Download presentation
Presentation is loading. Please wait.

1
Ectopic Pregnancy Xiaofang Yi, M.D.
Hospital of OB/GYN, Fudan University Mobile: Good afternoon everyone. I’m Dr. Yi, coming from Hospital of OB/GYN, which is also named as Redhouse Hospital. Before we start the class, I’d like to briefly introduce myself to you. I got my M.D. degree in 1996, and Ph.D degree in Between 2006 and 2008, I had two-year postdoc training in United States. Currently, I’m serving as associate professor in Redhouse Hospital. My major is in Gynecology and Gynecologic Oncology. I hope you’ll like attending my class. If you have any questions during the class, please don’t hesitate to stop me and ask. In this class, I’m going to introduce two emergency conditions, ectopic pregnancy and abortion. Since the risk of death for women with ectopic pregnancy is greater than any other conditions, we’ll spend more time to study this disease.

2
Abbreviations STD: sexually transmitted disease
ART: assisted reproductive technique hCG: human chorionic gonadotropin TVS: transvaginal sonography MTX: methotrexate Before we start, I’d like you to master these abbreviations, they’re also key words for this class. STD and ART are related to the risk factors of ectopic pregnancy, hCG and TVS are used to diagnose this disease, while MTX is an important medicine to treat the disease.

3
Contents 1. Definition 2. Classification 3. Epidemiology
4. Risk Factors 5. Tubal Pregnancy In this class, we’re going to learn the definition and classification of ectopic pregnancy. The epidemiology and risk factors are also to be discussed. We’ll majorly focus on tubal pregnancy, but briefly talk about other site of ectopic pregnancy. 6. Other Site of Ectopic Pregnancy

4
Definition “ektopos”=out of place
Implantation of blastocyst not in the endometrial lining of the uterine cavity Ectopic pregnancy is derived from the Greek “ektopos”, which means “out of place”. Normally the blastocyst implants in the endometrial lining of the uterine cavity, implantation anywhere else is considered ectopic pregnancy.

5
Classification Tubal pregnancy (95%) Ovarian ~ Cornual ~ Cervical ~
Abdominal ~ Ceasarean scar ~ Heterotopic ~, etc. Ectopic pregnancy can be classified as tubal…,….Nearly 95% ~ are implanted in fallopian tubes. Occasionally, usually with ART, multifetal pregnancies can be seen, with one ectopic, the other intrauterine, which is called heterotopic pregnancy.

6
Epidemiology 2% of all early pregnancies
10% of repeat ectopic pregnancy 6% of all pregnancy-related deaths Mortality ratio in black 18 times higher than in white women According to ACOG 2008, 2% of first trimester pregnancies are ectopic, and this accounts for 6% of all pregnancy-related deaths. It’s more commonly seen in black than in white women. After one previous ectopic pregnancy, the chance of another is approximately 10%.

7
Risk Factors Prior tubal damage, either from a previous tubal pregnancy, or from tubal surgery, confers the highest risk for ectopic pregnancy.

8
Tubal Pregnancy Because nearly 95% of ectopic pregnancies are tubal pregnancy, in the later 30 minutes, we’ll focus on this disease. Here shows the various segments of the fallopian tube. The fertilized ovum may lodge in any portion of the oviduct, giving rise to ampullary, isthmic, and interstitial tubal pregnancies. The ampulla is the most frequent site, followed by the isthmus. Interstitial pregnancy accounts for only about 2%. This is captured by laparoscope, could you tell me where is the lesion? Which portion did it locate?

9
Endings of tubal pregnancy
Rupture:Isthmic, 12~16 wks Abortion:Ampullary, 8~12 wks Secondary abdominal pregnancy Broad ligament pregnancy Persistent ectopic pregnancy Because the tube lacks a submucosal layer, the rapidly proliferating trophoblast may invade the subjacent muscularis, and rupture the oviduct. If a patient didn’t get earlier diagnosis, she might suffer from the endings of tubal pregnancy, such as …. Abortion is common in ampullary pregnancies, while rupture is the usual outcome with isthmic pregnancies.

