Download presentation
Presentation is loading. Please wait.

1
Prostate Radiotherapy A-Z
Dr Hamid Reza Dehghan Manshadi Radiation Oncologist Shahid Beheshti University of Medical Sciences

2
Distant metastasis (M)§
Staging Clinical (cT) T0 No evidence of primary tumor T1 Clinically inapparent tumor neither palpable nor visible by imaging T1a Tumor incidental histologic finding in 5 percent or less of tissue resected T1b Tumor incidental histologic finding in more than 5 percent of tissue resected T1c Tumor identified by needle biopsy (eg, because of elevated PSA) T2 Tumor confined within prostate* T2a Tumor involves one-half of one lobe or less T2b Tumor involves more than one-half of one lobe but not both lobes T2c Tumor involves both lobes T3 Tumor extends through the prostate capsule• T3a Extracapsular extension (unilateral or bilateral) T3b Tumor invades seminal vesicle(s) T4 Tumor is fixed or invades adjacent structures other than seminal vesicles such as external sphincter, rectum, bladder, levator muscles, and/or pelvic wall Distant metastasis (M)§ M0 No distant metastasis M1 Distant metastasis M1a Nonregional lymph node(s) M1b Bone(s) M1c Other site(s) with or without bone disease
 T0 No evidence of primary tumor. T1 Clinically inapparent tumor neither palpable nor visible by imaging. T1a Tumor incidental histologic finding in 5 percent or less of tissue resected. T1b Tumor incidental histologic finding in more than 5 percent of tissue resected. T1c Tumor identified by needle biopsy (eg, because of elevated PSA) T2 Tumor confined within prostate* T2a Tumor involves one-half of one lobe or less. T2b Tumor involves more than one-half of one lobe but not both lobes. T2c Tumor involves both lobes. T3 Tumor extends through the prostate capsule• T3a Extracapsular extension (unilateral or bilateral) T3b Tumor invades seminal vesicle(s) T4 Tumor is fixed or invades adjacent structures other than seminal vesicles such as external sphincter, rectum, bladder, levator muscles, and/or pelvic wall. Distant metastasis (M)§ M0 No distant metastasis. M1 Distant metastasis. M1a Nonregional lymph node(s) M1b Bone(s) M1c Other site(s) with or without bone disease.")
3
TNM anatomic stage prognostic groups for prostate cancer*
Stage (T) (N) (M) PSA Gleason I T1a-c N M PSA < Gleason ≤6 T2a N M PSA < Gleason ≤6 T1-2a N M PSA X Gleason X IIA T1a-c N M PSA < Gleason 7 T1a-c N M PSA ≥10<20 Gleason ≤6 T2a N M PSA < Gleason ≤7 T2b N M PSA < Gleason ≤7 T2b N M PSA X Gleason X IIB T2c N M Any PSA Any Gleason T N M PSA ≥ Any Gleason T N M Any PSA Gleason ≥8 III T3a-b N M Any PSA Any Gleason IV T N M Any PSA Any Gleason Any T N M0 Any PSA Any Gleason Any T Any N M Any PSA Any Gleason
 (N) (M) PSA Gleason. I T1a-c N0 M0 PSA <10 Gleason ≤6. T2a N0 M0 PSA <10 Gleason ≤6. T1-2a N0 M0 PSA X Gleason X. IIA T1a-c N0 M0 PSA <20 Gleason 7. T1a-c N0 M0 PSA ≥10<20 Gleason ≤6. T2a N0 M0 PSA <20 Gleason ≤7. T2b N0 M0 PSA <20 Gleason ≤7. T2b N0 M0 PSA X Gleason X. IIB T2c N0 M0 Any PSA Any Gleason. T1-2 N0 M0 PSA ≥20 Any Gleason. T1-2 N0 M0 Any PSA Gleason ≥8. III T3a-b N0 M0 Any PSA Any Gleason. IV T4 N0 M0 Any PSA Any Gleason. Any T N1 M0 Any PSA Any Gleason. Any T Any N M1 Any PSA Any Gleason.")
4
Risk stratification • Low risk — Clinical stage T1c or T2a AND a serum PSA <10 ng/mL AND a biopsy Gleason score ≤6 (anatomic stage prognostic group I) • Intermediate risk — Clinical stage T2b OR a serum PSA between 10 and 20 ng/mL OR a biopsy Gleason score 7 (anatomic stage prognostic group IIA) • High risk — Clinical stage T2c disease OR a serum PSA >20 ng/mL, OR a biopsy Gleason score ≥8 (anatomic stage prognostic group IIB)
 • Intermediate risk — Clinical stage T2b OR a serum PSA between 10 and 20 ng/mL OR a biopsy Gleason score 7 (anatomic stage prognostic group IIA) • High risk — Clinical stage T2c disease OR a serum PSA >20 ng/mL, OR a biopsy Gleason score ≥8 (anatomic stage prognostic group IIB)")
5
Treatment shedules EBRT : Brachytherapy : RADICAL PROSTATECTOMY
Indications : T1,/T2 some T3 Side Effects : Urinary incontinence, Impotence EBRT : Indications : T1/T4 Conformal, 3D , IMRT Brachytherapy : LDR (Seeds) HDR (Ir 192)
 HDR (Ir 192)")
6
Indications

