Download presentation
Presentation is loading. Please wait.

1
Sleep apnea and Cardiovascular diseases D. O. Rodenstein Service de pneumologie Cliniques universitaires Saint-Luc Université catholique de Louvain

3
Normal Sleep Effects Decreases in –Metabolic rate –Sympathetic nervous activity –Blood pressure –Heart Rate Increases in –Cardiac vagal tone

4
Diagnostic study

5
Obstructive events with thoraco-abdominal paradox

6
Epidemiology

9
There is a high prevalence of obstructive sleep apneas/hypopnea, in both men and women. Many subjects in the general population have more than 20 apneas/hypopneas per hour of sleep.

10
Accelération et descéleration cardiaques 55 82

11
Accelération et descéleration cardiaques 44 100

12
Possible mechanisms linking Sleep Apnea to Cardiovascular consequences Episodic Repetitive Hypercapnic Hypoxia Repetitive Reoxygenation Free Oxygen Radicals Repetitive arousals Sympathetic surges Inhibition of lung expansion Inhibition of parasympathetic tone

13
Possible mechanisms linking Sleep Apnea to Cardiovascular consequences Increase in Neural Sympathetic Traffic Peripheral vasoconstriction Increase negative intrathoracic pressure Increase left ventricular afterload Increased thoracic blood pooling and right ventricular preload Hypoxia related pulmonary vasoconstriction Increase in right ventricular afterload Paradoxical leftward shift of the interventricular septum Decrease in stroke volume

14
Intermittent hypoxia related to the production of –Oxygen-Free-Radicals –Tumor necrosis factor α –Interleukin 8 –Interleukin 6 –C Reactive Protein

15
Decrease endothelium dependent vasodilation Decrease endothelial nitric oxide (eNOS) Increased oxidated lipoproteins Increase in adhesion molecules Vascular smooth muscle proliferation Platelet aggregation and activation Increase in Fibrinogen and decrease in PAI1 (Plasminogen Activator Inhibitor type-1) activity
 Increased oxidated lipoproteins Increase in adhesion molecules Vascular smooth muscle proliferation Platelet aggregation and activation Increase in Fibrinogen and decrease in PAI1 (Plasminogen Activator Inhibitor type-1) activity")
16
Cardiovascular consequences of obstructive sleep apnea Clinical effects Hypertension Atherosclerosis Coronary artery disease Heart failure Arrhythmias Stroke Sudden death Glucose intolerance

17
Arrhythmias Arrhythmias in general seem not to be more prevalent in OSA, but recurrent atrial fibrillation is probably twice as frequent in OSA compared to non OSA patients

18
Atherosclerosis Increase markers of early atherosclerosis –Carotid Intima-Media Thickness –Decreased arterial compliance –Silent Brain Infarction –Decrease in cerebral blood flow during apneas

19
Atherosclerosis In animals, association of exposure to chronic intermittent hypoxia and a rich cholesterol diet lead to atherosclerosis, whereas neither of both alone does

20
Hypertension Epidemiological studies have shown that approximately 40% of patients with sleep apnea have hypertension, and that about 40% of patients with hypertension have sleep apnea. Actual figures vary, depending on the definitions and thresholds for sleep apnea and hypertension.

21
Sleep Apnea and Hypertension A Population-based Study| Khin Mae Hla; Terry B. Young; Tom Bidwell; Mari Palta; James B. Skatrud; and Jerome Dempsey Khin Mae Hla; Terry B. Young; Tom Bidwell; Mari Palta; James B. Skatrud; and Jerome Dempsey Ann Int Med 1994

