Download presentation
Presentation is loading. Please wait.

1
Metabolic bone diseases
There is a clinical problem?

3
Osteopertrosis Hereditary decreased osteoclastic function. Decreased resoprtion leads to thick sclerotic bones. Pathology Problems with the osteoclast resorption pit Increased bone density -> thick brittle bones -> fracture Marrow decreased by bone growth, may cause pancytopenia. Extramedullarly haematopoeisis Cranial nerve compression -> blindness, deafness, vision loss

4
Osteopetrosis X ray Clinical features Treatment
Osteosclerosis, long bones -> Erlenmeyer flask shaped deformity Clinical features Autosomal recessive (malignant) Infants and children, multiple fractures, early death Autosomal dominant (benign type) Adults, fractures, mild anaemia, cranial nerve impingement Carbonic anhydrase II deficiency Renal tubular acidosis, cerebral calcificaiton Treatment Bone marrow transplant
 Infants and children, multiple fractures, early death. Autosomal dominant (benign type) Adults, fractures, mild anaemia, cranial nerve impingement. Carbonic anhydrase II deficiency. Renal tubular acidosis, cerebral calcificaiton. Treatment. Bone marrow transplant.")
6
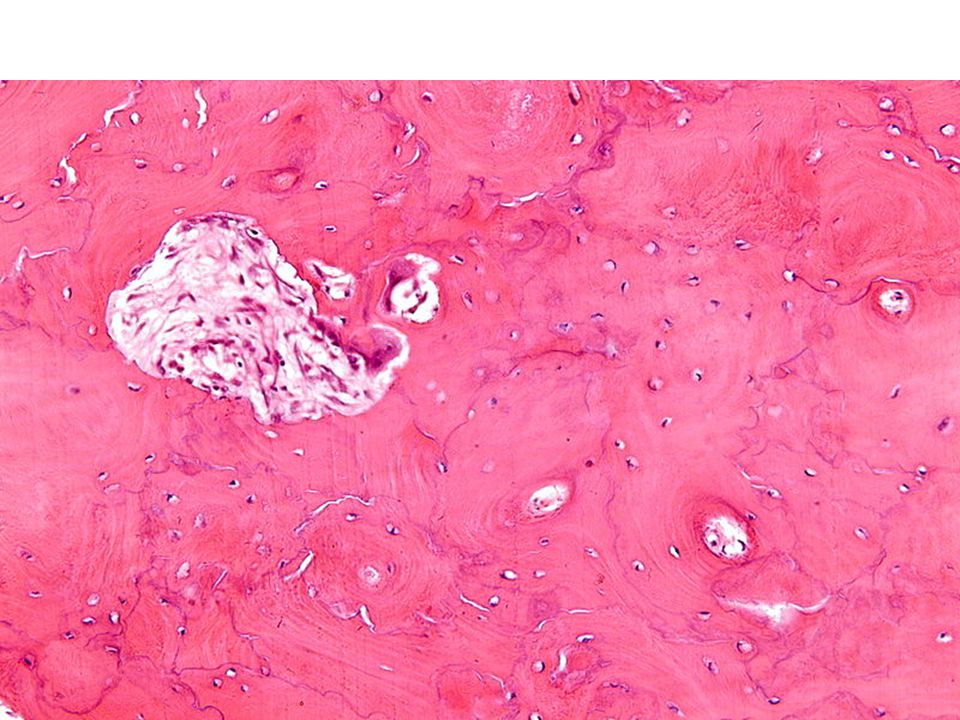
Paget’s disease (osteitis deformas)
Localised disorder of bone remodelling caused by excessive resorption and disorganised replacement leading to thickened but weaker bone. Epidemiology – begins after age 40, european ancestry Etiology – possible genetic predisposition, possibly paramyxovirus Forms of involvement Monostotic (15%), polystotic (85%) Commonly – skull, pelvis, femur, vertebrae Pathology Three stages Osteolytic – otseoclastic activity predominates Mixed osteoclastic and osteoblastic Osteosclerotic – osteoblastic activity predominates -> burnout stage Micro haphazard arrangement leads to mosiac pattern of lamellar bone Bone is weak, fractures easily Skull involvement Increase in head size Foraminal narrowing leading impingement of the cranial nerves Facial bones can be involved leading to a lion like face
, polystotic (85%) Commonly – skull, pelvis, femur, vertebrae. Pathology. Three stages. Osteolytic – otseoclastic activity predominates. Mixed osteoclastic and osteoblastic. Osteosclerotic – osteoblastic activity predominates -> burnout stage. Micro haphazard arrangement leads to mosiac pattern of lamellar bone. Bone is weak, fractures easily. Skull involvement. Increase in head size. Foraminal narrowing leading impingement of the cranial nerves. Facial bones can be involved leading to a lion like face.")
7
Paget’s disease (osteitis deformas)
X-ray Bone enlargement with lytic and sclerotic areas. Complications AV shunts within marrow can cause high output cardiac failure. Osteosarcoma or other sarcomas.