7
Treatment options for localized prostate cancer
The Urologist’ s point of view by country ? by hospital? by specialty ? Differences in patients: age (biologic), condition, QL--issues… Differences: individual patient: Anatomy,, erectile function… Patient selection / Education Cure potentials, Treatment Options
, condition, QL--issues… Differences: individual patient: Anatomy,, erectile function… Patient selection / Education. Cure potentials, Treatment Options.")
8
Equivalence between BT / EBT and Radical Prostatectomy
BT advantages : PTV = CTV - Real dose escalation (144 Gy) - Fast treatment (/ERT) - Low impotency rate (<RP and ERT) - Low rectitis rate (/RTE) - Low urinary complications (/RP)
 - Fast treatment (/ERT) - Low impotency rate (<RP and ERT) - Low rectitis rate (/RTE) - Low urinary complications (/RP)")
9
Practical advantages of temporary HDR prostate brachytherapy
Radioprotection – no free live sources – no risk of source loss – no radioprotection issues after discharge Cheap: utilises existing HDR source and equipment In some centers may be outpatient procedure

10
Physical advantages of temporary HDR prostate brachytherapy
• Brachytherapy enables localized high dose with reduced dose to critical normal tissues – rectum, bladder, small bowel • Uses volume definition after implant; can be customised to individual volume with no organ movement. Can implant larger volume than permanent implant with certain dose delivery including extracapsular region and seminal vesicles

