Download presentation
Presentation is loading. Please wait.

1
Metabolic Bone disease Tanya Potter Consultant Rheumatologist

2
Aims and Objectives Aims –Understand the definition and spectrum of metabolic bone diseases Objectives –demonstrate understanding of epidemiology, aetiology, clinical features and management of osteoporosis, osteomalacia, Paget’s disease and renal osteodystrophy

3
Case 1 72 year old lady Acute onset severe thoracic pain Keeping her awake at night Radiates around ribs No history of trauma PMH – COPD DH - Inhalers What other questions would you ask?

4
Case 1 - contd On examination – –Frail lady –Apyrexial –Thoracic kyphosis –Tender over spinous processes T7/8 –No neurological deficit –differential diagnosis?

5
Diff. Diagnosis of Back Pain Simple mechanical eg ligamentous strain Degenerative disease with/without neural, cord or canal compromise Metabolic – osteoporosis, Pagets Inflammatory – Ankylosing spondylitis Infective – bacterial and TB Neoplastic Others, (trauma,congenital) Visceral
 Visceral.")
6
Case 1 Investigations HB 12.9, WCC 9.0, Plts 245 Na 139, K 4.4, U 7.3, Cr 96 AP 297, ALT 32, Bil 13, Ca 2.41 CRP 8

8
Osteoporosis Reduction in bone mass leading to increase risk of fracture Ratio of mineralised bone: matrix is normal Imbalance of bone remodelling

10
Risk factors for osteoporosis?

12
Measurement and definition of OP?

13
DEXA

14
T scores

16
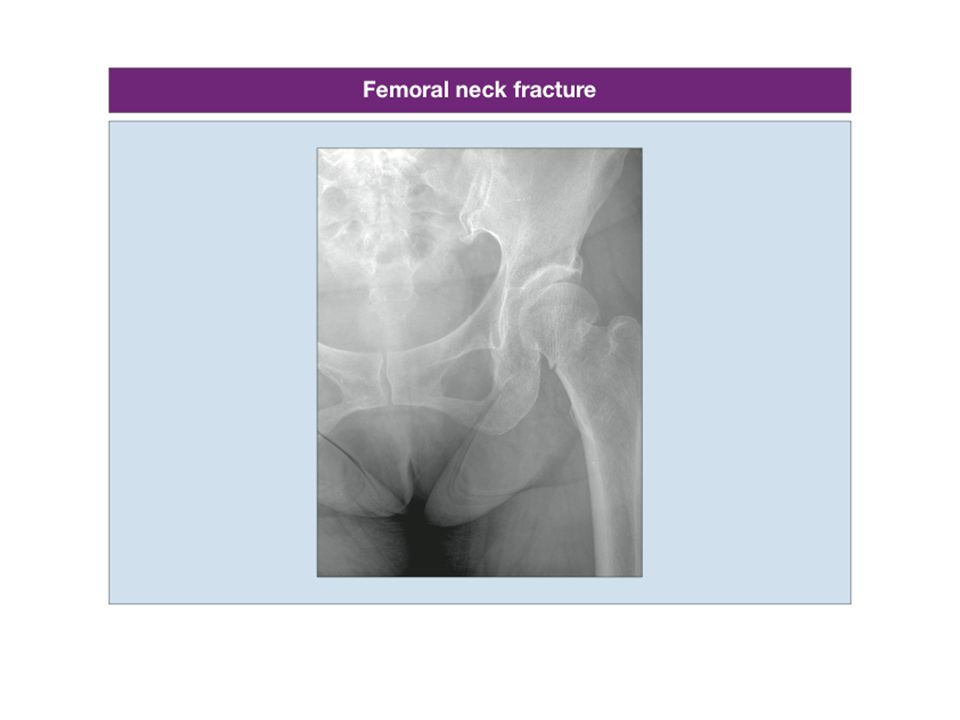
Typical OP # ?