10
Clinical Manifestations
Delayed menstruation Vaginal bleeding or spotting Abdominal & pelvic pain Sharp, stabbing, or tearing With vasomotor disturbance: vertigo to syncope Tenderness Pelvic mass: tender, boggy Diaphragmatic irritation: pain in neck or shoulder Women with a tubal pregnancy have diverse clinical manifestations that largely depend on whether there is rupture. Typically, a woman assumes she has a normal pregnancy or having a miscarriage is there is delayed menstruation and vaginal bleeding or spotting. When rupture, there is usually sever lower abdominal and pelvic pain. If there is sizable intraperitoneal heamorrhage, symptoms of diaphragmatic irritation may develop, characterized by pain in neck or shoulder.

11
Often subtle or even absent Pain, bleeding, tenderness
Before rupture Pain, bleeding, tenderness Rupture Symptoms and signs of ectopic pregnancy are often subtle or even absent. But when rupture, there’re usually symptoms, and signs of hypovolemia are common.

12
Symptoms and Signs Pain: 95% Abnormal bleeding: 60-80%
Abdominal & pelvic tenderness Uterine changes: pushed to one side, enlarged Vital signs: BP will fall, P will rise only when hypovolemia Pelvic and abdominal pain are reported by 95% of women with tubal pregnancy. Amenorrhea with some degree of vaginal bleeding or spotting is reported by 60-80% of women with tubal pregnancy. With rupture, there’re usually symptoms, and signs of hypovolemia are common.

13
Laboratory Tests hCG: the rise over 48 hours ﹤ 66%
Progesterone: ng/ml Hemogram: decrease in hemoglobin or hematocrit Sonography:TVS Culdocentesis Uterine currettage Laparoscopy / laparotomy To make diagnosis for women with complaints suggestive of ectopic pregnancy, rapid and accurate determination of pregnancy is essential. In greater than 99% of ectopic pregnancy serum and urine pregnancy tests are positive. A value of progesterone exceeding 25 ng/ml excludes ectopic pregnancy with 92.5% sensitivity. Values <5 ng/mL suggest either an intrauterine pregnancy with a dead fetus or an ectopic pregnancy. After an acute hemorrhage, a decrease in hemoglobin or hematocrit level over several hours is a more valuable index of blood loss than is the initial level. High-resolution transvaginal sonography has revolutionized the care of women with suspected ectopic pregnancy. Culdocentesis is a simple technique, which was used commonly in the past to identify hemoperitoneum. Distinction between a nonliving intrauterine and an ectopic pregnancy is made by uterine curettage. Some do not recommend diagnostic curettage as shown in the diagnostic algorithm because it results in unnecessary medical or surgical therapy for ectopic pregnancy. Direct visualization of the fallopian tubes and pelvis by laparoscopy offers a reliable diagnosis in most cases of suspected ectopic pregnancy.

14
Arias-Stella reaction
Glands: closely packed , hypersecretory. Nuclei: large, hyperchromatic. The Arias-Stella reaction of the endometrium. The glands are closely packed and hypersecretory with large, hyperchromatic nuclei suggesting malignancy. The Arias-Sella reaction is a nonspecific finding that can be seen in patients with intrauterine pregnancies

15
Laboratory Tests hCG: the rise over 48 hours ﹤ 66%
Progesterone: ng/ml Hemogram: decrease in hemoglobin or hematocrit Sonography:TVS Culdocentesis Uterine currettage Laparoscopy / laparotomy Sonography is very helpful to make the early diagnosis for ectopic pregnancy. It has decreased the need for diagnostic laparoscopy and/or curettage to establish the diagnosis of ectopic pregnancy.

