Download presentation
Presentation is loading. Please wait.

1
Chronic Kidney Disease (CKD)
Shiva Seyrafian IKRC- IUMS 1392/2/19____9/5/2013

2
The Story of Mr. G. L. 45 yr with Diabetes for 10 yrs, “reasonably well controlled” PMH: Hypertension for 7 yrs..well controlled BMI of 30 Dyslipidemia Fam Hx: Diabetes; Soc Hx: Sedentary; non smoker; Comedian Exam 139/85 – Mild Obesity, rest fairly normal Labs BUN 28, Creatinine 1.8, Urine protein (dipstick) 2+
 2+")
3
Chronic Kidney Disease
Definition: Chronic, irreversible loss of kidney function attributable to loss of functional nephron mass – pathophysiologic processes for more than 3 months.

4
Epidemiology CKD affects about 26 million people in the US
Approximately 19 million adults are in the early stages of the disease On the rise due to increasing prevalence of diabetes and hypertension Total cost of ESRD in US was approximately $40 billion in 2008

5
Pathophysiology of CKD
Final Common Pathway is loss of nephron mass Diabetes Hypertension Chronic GN Cystic Disease Tubulointerstitial disease Mediated by vasoactive molecules, cytokines and growth factors, renin angiotensin axis

6
Pathophysiology Repeated injury to kidney
The causes of acute or chronic kidney disease are traditionally classified by that portion of the renal anatomy most affected by the disorder The two major causes of reduced renal perfusion are volume depletion and/or relative hypotension. This may result from true hypoperfusion due to bleeding, gastrointestinal, urinary, or cutaneous losses, or to effective volume depletion in heart failure, shock, or cirrhosis Various vascular diseases can also lead to kidney disease. Direct etiologies from kidney: Tubular and interstitial disease, Glomerular disease, Obstructive uropathy Acute tubular necrosis — 45 percent Prerenal — 21 percent Acute or chronic kidney disease — 13 percent (mostly due to acute tubular necrosis and prerenal disease) Urinary tract obstruction — 10 percent (most often older men with prostatic disease) Glomerulonephritis or vasculitis — 4 percent Acute interstitial nephritis — 2 percent Atheroemboli — 1 percent
 Urinary tract obstruction — 10 percent (most often older men with prostatic disease) Glomerulonephritis or vasculitis — 4 percent. Acute interstitial nephritis — 2 percent. Atheroemboli — 1 percent.")
7
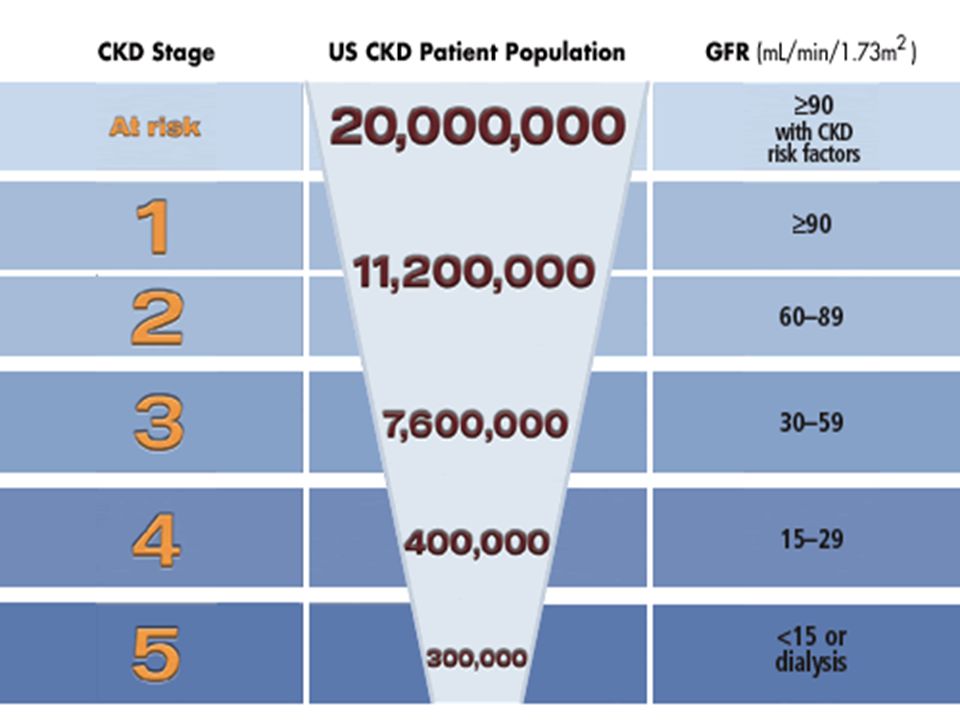
Staging of Chronic Kidney Disease
Stage Description GFR (ml/min/1.73 m2) At increased risk 90 (with CKD risk factors) 1 Kidney damage with normal or increased GFR 90 2 Kidney damage with Mildly decreased GFR 60-89 3 Moderately decreased GFR 30-59 4 Severely decreased GFR 15-29 5 Renal Failure <15 (or dialysis)
 At increased risk. 90 (with CKD risk factors) 1. Kidney damage with normal or increased GFR Kidney damage with Mildly decreased GFR Moderately decreased GFR Severely decreased GFR Renal Failure. <15 (or dialysis)")
8
Who is at Risk for CKD? Family history of heritable renal disease
Diabetes Hypertension Auto-immune disease Old age Prior episode of ARF Current evidence of renal damage, even with normal or increased GFR

