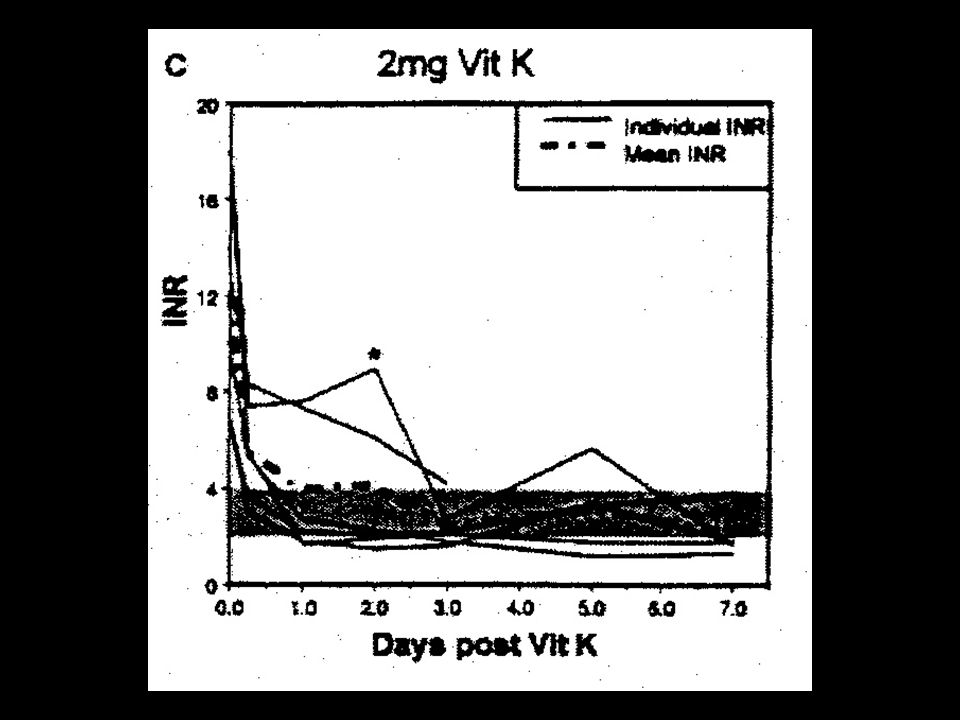
49
Vitamin K

Similar presentations