16
TVS Findings Endometrial cavity Adnexa Rectouterine cul-de-sac
Pseudogestational sac Decidual cyst Adnexa Extrauterine yolk sac or embryo: 15-30% Adnexal mass: PPV 96%, NPV 95% Rectouterine cul-de-sac Free peritoneal fluid Caution in diagnosing an intrauterine pregnancy in the absence of definite yolk sac or embryo A trilaminar endometrial pattern is unique for diagnosis of ectopic pregnancy—its specificity is 94 percent, but with a sensitivity of only 38 percent (Hammoud and associates, 2005). Anechoic fluid collections, however, which would normally suggest an early intrauterine gestational sac, may also be seen with ectopic pregnancy. These include pseudogestational sac and decidual cyst. When fallopian tubes and ovaries are visualized and an extrauterine yolk sac or embryo is identified, a tubal pregnancy is clearly confirmed (Fig. 10-6). But, such findings are present in only 15 to 30 percent of cases (Paul and co-workers, 2000). In their meta-analysis of 10 studies, Brown and Doubilet (1994) reported that the finding of any adnexal mass, other than a simple ovarian cyst, was the most accurate sonographic finding. Free peritoneal fluid suggests intra-abdominal bleeding. As little as 50 mL can be seen in the cul-de-sac using the transvaginal transducer. Detection of peritoneal fluid in conjunction with an adnexal mass is highly predictive of ectopic pregnancy (Nyberg and associates, 1991).
. Anechoic fluid collections, however, which would normally suggest an early intrauterine gestational sac, may also be seen with ectopic pregnancy. These include pseudogestational sac and decidual cyst. When fallopian tubes and ovaries are visualized and an extrauterine yolk sac or embryo is identified, a tubal pregnancy is clearly confirmed (Fig. 10-6). But, such findings are present in only 15 to 30 percent of cases (Paul and co-workers, 2000). In their meta-analysis of 10 studies, Brown and Doubilet (1994) reported that the finding of any adnexal mass, other than a simple ovarian cyst, was the most accurate sonographic finding. Free peritoneal fluid suggests intra-abdominal bleeding. As little as 50 mL can be seen in the cul-de-sac using the transvaginal transducer. Detection of peritoneal fluid in conjunction with an adnexal mass is highly predictive of ectopic pregnancy (Nyberg and associates, 1991).")
17
The “ring of fire” Vaginal sonogram of an ectopic pregnancy. A. The uterus (Ut) is seen with a normal endometrial stripe (ES). A small amount of free fluid (FF) is visible in the posterior cul-de-sac. B. The tubal ectopic pregnancy (EP) with its yolk sac (YS) is seen along with a corpus luteum (CL) cyst. Color Doppler transvaginal sonogram of an ectopic pregnancy. The "ring of fire" reflects placental blood flow around the periphery of the pregnancy. This finding may also be seen with a corpus luteum cyst.
 is seen with a normal endometrial stripe (ES). A small amount of free fluid (FF) is visible in the posterior cul-de-sac. B. The tubal ectopic pregnancy (EP) with its yolk sac (YS) is seen along with a corpus luteum (CL) cyst. Color Doppler transvaginal sonogram of an ectopic pregnancy. The ring of fire reflects placental blood flow around the periphery of the pregnancy. This finding may also be seen with a corpus luteum cyst.")
18
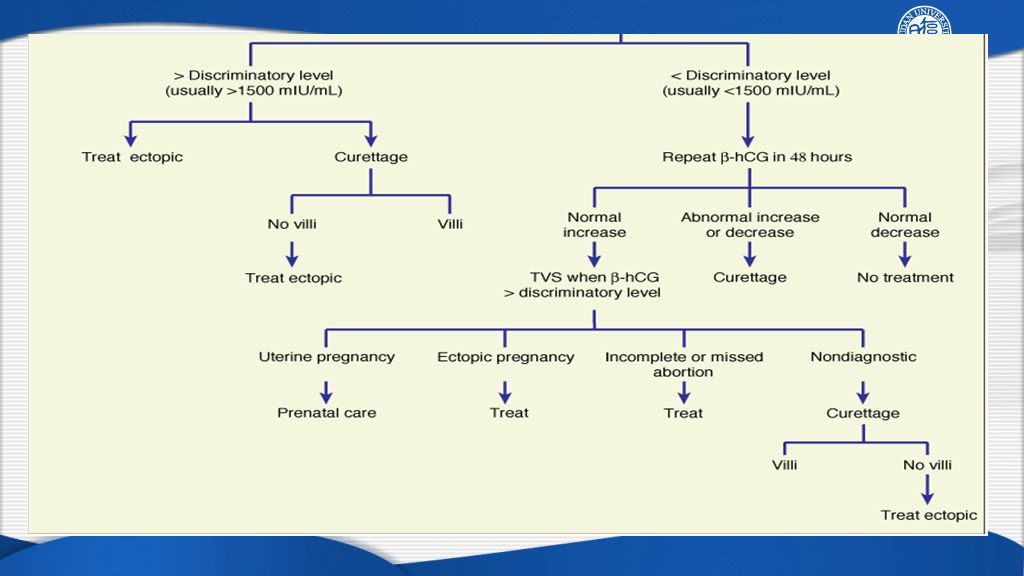
Discriminatory hCG Serial assays of hCG, w/ serial TVS evaluation
Empty uterus w/ hCG > 1500 mIU/mL Ectopic pregnancy Nonliving uterine pregnancy Early multifetal gestation Serial assays of hCG, w/ serial TVS evaluation <66% increase within 48hr Empty uterus If the initial -hCG level exceeds the discriminatory level—1500 mIU/mL in this case, and no live intrauterine pregnancy is seen with TVS, then the diagnosis is narrowed to an intrauterine pregnancy with a dead fetus versus an ectopic pregnancy. Early multifetal gestation, of course, remains a possibility. Kadar and Romero (1987) reported that mean doubling time for serum -hCG levels with early normal pregnancy was approximately 48 hours. The lowest normal value for this increase was 66 percent. Failure to maintain this minimum rate of increased -hCG production, along with an empty uterus, is suggestive of an ectopic pregnancy or completed abortion.
 reported that mean doubling time for serum -hCG levels with early normal pregnancy was approximately 48 hours. The lowest normal value for this increase was 66 percent. Failure to maintain this minimum rate of increased -hCG production, along with an empty uterus, is suggestive of an ectopic pregnancy or completed abortion.")
19
Differential Diagnosis
Abortion Pelvic inflammation disease Appendicities Rupture of corpus luteum Torsion of ovarian cyst