9
Estimation of GFR Modification of Diet in Renal Disease (MDRD) Formula
Estimated GFR = 1.86 (Serum Creat) X (age) Multiply by for women Multiply by 1.21 for African Americans Cockroft Gault Formula (140 – age) X Body Weight (Kg) 72 X Serum Creatinine (mg/dL) Multiply by 0.85 for women
 X (age) Multiply by for women. Multiply by 1.21 for African Americans. Cockroft Gault Formula. (140 – age) X Body Weight (Kg) 72 X Serum Creatinine (mg/dL) Multiply by 0.85 for women.")
10
MDRD GFR for Mr Lopez Diabetic, Hypertension, Metabolic Syndrome X
Stage 3 CKD GFR = 44 ml/min/1.73 m2

11
Stages in Progression of CKD and Therapeutic Strategies
AJKD 2002: 39(2)
")
13
Etiology and Epidemiology
6% of the US population has CKD (Stage 1 and 2) Additional 4-5% have Stage 3 and 4 CKD Diabetic nephropathy Hypertension – chronic ischemic nephropathy Very high CV disease burden
 Additional 4-5% have Stage 3 and 4 CKD. Diabetic nephropathy. Hypertension – chronic ischemic nephropathy. Very high CV disease burden.")
14
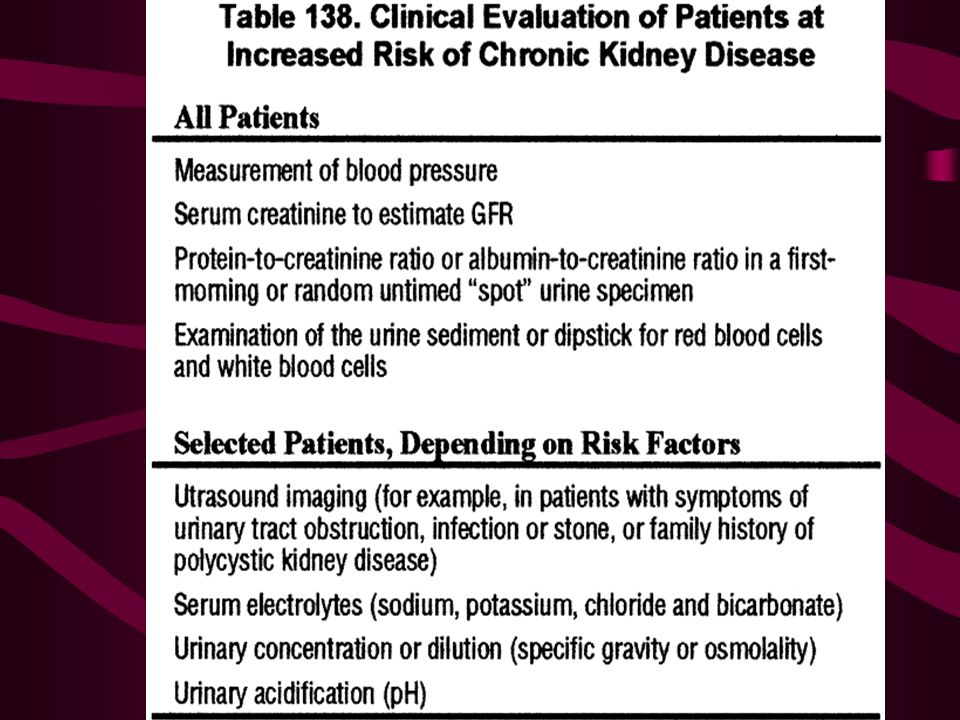
Monitoring of CKD Serial measurements of Albumin
Creatinine GFR Albumin Albumin-creatinine ratio in the 1st morning sample Electrolytes including HCO3, Ca, Phos; alkaline phosphatase, iron studies, intact PTH Renal sonogram Renal biopsy