24
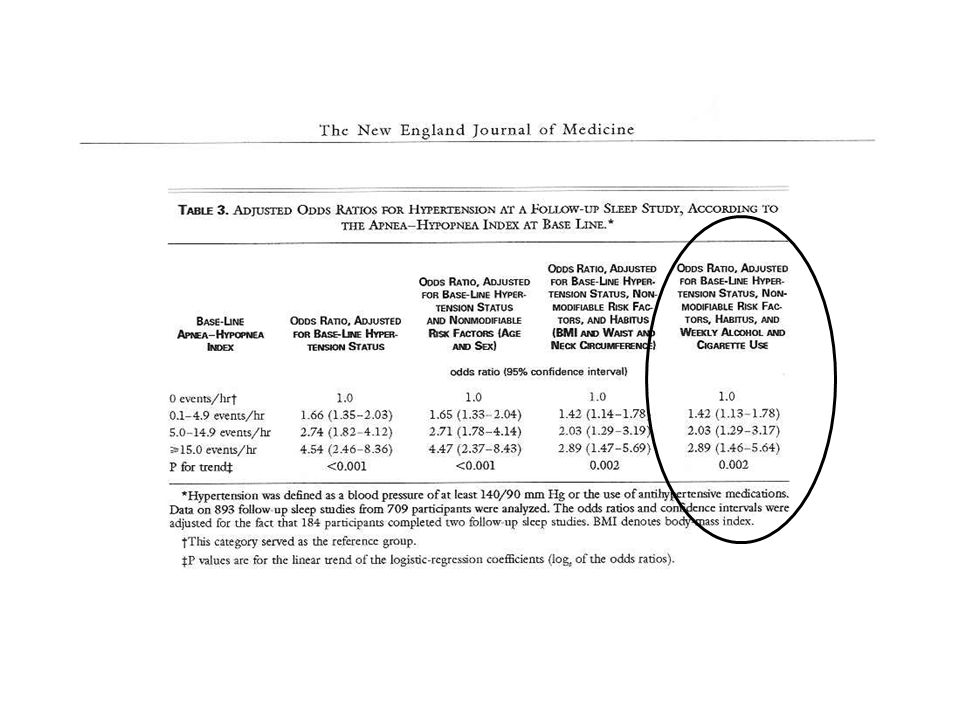
Confounders Hypertension, as sleep apnea, rarely comes alone. Therefore, before implying causality from association, possible confounders need to be considered. These include gender, age, alcohol consumption, smoking, obesity (in general, or in particuler as for instance neck circumference)
.")
25
Odds ratio for hypertension at 4 year follow-up according to baseline apnea-hypopnea index in 704 subjects from the Wisconsin Sleep Cohort. 184 subjects were followed-up for 8 years. Data were adjusted for baseline hypertension, body mass index, neck and waist circumference, age, gender, alcohol consumption and smoking habits.

27
Animal Models Intermittent sustained hypoxia Intermittent cyclic hypoxia Sleep-related obstructive apneas Sleep-related auditory arousals

31
A drop in mean blood pressure of 10 mmHg would reduce coronary heart disease risk by 37% and stroke risk by 56%. Subtherapeutic CPAP reduced AHÍ by 50% but did not influence blood pressure

33
Normotensive Hypertensive BP HR Na

34
11 consecutive patients with refractory hypertension (hypertension despite 3 different drugs at maximal dosing)
")
35
Treatment with CPAP lowers blood pressure in patients with OSA. This effect is modest but consistent, and is more evident in patient with more severe hypertension

36
In addition, CPAP increases Left Ventricular Ejection Fraction

37
Hypertension: Conclusions Sleep apnea is an independent cause of systemic hypertension, beyond the effects of obesity, gender, age etc Patients with sleep apnea have 30% to 300% more risk of hypertension Treatment of sleep apnea may contribute to the treatment or control of hypertension, decreasing mean blood pressure by about 10 mmHg

38
Mechanisms: hormones Hypertension 2004 ANP Renin Angiotensin Aldosterone Norepinephrine Epinephrin Cytokines

39
Mechanisms: “metabolism” Visceral fat Hyperleptinemia Insulin resistance Interleukin-6 Interleukin-1β Tumor necrosis factor-α

40
OSAS and cardiovascular disease

41
Compared with subjects with an AHI ~1, subjects with an AHI >11 have 22% more coronary heart disease, 220% more heart failure, and 55% more stroke, after adjusting for confounding variables.