20
allows definitive surgical or medical management
Early diagnosis allows definitive surgical or medical management Treatment before rupture Less morbidity, mortality, better prognosis for fertility Treatment before rupture is associated with less morbidity and mortality and a better prognosis for fertility.

21
Surgical Management (1/3)
C1: Laparoscopy or laparotomy ? Tubal patency following salpingostomy Subsequent uterine pregnancies Subsequent ectopic pregnancies Safety & cost: operative time, blood loss, analgesic requirements, hospital stays Laparoscopy is the preferred surgical treatment for ectopic pregnancy unless the woman is hemodynamically unstable. No significant difference were seen in the following aspects.

22
Laparoscopy vs Laparotomy
Longer OP time Limitaion in Manipulation 2-Dimensional Image Expensive Eye-Hand Discrepancy Less Pain Early recovery Smaller Scar Less Bleeding Early return to work Less adhesion Short Hospital Stay Magnification of OP field Advantage in Immunology LAPAROSCOPIC SURGERY

23
Surgical Management (2/3)
C2: Conservative or radical? Subsequent uterine pregnancies Persistent ectopic pregnancies Indications for conservative surgery < 3 cm in length Unruptured hCG < 3000 mIU/mL Hemodynamically stable Tubal surgery is considered conservative when there is tubal salvage. Radical surgery is defined by salpingectomy. Conservative surgery may increase the rate of subsequent uterine pregnancy but is associated with higher rates of persistently functioning trophoblast (Bangsgaard and colleagues, 2003).
.")
24
Surgical Management (3/3)
C3: Surgical types? Salpingostomy Salpingotomy: suture the tubal incision Salpingectomy Cornual resection

25
Salpingostomy Salpingotomy
Salpingostomy is used to remove a small pregnancy that is usually less than 2 cm in length and located in the distal third of the fallopian tube. Linear incision for removal of a small tubal pregnancy is created on the antimesenteric border of the tube. Products of conception may be flushed from the tube using an irrigation probe. Alternatively, products may be removed with grasping forceps. Following evacuation of the tube, bleeding sites are treated with electrosurgical coagulation or laser, and the incision is not sutured. If the incision is closed, the procedure is termed a salpingotomy. Natale and associates (2003) reported that serum -hCG levels > 6000 mIU/mL are associated with a higher risk of implantation into the muscularis and thus with more tubal damage. According to Tulandi and Saleh (1999), there is no difference in prognosis with or without suturing
 reported that serum -hCG levels > 6000 mIU/mL are associated with a higher risk of implantation into the muscularis and thus with more tubal damage. According to Tulandi and Saleh (1999), there is no difference in prognosis with or without suturing.")
26
Salpingectomy When removing the oviduct, it is advisable to excise a wedge of the outer third (or less) of the interstitial portion of the tube. This so-called cornual resection is done in an effort to minimize the rare recurrence of pregnancy in the tubal stump.
 of the interstitial portion of the tube. This so-called cornual resection is done in an effort to minimize the rare recurrence of pregnancy in the tubal stump.")
27
Cornual Resection Cornual ectopic pregnancy. A. Transvaginal sonogram, parasagittal view shows an empty uterine cavity (white arrows) and a mass lateral to the uterine fundus (red arrow). (Courtesy of Dr. Elysia Moschos.) B. Intraoperative photograph during cornual resection of an ectopic pregnancy. A Pean clamp is placed across the round ligament, uteroovarian ligament, and fallopian tube distal to the cornual pregnancy (white arrow). The surgeon is injecting a dilute vasopressin solution at the cornual base prior to incision. (Used with permission from Dr. Marlene Corton.)
 and a mass lateral to the uterine fundus (red arrow). (Courtesy of Dr. Elysia Moschos.) B. Intraoperative photograph during cornual resection of an ectopic pregnancy. A Pean clamp is placed across the round ligament, uteroovarian ligament, and fallopian tube distal to the cornual pregnancy (white arrow). The surgeon is injecting a dilute vasopressin solution at the cornual base prior to incision. (Used with permission from Dr. Marlene Corton.)")
28
Persistent Ectopic Pregnancy
Post-op day 1: hCG > 50% of the pre-op value Post-op day 12: hCG > 10% of the pre-op value Risk factors Small pregnancies: < 2 cm Early therapy: before 42 menstrual days hCG > 3000 mIU/mL Implantation medial to the salpingostomy site Additional surgical or medical therapy is necessary Incomplete removal of trophoblast may result in persistent ectopic pregnancy. Persistent trophoblast complicates 5 to 20 percent of salpingostomies and can be identified by persistent or rising hCG levels. In the face of persistent or increasing -hCG, additional surgical or medical therapy is necessary.