15
Symptoms of CKD Stage 1 and 2 Stage 3 and 4 Stage 5
Asymptomatic, hypertension Stage 3 and 4 Anemia – loss of energy Decreasing appetite; poor nutrition Abnormalities in Calcium, Phosphorus metabolism Sodium, water, potassium and acid base abnormalities Stage 5 All of the above – accentuated; eventually overt uremia

16
Symptoms Hematuria Flank pain Edema Hypertension Signs of uremia
Lethargy and fatigue Loss of appetite If asymptomatic may have elevated serum creatinine concentration or an abnormal urinalysis

17
Common Causes and Presentation
Clinical Presentation Diabetic kidney disease History of diabetes, proteinuria and retinopathy Hypertension Elevated BP, normal UA, family history Non diabetic glomerular disease Nephritic or nephrotic presentations Cystic kidney disease Urinary symptoms, abnormal sediment, radiologic findings Tubulointerstitial disease UTI, reflux, chronic med use, drugs, imaging abnormalities, urine concentrating defects

19
Risk Factors Age of more than 60 years Hypertension and Diabetes
Responsible for 2/3 of cases Cardiovascular disease Family history of the disease. Race and ethnicity Highest incidence is for African Americans Hispanics have higher incidence rates of ESRD than non-Hispanics. _followed by American Indians and Alaska Natives, then Asian Americans and native Hawaiians and other Pacific Islanders, and finally Caucasians.

20
Convergence of Genetic Factors
Genes for heart and vascular disease Genes that maintain ionic balance Genes for glomerulonephritis Genes for diabetes Genes that may be involved in inherited renal diseases

21
Genetic Considerations
Autosomal dominant PKD Alport’s hereditary nephritis Familial FSGS Nephronopthisis Medullary cystic kidney disease Fabry’s disease