42
Obstructive sleep apnea aggravates the clinical course of coronary artery disease, with higher mortality, more major cardiac events and more restenoses after percutaneous dilation

43
OSAS and Stroke

44
In cross-sectional studies, OSAS appears as a possible risk factor for stroke.

45
New Engl J Med 2005 Longitudinal study. Polysomnography at entry, events on follow-up

46
New Engl J Med 2005

47
$$$$ $$$$ $$$$

49
218 patients with sleep apnea and 218 normal subjects matched for age, gender, neighborhood and family physician were compared for health care costs for the 2 years prior to diagnosis. Patients mean annual individual costs (948 US$) were significantly higher than costs for controls (571 US$). Excess costs were due to more admissions, more consultations and more prescribed medications. The main prescribed pharmacological groups were cardiovascular and alimentary tract and metabolism. Chest 2005; 128: 1310-1314
 were significantly higher than costs for controls (571 US$). Excess costs were due to more admissions, more consultations and more prescribed medications. The main prescribed pharmacological groups were cardiovascular and alimentary tract and metabolism. Chest 2005; 128:")
50
OSAS and cardiovascular mortality

52
In this prospective study, severe OSAS increases the risk of fatal and non-fatal cardiovascular events in the 10 years following the initial diagnosis. Effective treatment with nCPAP in compliant patients eliminates this increased risk

53
4 years follow-up of patients with severe OSAS treated with nCPAP according to compliance to tretment: less than 1 hour per night (n= 85), 1 to 6 hours per night (n= 342) and >6 hours per night (n= 322).
, 1 to 6 hours per night (n= 342) and >6 hours per night (n= 322).")
54
Untreated (or very poorly treated) patients with severe OSAS have a reduced survival after 4 years follow-up, compared to similar patients moderately or very compliant to nCPAP therapy (85.5% vs 91.3% vs 96.4%). The main cause of death was cardiovascular. Compliance to nCPAP, hypertension, age and FEV 1 independently predicted survival.

55
Lancet 2009; 373: 82-93

56
Conclusions Obstructive sleep apnea is –A prevalent disease –Linked to obesity –Causally related to hypertension –Increasing risks for Heart failure Stroke Cardiovascular related mortality –Reversible under CPAP treatment

57
Conclusions Obstructive sleep apnea is NOT a cardiovascular disease It is a respiratory sleep-related disease The events that follow breathing cessation lead to cardiovascular consequences, among others, but the primary event is the sleep-related collapse of the pharynx in the face of persistent ineffective breathing efforts

58
Presenting Symptoms Related to sleep –Unrefreshing sleep –Unrestorative sleep –Disturbing snoring –Breathing pauses –Restless sleep –Nocturia –Nocturnal sweating –Gasping sounds –Wake-up suffocating

59
Presenting Symptoms Related to wakefulness –Tiredness –Lack of energy –Sleepiness –Memory impairment –Anxiety and Irritability –Depression –Lack (or loss) of interest –Sexual Dysfunction (Erectile Dysfunction, loss of sexual desire) –Headaches
 of interest –Sexual Dysfunction (Erectile Dysfunction, loss of sexual desire) –Headaches")
60
Conclusions Even if the patient is referred just for refractory hypertension, the treatment of obstructive sleep apnea will correct a large series of consequences: Neurologic Cognitive Behavioral Cardiovascular

61
Thank you

63
In the cross-sectional Sleep Heart Health Study, sleep apnea significantly increases the risk for coronary heart disease, heart failure, stroke, and combined cardiovascular disease, independently from confounding factors

64
Intervention studies

65
Significant decrease in nightime, but not daytime, blood pressure after 3 weeks nCPAP

66
Acute nocturnal effects of CPAP

67
Effects of 2 months nocturnal CPAP: decrease in nocturnal and diurnal blood pressure

69
Mechanisms: arousals Pepperell et Al, Sleep Med Rev 2002

70
Mechanisms: sympathetic stimulation

74
Cheyne Stokes

75
Cardiovascular consequences of obstructive sleep apnea Type of effects Hemodynamic Autonomic Chemical Inflammatory Metabolic

Similar presentations