29
Medical Management Indications Contraindication
Asymptomatic, motivated, compliant Mass ≤ 3.5 cm hCG< 2000 mIU/mL Contraindication Active intra-abdominal hemorrhge Intrauterine pregnancy Breast feeding Immunodeficiency, alcoholism Chronic hepatic, renal, or pulmonary disease Blood dyscrasias Peptic ulcer disease This folic acid antagonist is highly effective against rapidly proliferating trophoblast, and it has been used for more than 40 years to treat gestational trophoblastic disease. Tanaka and associates (1982) first used methotrexate to treat an interstitial pregnancy, and since then, it has been used successfully for all varieties of ectopic pregnancy.
 first used methotrexate to treat an interstitial pregnancy, and since then, it has been used successfully for all varieties of ectopic pregnancy.")
30
Methotrexate (MTX) Folic acid antagonist Dose & administration
Toxicity Liver: 12% Stomatitis: 6% Gastroenteritis: 1% Failure rate: 1.5% (hCG <1000 mIU/mL) 14.3% (hCG > 5000 mIU/mL) 80 percent of these women required only one dose. About 15 to 20 percent of women require a second dose of methotrexate. Adverse effects were resolved by 3 to 4 days after methotrexate was discontinued. 20 percent of women given single-dose methotrexate will have significant pain, and 20 percent of these will require laparoscopy.
 14.3% (hCG > 5000 mIU/mL) 80 percent of these women required only one dose. About 15 to 20 percent of women require a second dose of methotrexate. Adverse effects were resolved by 3 to 4 days after methotrexate was discontinued. 20 percent of women given single-dose methotrexate will have significant pain, and 20 percent of these will require laparoscopy.")
31
MTX Therapy Surgical treatment if -hCG levels not decreasing or fetal cardiac activity persists after three doses methotrexate.

32
Monitoring Efficacy of Therapy
“15%, day 4 and 7 rule” Weekly serum hCG determination until undetectable Resolution time Salpingostomy: 20 days Single-dose MTX: days Rupture of persistent ectopic pregnancy: 5-10% The longest resolution time: 109 days Kirk and colleagues (2007) recently confirmed the efficacy of the "15 percent, day 4 and 7 rule." With variable-dose methotrexate, levels are measured at 48-hour intervals until they fall more than 15 percent. Tubal rupture can occur in the face of declining hCG.
 recently confirmed the efficacy of the 15 percent, day 4 and 7 rule. With variable-dose methotrexate, levels are measured at 48-hour intervals until they fall more than 15 percent. Tubal rupture can occur in the face of declining hCG.")
33
Schematic of comparative patterns of serum-hCG level decline after single-dose methotrexate treatment or laparoscopic salpingostomy for unruptured ectopic pregnancy. Values are approximate. Yellow area is range between mean values reported by aSaraj and colleagues (1998) and those reported by bDilbaz and associates (2006). Gray area represents area under the curve for mean values following salpingostomy reported by aSaraj and colleagues (1998).
 and those reported by bDilbaz and associates (2006). Gray area represents area under the curve for mean values following salpingostomy reported by aSaraj and colleagues (1998).")
34
Expectant treatment Resolution rate: Indications
Tubal ectopic pregnancies only Decreasing serial hCG levels Mass ≤ 3.5 cm TVS: no intra-abdominal bleeding or rupture Resolution rate: hCG < 1000 mIU/mL: 50-73% hCG < 200 mIU/mL: 88% ThIn appropriately selected cases, it is reasonable to observe very early tubal pregnancies that are associated with stable or falling serum -hCG levels. e failure rate is similar for either medical or surgical management.