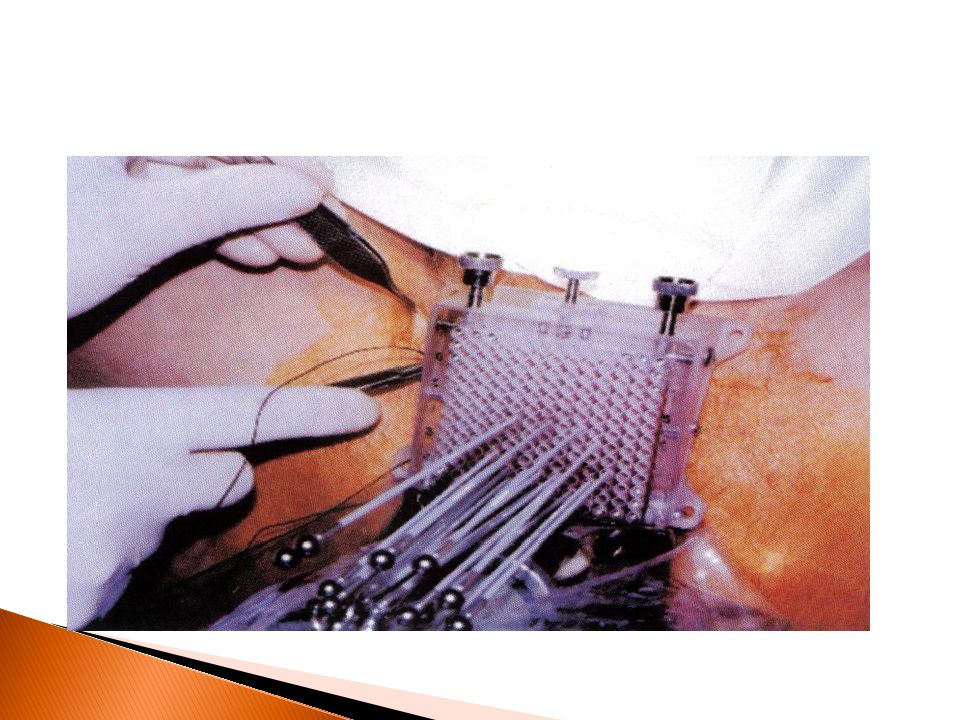
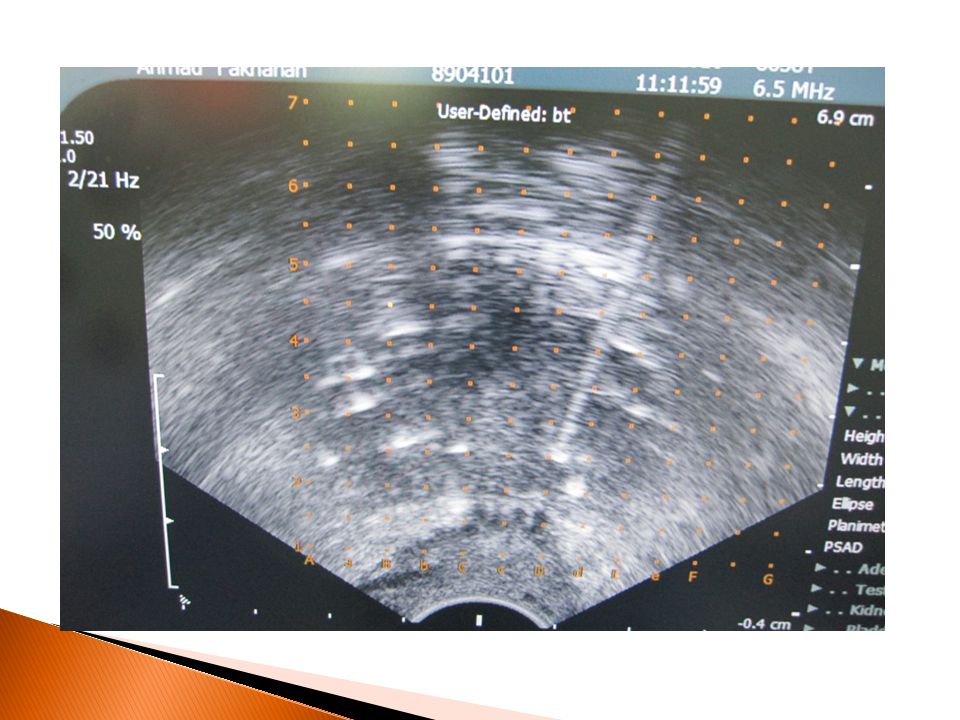
11
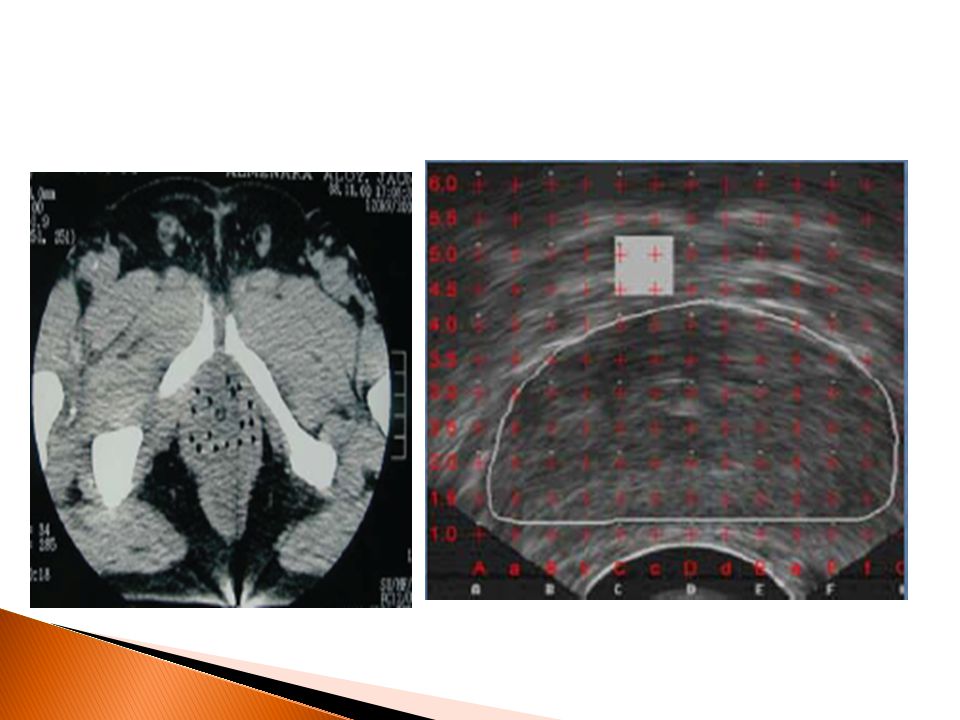
HDR implant: volume definition