17
OP fractures

20
250,000 # / yr in UK

21
Treatment for OP ?

22
Osteoporosis Lifestyle factors –Falls prevention –Hip protectors Ca and Vit D

23
Bisphosphonates Strontium SERMs Teriparatide- PTH

24
Preventing steroid induced osteoporosis All: lifestyle advise, calcium and vit D Age <65DEXA- if T score -1.0 or less then alendronate Age >65alendronate

25
NICE guidance http://guidance.nice.org.uk/TA87/?c=9152 4http://guidance.nice.org.uk/TA87/?c=9152 4 www.sheffield.ac.uk/FRAX/tool

26
Case 2 33 year old Asian lady Presents with 3 /12 history of generalised bony pain PMH – depression DH – sertraline O/E – generalised bony tenderness Joints – normal ROM, no inflammation

27
Investigations Hb 12.9 (11.5-16.5)Calcium 2.18 (2.2-2.6) WCC4.7 (4.9-11.0)Phosphate 0.79 (0.85- 1.45) Plt253 (150-400)Albumin39 (35-50) ESR 12Alk Phos172 (25-96) Clotting NormalTotal protein 72 (60-80) Urea 4.2 (3.0-6.5)LFTsnormal Creat85 (35-120)
Calcium 2.18 ( ) WCC4.7 ( )Phosphate 0.79 ( ) Plt253 ( )Albumin39 (35-50) ESR 12Alk Phos172 (25-96) Clotting NormalTotal protein 72 (60-80) Urea 4.2 ( )LFTsnormal Creat85 (35-120)")
28
Diagnosis?

30
Osteomalacia Rickets of adulthood Deficiency or resistance to Vit D OR Phosphate handling problem Defective mineralization of bone Proximal myopathy, Bony pain, malaise –Deformities much less common than with rickets AP raised, Ca and Vit D low or normal PO4 low or normal

31
Causes of osteomalacia/rickets Reduced availability of Vit D –Diet: oily fish, eggs, breakfast cereals –Elderly individuals with minimal sun exposure –Dark skin, skin covering when outside –Fat malabsorption syndromes –Kidney failure –malabsorption

32
malabsorption –Coeliac –Intestinal bypass –Gastrectomy –Chronic pancreatitis –Pbc Epilepsy: phenytoin, phenobarbitones Genetic disease

33
Defective metabolism of Vitamin D –Chronic renal failure, Vit D dependent rickets, –Liver failure, anticonvulsants Receptor Defects Altered phosphate homeostasis –Malabsorption, RTA, hypophosphatasia (rare, low levels of alk phos)
")
34
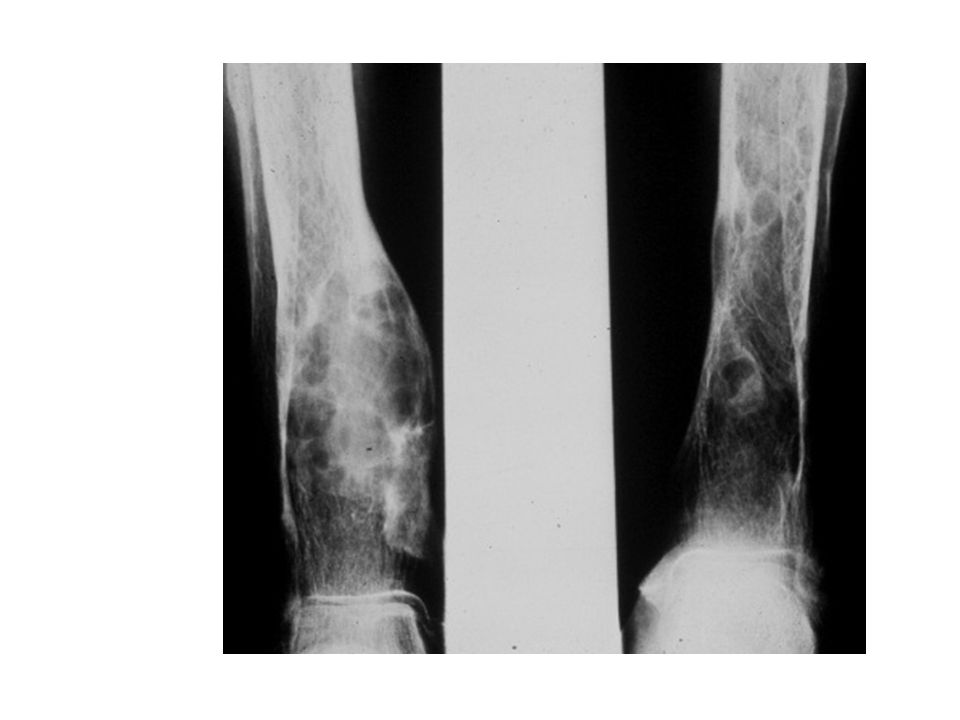
Loosers zones