35
With expectant management, subsequent rates of tubal patency and intrauterine pregnancy are comparable with surgery and medical management.

36
Other Sites of Ectopic Pregnancies

37
Abdominal Pregnancy Incidence: 1 in 85,000
Symptoms: vague, nonspecific Sonography, MRI: might be helpful Life threatening Pre-op angiographic embolization Surgical termination Strictly defined, abdominal pregnancy is an implantation in the peritoneal cavity exclusive of tubal, ovarian, or intraligamentary implantations. Fig. Abdominal pregnancy at term. The placenta is implanted on the posterior surface of the uterus and broad ligament. The enlarged, flattened uterus is located just beneath the anterior abdominal wall. The cervix and vagina are dislodged anteriorly and superiorly by the large fetal head in the cul-de-sac. Termination generally is indicated when the diagnosis is made.

38
Ovarian Pregnancy Symptoms: Mimic tubal pregnancy or a bleeding corpus luteum Surgery: Ovarian wedge resection Cystectomy Ovariectomy MTX: if unruptured

39
Cervical Pregnancy Incidence: 1 in 18,000
Clinical feature:painless vaginal bleeding Treatment: Cerclage Curretage and tamponade Arterial embolization Laparoscopically assisted uterine artery ligation followed by hysteroscopic endocervial resection MTX: mg/m2 Sonographically guided fetal intracardiac injection of 2 mL KCl was added when needed Intracervical Foley catheter was placed for 3 days Painless vaginal bleeding is reported by 90 percent of women with a cervical pregnancy—a third of these have massive hemorrhage (Ushakov and colleagues, 1997). Only a fourth have abdominal pain with bleeding.
. Only a fourth have abdominal pain with bleeding.")
40
TVS of a cervical pregnancy.
(1) an hourglass uterine shape and ballooned cervical canal; (2) gestational tissue at the level of the cervix (black arrow); (3) absent intrauterine gestational tissue (white arrows); (4) a portion of the endocervical canal seen interposed between the gestation and the endometrial canal. In a transverse view of the cervical pregnancy, Doppler color flow shows abundant vascularization. (From Dr. Elysia Moschos.)
 an hourglass uterine shape and ballooned cervical canal; (2) gestational tissue at the level of the cervix (black arrow); (3) absent intrauterine gestational tissue (white arrows); (4) a portion of the endocervical canal seen interposed between the gestation and the endometrial canal. In a transverse view of the cervical pregnancy, Doppler color flow shows abundant vascularization. (From Dr. Elysia Moschos.)")
41
Cesearean Scar Pregnancy
Incidence: 1 in 2,000 Clinical presentation: Pain & bleeding Asymptomatic: 40% Treatment: MTX Curretage Hysteroscopic resection Uterine-preserving rection Hysterectomy

42
TVS shows a uterus with CSP
TVS shows a uterus with CSP. An empty uterine cavity appearing as a bright hyperechoic endometrial stripe (long, white arrow); an empty cervical canal (short, white arrow); and an intracavitary mass seen in the anterior wall of the uterine isthmus (red arrows). (From Dr. Elysia Moschos.) This hysterectomy specimen with a CSP is transversely sectioned at the level of the uterine isthmus and through the gestational sac. (From Drs. Sunil Balgobin, Manisha Sharma, and Rebecca Stone.)
; an empty cervical canal (short, white arrow); and an intracavitary mass seen in the anterior wall of the uterine isthmus (red arrows). (From Dr. Elysia Moschos.) This hysterectomy specimen with a CSP is transversely sectioned at the level of the uterine isthmus and through the gestational sac. (From Drs. Sunil Balgobin, Manisha Sharma, and Rebecca Stone.)")
43
Heterotopic pregnancy
A condition in which ectopic and intrauterine pregnancies coexist. Incidence: 1 in

44
Summary

45
Summary

47
Abortion As many as 30% of pregnancies may be spontaneously lost.

48
Contents 1. Definition 2. Type of abortion 3. Etiology 4. Diagnosis
5. Management

49
Definition Latin “Aboriri”-”to miscarry”
A pregnancy termination prior to 20 weeks of gestation, or with a fetus born weighing < 500 g. China: 28 wks, 1000g Vary widely.