13
HDR implant: biological advantage 2Gy EQD

14
Selection Criteria for Using HDR Brachytherapy in Patients With Prostate Cancer
Inclusion criteria Tumor stages T1-T3b Tumor invasion of bladder neck Any Gleason score Any PSA level Prostate volume ≤60-80 cc Possible exclusion criteria Distant metastases Life expectancy <5 y Substantial urinary obstruction Inability to implant entire prostate Patient unfit for anesthesia TURP within previous 6 mo Rectum-prostate distance <5 mm

15
HDR As Salvage (up To 76 Gy)
Indications and Patient selection for HDR-Brachytherapy(GEC- ESTRO) Recommendations HDR As Boost To EBRT: Stage >=T2B or, PSA>10 or GS>=7(intermediate/ Highrisk HDR As Monotherapy: Stage =<T2a and PSA=< 10 and GS=<7 (low risk HDR As Salvage (up To 76 Gy) No Mts, Biopsy confirmation, PSA relapse, Antianrogen resistance or intolerance
 Recommendations. HDR As Boost To EBRT: Stage >=T2B or, PSA>10 or GS>=7(intermediate/ Highrisk. HDR As Monotherapy: Stage =<T2a and PSA=< 10 and GS=<7 (low risk. HDR As Salvage (up To 76 Gy) No Mts, Biopsy confirmation, PSA relapse, Antianrogen resistance or intolerance.")
16
Indications for HDR prostate brachytherapy BOOST

19
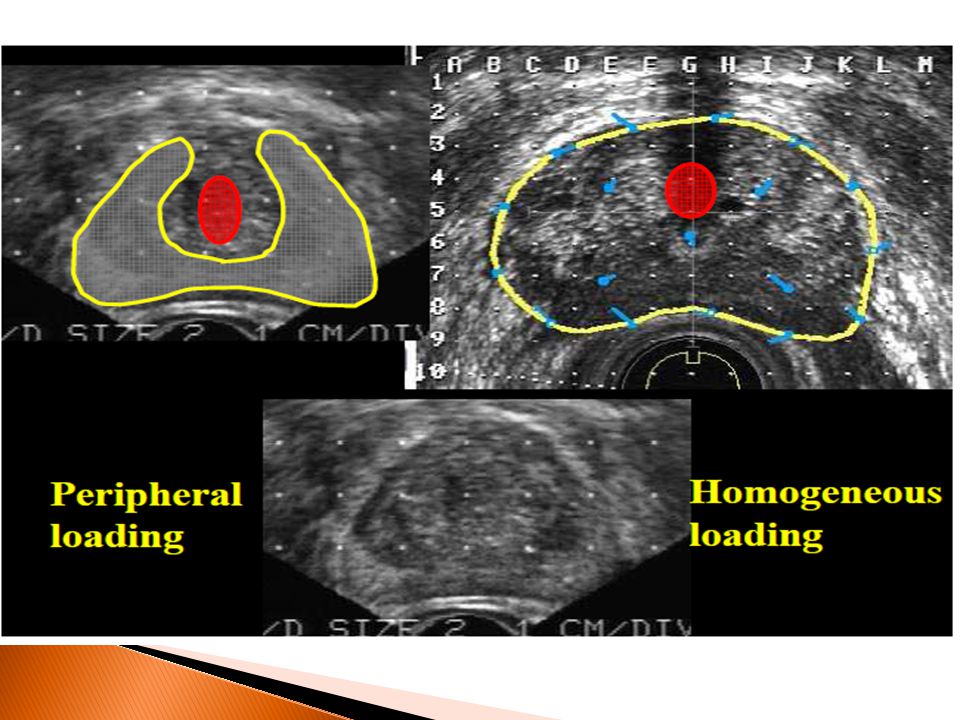
CTV criteria GEC ESTRO guidelines
• CTV1: whole gland defined by capsule – Margin around capsule may be added 3 –5 mm • CTV2: peripheral zone • CTV3: GTV • PTV = CTV