35
Treatment Vitamin D –usually oral Calcium supplements

36
Case 3 62 year old lady referred with generalised muscular pain PMH – hypertension DH – bendrofluazide Examination – largely unremarkable Routine bloods all normal except Calcium of 2.95 She has come back to clinic for results What would you do now?

37
Symptoms of hypercalcaemia Stones, Bones, Moans, Psychic Groans

38
An approach to hypercalcaemia Stones, Renal colic Bones, Joint, bone, muscle pain, Muscle weakness Moans, Constipation Abdominal pains Psychic Groans Depression, confusion, altered mental state, Fatigue, lethargy Dehydration, polyuria

39
Causes of Hypercalcaemia Malignancy Hyperparathyroidism – primary or tertiary Increased intake Myeloma Sarcoid Adrenal failure

42
Treatment of acute hypercalcaemia Hydration, IV if Ca very high Bisphosphonates Treat cause

43
Hyperparathyroidism Primary hyperparathyroidism: –Often an incidental finding –May be part of MEN I, MEN II Secondary hyperparathyroidism –Compensates for chronic low Ca eg. Renal failure or malabsorption –[Ca 2+ ] and [PO 4 2- ] normal PTH high Tertiary hyperparathyroidism –Hyperplasia in longstanding secondary disease

44
Multiple endocrine neoplasia Aut dom MEN 1 parathyroid tumours, ant pituitary, pancreas MEN 2A thyroid tumour, phaeochromocytomas, parathyroid hyperplasia MEN 2B thyroid tumours and phaeos

45
Renal Osteodystrophy Effect on bone of disordered calcium homeostasis May be osteomalacia, hyperparathyroidism Leads to –Bone pain –Skeletal deformity –Muscular weakness –Ectopic calcification –Growth retardation

46
Hypoparathyroidism Causes Destruction of gland- surgical (thyroidectomy- may be transient) Autoimmune- polyglandular autoimmune glandular syndrome Irradiation or infiltration (cancer, wilsons) Abnormal gland development
 Autoimmune- polyglandular autoimmune glandular syndrome Irradiation or infiltration (cancer, wilsons) Abnormal gland development")
47
Case 4 This 73 year old lady was referred from her GP to ENT with deafness. They asked her to see the rheumatologist Why?

48
Paget’s Disease Disease of bone remodeling Accelerated bone resorption and formation Disorganised mosaic pattern bone with increased vascularity and fibrosis Cause unknown –paramyxovirus, canine distemper –Genetics- susceptibility loci More common in caucasian M:F ratio 3:210% in over 70’s

49
Paget’s Disease: clinical manifestations Bone pain Joint pain Deformity Spontaneous fractures

50
Pagets Disease: complications Fractures Deafness Nerve entrapment Spinal stenosis Cardiac failure Osteogenic sarcoma Hypercalcaemia (only if immobilized)
")
51
Paget’s Disease: investigations Raised serum alk phos Urinary hydroxyproline, pyridinoline cross-links Radiology –cortical thickening –osteolytic, osteosclerotic and mixed lesions –osteoporosis circumscripta –bone scan

52
Normal

55
Paget’s Treatment Bisphosphonates –calcitonin Indicated if –Complications –Pain –Deformity –AP 2-3X Upper limit –Skull disease

56
Questions?

Similar presentations






















 1,25(OH) 2 D 3 calcitriol Synthesis of active vitamin D 10%, 90%, Bile Salts Tightly regulated 25-hydroxylase.>")