50
Type of Abortion Spontaneous abortion Induced abortion Septic abortion
Recurrent spontaneous abortion: The loss of more than three pregnancies before 20 weeks of gestation About 15% to 20% of known pregnancies terminate in spontaneous abortion. With the use of serial human chorionic gonadotropin (hCG) measurements to detect early subclinical pregnancy losses, the percentage increases to 30%. About 80% of spontaneous pregnancy losses occur in the first trimester; the incidence decreases with each gestational week.
 measurements to detect early subclinical pregnancy losses, the percentage increases to 30%. About 80% of spontaneous pregnancy losses occur in the first trimester; the incidence decreases with each gestational week.")
51
Type of Spontaneous Abortion
Threatened ~:Vaginal bleeding before 20 weeks of gestation. Inevitable ~: Uterine bleeding from a gestation of less than 20 weeks, accompanied by cervical dilation but without expulsion of placental or fetal tissue through the cervix. Anembryonic gestation: An intrauterine sac without fetal tissue present at more than 7.5 weeks of gestation. Incomplete ~: Expulsion of some but not all of the products of conception before 20 completed weeks of gestation. Complete ~: Spontaneous expulsion of all fetal and placental tissue from the uterine cavity before 20 weeks of gestation. Missed ~ About 15% to 20% of known pregnancies terminate in spontaneous abortion. With the use of serial human chorionic gonadotropin (hCG) measurements to detect early subclinical pregnancy losses, the percentage increases to 30%. About 80% of spontaneous pregnancy losses occur in the first trimester; the incidence decreases with each gestational week. There is no effective therapy for a threatened intrauterine pregnancy. When it is certain that the pregnancy is not viable because the cervical os is dilated or excessive bleeding is present, suction curettage should be performed. Blood type and Rh determination and a complete blood count should be obtained if there is any concern about the amount of bleeding. Before 6 weeks of gestation, the placenta and fetus are generally passed together, but after this time, they often are passed separately. If the patient is febrile, broad-spectrum antibiotic therapy should be administered before suction curettage is performed to reduce the incidence of postabortal endometritis and pelvic inflammatory disease, thereby reducing potential deleterious effects on fertility.
 measurements to detect early subclinical pregnancy losses, the percentage increases to 30%. About 80% of spontaneous pregnancy losses occur in the first trimester; the incidence decreases with each gestational week. There is no effective therapy for a threatened intrauterine pregnancy. When it is certain that the pregnancy is not viable because the cervical os. is dilated or excessive bleeding is present, suction curettage should be performed. Blood type. and Rh determination and a complete blood count should be obtained if there is any concern. about the amount of bleeding. Before 6 weeks of gestation, the placenta and fetus are generally passed together, but after this time, they. often are passed separately. If the patient is febrile, broad-spectrum antibiotic therapy should be administered. before suction curettage is performed to reduce the incidence of postabortal. endometritis and pelvic inflammatory disease, thereby reducing potential. deleterious effects on fertility.")
52
Bleeding Abdominal Pain Tissue Expulsion Cervical Os Uterus Threatened Abortion Inevitable Abortion Incomplete Abortion Complete Abortion Light Mild to heavy Light to heavy Light to none None/light Intensified Relieved None Partial Complete Closed Dilated Dilated or obstructed Normal Normal or slightly small Small Normal or slightly large

53
Etiology Fetal factors Maternal factors:
Infections Chronic debilitating diseases Endocrine anomalies Uterine defects Drug use and environmental factors Paternal factors