25
Natural History of CKD Most CKD has a logarithmic progression and is predictable

26
Mr. G. L. – Progressive Decline

27
Clinical Features of Diabetic CKD

28
Symptoms of Uremia Organ System Symptoms Signs General
Fatigue, weakness Sallow-appearing, chronically ill Skin Pruritus, easy bruisability Pallor, ecchymoses, excoriations, edema, xerosis ENT Metallic taste in mouth, epistaxis Urinous breath / fetor Eye Pale conjunctiva Pulmonary Shortness of breath Rales, pleural effusion Cardiovascular Dyspnea on exertion, retrosternal pain on inspiration (pericarditis) Hypertension, cardiomegaly, friction rub Gastrointestinal Anorexia, nausea, vomiting, hiccups Genitourinary Nocturia, impotence Isosthenuria Neuromuscular Restless legs, numbness and cramps in legs Neurologic Generalized irritability and inability to concentrate, decreased libido Stupor, asterixis, myoclonus, peripheral neuropathy
 Hypertension, cardiomegaly, friction rub. Gastrointestinal. Anorexia, nausea, vomiting, hiccups. Genitourinary. Nocturia, impotence. Isosthenuria. Neuromuscular. Restless legs, numbness and cramps in legs. Neurologic. Generalized irritability and inability to concentrate, decreased libido. Stupor, asterixis, myoclonus, peripheral neuropathy.")
29
Sodium and water Imbalance
Sodium retention, contributes to hypertension. Higher than usual doses for diuretics. In situations with volume depletion – can be severe, because of inadequate sodium retention.

30
Potassium Imbalance Potassium GI excretion is augmented
Constipation, dietary intake, protein catabolism, hemolysis, hemorrhage, transfusion of stored blood, metabolic acidosis, Drugs: ACE inhibitors, ARBs, B blockers, K sparing diuretics and NSAIDs Hyporeninemic hypoaldosteronism: Diabetes, sickle cell disease

31
Acid Base Imbalance Damaged kidneys are unable to excrete the 1 mEq/kg/d of acid generated by metabolism of dietary proteins. NH3 production is limited because of loss of nephron mass Decreased filtration of titrable acids – sulfates, phosphates Decreased proximal tubular bicarb reabsorption, decreased H ion secretion Arterial pH: ; serum HCO3 rarely below 15 – buffering offered by bone calcium carbonate and phosphate Should be maintained over 21

33
Bone Disease

34
Young boy on HD several years with 2nd hyperpara, brown tumor and cyst, 91/8

35
Mineral Metabolism Calciphylaxis
PTH, P, Ca x P, Active Vitamin D, Fetuin A, Matrix Gla protein ( warfarin) Calcemic uremic arteriopathy Extraosseous/metastatic calcification of soft tissues and blood vessels Devastating complication
 Calcemic uremic arteriopathy. Extraosseous/metastatic calcification of soft tissues and blood vessels. Devastating complication.")
38
Reza ahmadi niya –alzahra univ. haospit
Reza ahmadi niya –alzahra univ. haospit. HD, renal osteodystrophy 91/ 7, 69 Y/O

39
Reza ahmadi niya –alzahra univ. haospit
Reza ahmadi niya –alzahra univ. haospit. HD, renal osteodystrophy 91/ 7, 69 Y/O

40
Reza ahmadi niya –alzahra univ. haospit
Reza ahmadi niya –alzahra univ. haospit. HD, renal osteodystrophy 91/ 7, 69 Y/O

41
Cardiovascular Abnormalities
Leading cause of morbidity and mortality in patients with CKD at all stages Ischemic CAD Hypertension and LVH Congestive heart failure Uremic pericarditis

42
Cardiovascular risks in CKD
Reduced glomerular filtration rate (GFR) and proteinuria are both independently associated with an increased risk of cardiovascular events. The increase in cardiovascular risk associated with CKD. The risk of death, particularly due to cardiovascular disease, is typically higher than the risk of eventually requiring renal replacement therapy.
 and proteinuria are both independently associated with an increased risk of cardiovascular events. The increase in cardiovascular risk associated with CKD. The risk of death, particularly due to cardiovascular disease, is typically higher than the risk of eventually requiring renal replacement therapy.")
43
Pericarditis Uremic pericarditis:There is a correlation with the degree of azotemia (the BUN is usually >60 mg/dL), Except in the case of systemic immune disorders (such as lupus erythematosus or scleroderma), there is no relationship with the underlying cause of renal failure. Dialysis-associated pericarditis: two causses: inadequate dialysis (ie, the patient has uremic pericarditis) and/or fluid overload.
, Except in the case of systemic immune disorders (such as lupus erythematosus or scleroderma), there is no relationship with the underlying cause of renal failure. Dialysis-associated pericarditis: two causses: inadequate dialysis (ie, the patient has uremic pericarditis) and/or fluid overload.")
44
Pericarditis Unusual feature of uremic pericarditis: the electrocardiogram does not show the typical diffuse ST and T wave elevations observed with other causes of acute pericarditis. With the development of cardiac tamponade, typical ECG changes (eg, electrical alternans) may occur
 may occur.")
45
Cardiac Complications