9
Osteoporosis Osteopenia Epidemiology Pathogenesis Clinical features
Most common bone disease Elderly, post menopausal Pathogenesis Primary………………………. Secondary………………….. Clinical features Bone pain and fractures Weight bearing bone predisposed to fracture Loss of height and kyphosis

10
Osteoporosis X-ray Treatment General translucency of bone
Oestrogen replacement therapy – controversial Weight bearing exercise Calcium and vitamin D Biphosphonate Calcitonin

12
Osteomalacia and Rickets
Decreased mineralisation of newly formed bones, usually caused by deficiency or abnormal metabolism of vitamin D. Etiology – deficiency of vit D, intestinal malabsorption, lack of sunlight, renal or liver disease. Epidemiology Osteomalacia – adults Rickets - children

13
Osteomalacia and Rickets
Pathogenesis Osteomalacia -> poor mineralisation of newly formed bone -> thin fragile bones -> fracture Rickets Remodelled bone and bone at growth plates are undermineralised Endochondral bone formation also affected -> deformity Fractures also occur Clinical presentation Osteomalacia -> bone pain, fracture (vertebrae, hips, wrist) Rickets -> bow legs, craniotabes, lumbar lordosis,
 Rickets -> bow legs, craniotabes, lumbar lordosis,")
14
Hyperparathyroidism Primary Secondary Tertiary?
Adenoma or autonomous hyperplasia (Robbins) Secondary Caused by prolonged states of hypocalcemia leading to hyperplasia Tertiary? Autonomous hyperplasia Severe cases lead to osteitis cystic fibrosa (no longer though…) Presentation Asymptomatic hypercalcamia Treatment Curvative parathyroidectomy
 Secondary. Caused by prolonged states of hypocalcemia leading to hyperplasia. Tertiary Autonomous hyperplasia. Severe cases lead to osteitis cystic fibrosa (no longer though…) Presentation. Asymptomatic hypercalcamia. Treatment. Curvative parathyroidectomy.")
15
Renal Osteodystrophy Describes clinically all of the skeletal changes of chronic renal disease. Increased osteoclastic bone resorption mimicking osteoitis fibrosa cystica. Delayed matrix mineralisation. Osteosclerosis. Growth retardation. Osteoporosis. Main types High turnover -> increased resorption and bone formation (dominates) Low turnover (aplastic) -> adynamic bone, less commonly osteomalacia
 Low turnover (aplastic) -> adynamic bone, less commonly osteomalacia.")
16
Renal Osteodystrophy Pathogenesis (long..)
Chronic renal failure results in phosphate retention and hyperphosphatemia Hyperphospatemia induces secondary hyperparathyroidism (via regulating PTH secretion) Hypocalcaemia develops due vitamin D problems (kidneys) PTH secretion markedly increases at all levels of serum calcium In renal failure decrease in the binding of 1,25-(OH)2D3 to parathyroid cells Decreased degradation and excretion of PTH (kidneys) Secondary hyperparathyroidism produces increased osteoclastic activity Metabolic acidosis associated with renal failure leads to bone resorption
 Hypocalcaemia develops due vitamin D problems (kidneys) PTH secretion markedly increases at all levels of serum calcium. In renal failure decrease in the binding of 1,25-(OH)2D3 to parathyroid cells. Decreased degradation and excretion of PTH (kidneys) Secondary hyperparathyroidism produces increased osteoclastic activity. Metabolic acidosis associated with renal failure leads to bone resorption.")
Similar presentations











 1,25(OH) 2 D 3 calcitriol Synthesis of active vitamin D 10%, 90%, Bile Salts Tightly regulated 25-hydroxylase.>")








 Vitamin D 2 : Ergosterol (pro D 2 ) Ergocalciferol (D 2 ) added to milk and dairy. (Human) Vitamin D 3 : Pro (7-dehydrocholesterol)>")