20
OAR criteria GEC ESTRO guidelines
• Urethral dose <10Gy per fraction • Rectal dose <6Gy per fraction

23
Intermediate risk prostate cancer External beam +HDR boost
– Highest overall BED – Includes advantages of regional irradiation by external beam – Includes advantages of conformality with HDR including extracapsular and seminal vesicle areas – Optimal therapeutic ratio – Dose delivery reliable

25
Dose and Fractions HDR Boost :PTV= CTV1 HDR Monotherapy : PTV=CTV1
45Gy EBRT + 2 implants (10.5 Gy*2) BED >94-100 HDR Monotherapy : PTV=CTV1 2 implants , 2* 9.5 Gy/implant total 38 Gy in 2 weeks BED =100 Gy HDR Salvage : 4 implants * 6 Gy = 24 Gy in 12 weeks
 BED > HDR Monotherapy : PTV=CTV1. 2 implants , 2* 9.5 Gy/implant total 38 Gy in 2 weeks BED =100 Gy. HDR Salvage : 4 implants * 6 Gy = 24 Gy in 12 weeks.")
26
EBRT + Boost : Less Failure, Less Toxicity
Results HDR Boost : Late toxicity : Rectum EBRT (76 Gy ) EBRT+HDRBoost(86Gy) Grade % % Grade % % Grade % (Bleeding) % Grade % Bladder Grade % % Grade % % Grade % % Grade EBRT + Boost : Less Failure, Less Toxicity
 EBRT+HDRBoost(86Gy) Grade 0 81% 96% Grade 1 6.7% 1.3% Grade % (Bleeding) 2.7 % Grade 3 0.4% -- Bladder. Grade 0 91% 90% Grade 1 1.3% 1.8% Grade 2 8.5% 8.5% Grade EBRT + Boost : Less Failure, Less Toxicity.")
27
LONG-TERM COMPLICATIONS ?
Brachy (a) RRP XRT Urethritis % N/A % Stricture % % % Incontinence <1% (b) - 30 (c) % % Rectal/proctitis 5% N/A % Impotence: < % % d 60 – % % d vs. 70% (e) 30% > % % d (a) No pre-implant TURP (b) Center of excellence (c) Population studies (d) Nerve sparing (e) Non-nerve sparing