54
Symptoms Amenorrhea Vaginal bleeding Abdominal pain

55
Diagnosis History & physical examination Transvaginal ultrasonography
hCG Serum progesterone

56
Endovaginal ultrasonography can detect a gestational sac at an hCG level of 1,000
to 2,000 mIU/mL. By 7 weeks of gestation, a fetal pole with fetal cardiac activity can be seen. When a gestational sac is visualized, subsequent loss of the pregnancy occurs in 11.5% of patients. If a yolk sac is present, the loss rate is 8.5%; with an embryo of 5 mm, the loss rate is 7.2%; with an embryo of 6 to 10 mm, the loss rate is 3.2%; and when the embryo is 10 mm, the loss rate is only 0.5%. The fetal loss rate after 14 weeks of gestation is about 2% (3). Transvaginal measurement of gestational sac size is useful in differentiating viable from nonviable intrauterine pregnancies. A mean sac diameter greater than 13 mm without a visible yolk sac or a mean sac diameter greater than 17 mm lacking an embryo predicts nonviability in all cases (4).
. Transvaginal measurement of gestational sac size is useful in differentiating viable. from nonviable intrauterine pregnancies. A mean sac diameter greater than 13 mm without a. visible yolk sac or a mean sac diameter greater than 17 mm lacking an embryo predicts. nonviability in all cases (4).")
57
Differential Diagnosis
Cervical polyps Vaginitis Cervical carcinoma Gestational trophoblastic disease Ectopic pregnancy Trauma Foreign body

58
Management There is no effective therapy for a threatened intrauterine pregnancy. Bed rest Progesterone? sedative? All patients with an incomplete abortion should undergo suction curettage as quickly as possible. Genetic consulting Cervical cerclage

59
Abortion Techniques

60
A Hegar dilator. Note that the fourth and fifth fingers rest against the perineum and buttocks, lateral to the vagina. Dilatation of cervix with a Hegar dilator. Note that the fourth and fifth fingers rest against the perineum and buttocks, lateral to the vagina. This maneuver is an important safety measure because if the cervix relaxes abruptly, these fingers prevent a sudden and uncontrolled thrust of the dilator, a common cause of uterine perforation. If the bleeding is profuse, the patient should be examined promptly for tissue protruding from the cervical os; removal of this tissue with a ring forceps reduces the bleeding.

61
A suction curette is simultaneously rotated 360° several times to remove tissue circumferentially from the uterine walls. A suction curette is advanced to the uterine fundus and then back to the internal os. During its insertion and retraction, the curette is simultaneously rotated 360° several times to remove tissue circumferentially from the uterine walls.

62
A sharp curette is held with the thumb and forefinger
A sharp curette is held with the thumb and forefinger. In the upward movement of the curette, only the strength of these two fingers should be used. Introduction of a sharp curette. The instrument is held with the thumb and forefinger. In the upward movement of the curette, only the strength of these two fingers should be used.

63
When floated in saline, chorionic villi are often readily distinguishable as lacy fronds of tissue.

64
Regimens for Medical Termination of Early Pregnancy
aDoses of 200 versus 600 mg similarly effective. bOral route may be less effective and with more nausea and diarrhea. May be given sublingually, or buccally. Postprocedure pelvic infection significantly higher with vaginal versus oral route. Possibly more effective when given at hours instead of at 6 hours. cEfficacy similar for routes of administration. dSimilar efficacy when given on day 3 versus day 5.

65
References Williams Obstetrics, 23rd Edition Chapter 10. Ectopic Pregnancy Berek & Novak’s Gynecology, 14th Edition Ectopic Pregnancy and Miscarriage: Diagnosis and Initial Management in Early Pregnancy of Ectopic Pregnancy and Miscarriage. National Institute for Health and Clinical Excellence: Guidance. Editors: National Collaborating Centre for Women's and Children's Health (UK). Source: London: RCOG; 2012 Dec.
. Source: London: RCOG; 2012 Dec.")
66
Quizs If a patient has documented cardiac activity in the ectopic, what should be initiated, MTX or surgery ? How to monitor hCG levels and evaluate transvaginal ultrasound while instituting MTX ? Does surgical management and medical therapy appear to be equivalent ? Summarize the management strategies for tubal pregnancy and its indications. What conditions should be differentiated from abortion?

67
Which statement about ectopic pregnancy is true?
Implantation of the fertilized egg outside the uterine cavity Rarely involves the fallopian tubes Usually associated with cervical carcinoma The most common site of involvement is the ovary Rarely a surgical emergency

68
THANK YOU Xiaofang Yi, M.D. Hospital of OB/GYN, Fudan University
Mobile:

Similar presentations






 Medical therapy method terexate.>")










 Dr Kamel Elbadry MD (Sheffield University), FRCOG MD (Sheffield University), FRCOG Consultant Obstetrician and Gynaecologist.>")