46
Lipid abnormalities The most common dyslipidemia in CKD patients is hypertriglyceridemia, whereas the total cholesterol concentration can be normal or low, perhaps due in part to malnutrition. Some have found that low (not high) serum cholesterol values are associated with increased mortality.
 serum cholesterol values are associated with increased mortality.")
47
Lipid abnormalities Some have found no association between lipid levels and mortality among patients with CKD. Reflect the adverse effect of malnutrition and chronic inflammation upon mortality.

48
Hematological Abnormalities
Anemia: Chronic blood loss, hemolysis, marrow suppression by uremic factors, and reduced renal production of EPO Normocytic, normochromic Coagulopathy: Clinical bleeding in uremia is typically cutaneous, including easy bruising and mucosal bleeding, or may occur in response to injury or invasive procedures. Less frequent is epistaxis, gingival bleeding, or hematuria. Mainly platelet dysfunction – decreased activity of platelet factor III, abnormal platelet aggregation and adhesiveness and impaired thrombin consumption Increased propensity to bleed – post surgical, GI Tract, pericardial sac, intracranial Increased thrombotic tendency – nephrotic syndrome

49
Other Abnormalities Neuromuscular
Central, peripheral and autonomic neuropathy Motor Neuropathy: muscle atrophy, myoclonus, and eventual paralysis. Mononeurpathy: Carpal tunnel syndrome Dysfunction of both the vestibular and cochlear divisions of the eighth cranial nerve Polyneuropathy: paresthesias, burning sensations, and pain — tend to precede the motor symptoms. The initial finding in uremic polyneuropathy is loss of position and vibration sense in the toes and decreased deep tendon reflexes, beginning with the Achilles reflex. The hands may become involved. Sensory syndromes: restless leg syndrome, the burning foot syndrome, Paradoxical heat sensation

50
Other Abnormalities Gastrointestinal Endocrine Uremic fetor
Gastritis, peptic disease, mucosal ulcerations, Endocrine Glucose metabolism Some patients have hyperglycemia in response to oral and intravenous glucose loads, while others are able to maintain normoglycemia by raising plasma insulin levels. Accumulation of a uremic toxin or toxins and excess parathyroid hormone (PTH), resulting from abnormalities in phosphate and vitamin D metabolism, are thought to be responsible for the insulin resistance
, resulting from abnormalities in phosphate and vitamin D metabolism, are thought to be responsible for the insulin resistance.")
51
Other Abnormalities HYPOGLYCEMIA spontaneous hypoglycemia. This complication can be seen in both diabetic and nondiabetic subjects. Estrogen levels – amenorrhea, frequent abortions Male: oligospermia, germinal cell dysplasia, delayed sexual maturation Dermatologic Pallor, ecchymoses, hematomas, calciphylaxis, pruritus, uremic frost

52
Dermatologic changes of Uremic

53
Uremic Complications

54
What Should Patients and Doctors Know
In general CKD is characterized by a gradual loss of the kidney’s filtration capacity. Markers Don’t tell everything Source:

55
What Should Patients and Doctors Know
Prevention Keep diabetes and blood pressure controlled If at risk perform screening tests Reduce exposure to nephrotoxic drugs Eat right and exercise Know your family history If you have a positive family history ask doctor to perform common screening tests for kidney function.

58
Thanksمتشکرم

Similar presentations








>")





 Dr. Belal Hijji, RN, PhD April 18 & 23, 2012.>")