 RRP XRT. Urethritis 5% N/A 3% Stricture 6% 5% 6% Incontinence <1% 5 (b) - 30 (c) % 1% Rectal/proctitis 5% N/A 9% Impotence: < 60 10% 25% d. 60 – 70 20% 35% d vs. 70% (e) 30% > 70 40% 50% d. (a) No pre-implant TURP. (b) Center of excellence. (c) Population studies. (d) Nerve sparing. (e) Non-nerve sparing.")
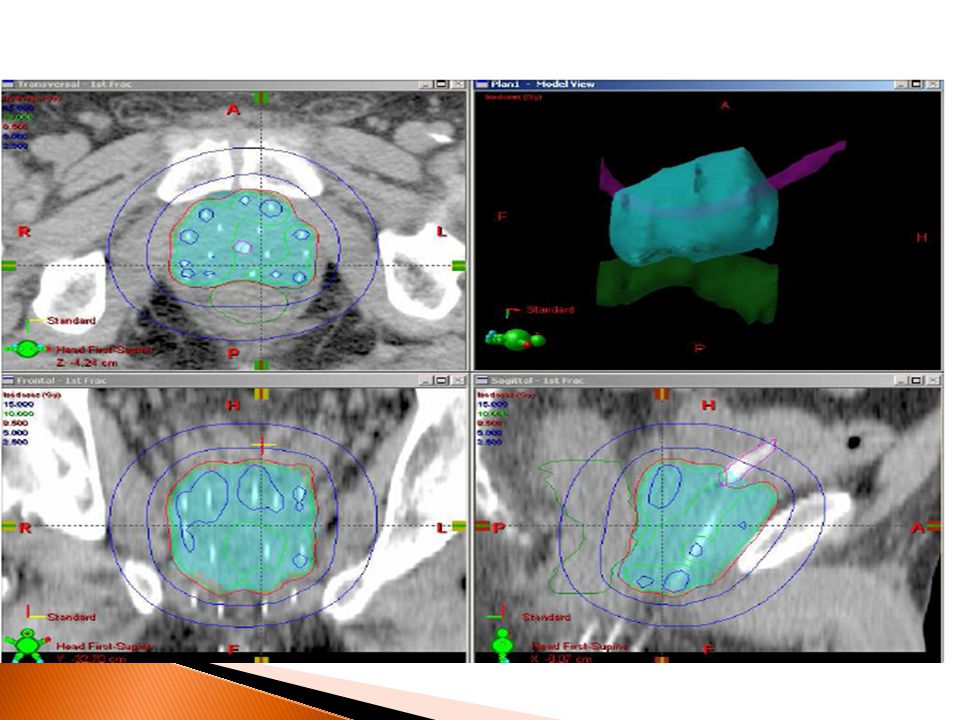
31
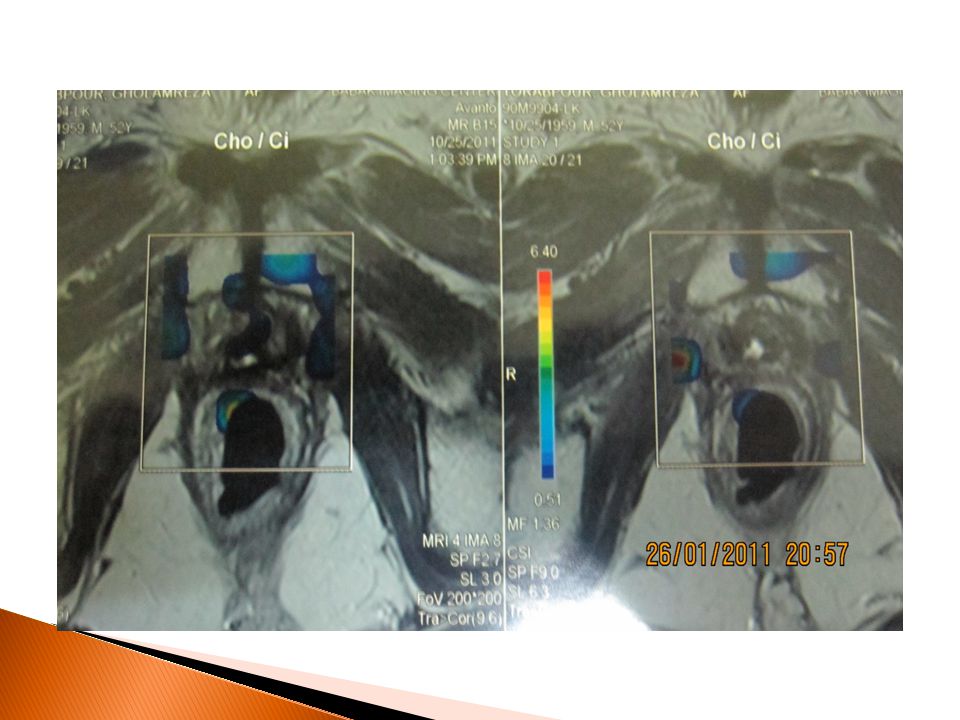
Target Volume Delineation

32
HDR Monotherapy for Localised Prostate Cancer
HDR brachytherapy is an established technique enabling high dose delivery to prostate gland HDR brachytherapy has potential advantages especially for more advanced prostate cancer – Physical implant flexibility – Biological advantage of large fractions

33
HDR Monotherapy for Localised Prostate Cancer Conclusions
HDR monotherapy is feasible and can deliver 4 fractions over 3 days with one implant procedure Acute toxicity is limited to transient urinary disturbance, returning to baseline at 12 weeks Early biochemical results for advanced disease are encouraging. Further dose escalation is possible or necessary

36
Post operative follow up
Foley catheter removed on Day 2 No residual pain Recommandations/information Acute effects Irritation syndrome Retentionnal syndrome Radiation hazards

37
HDR Monotherapy : OS; 98.9% ,PSA Specific control :100%, Biochemical control : 97.2% GU Toxicity GI Toxicity Grade0 34% % Grade % % Grade % Grade %

Similar presentations














: The optimal indication for operable tumors in inoperable patients D.Katsochi 1, S.Kosmidis 1, A.Fotopoulou.>")

 KSMC.>")








.>")