Download presentation
Presentation is loading. Please wait.

1
Functional Neurosurgery and Anesthetic Considerations Susan M Ryan, PhD, MD Associate Clinical Professor Department of Anesthesia, UCSF 2006

2
What is Functional Neurosurgery? “Neurosurgery intended to improve or restore function by altering underlying physiology”

3
Areas of Functional Neurosurgery Movement disorders Seizures Pain syndromes Psychiatric disorders Peripheral nerve injuries

4
Areas of Expansion Movement disorders Seizures Psychiatric disorders

5
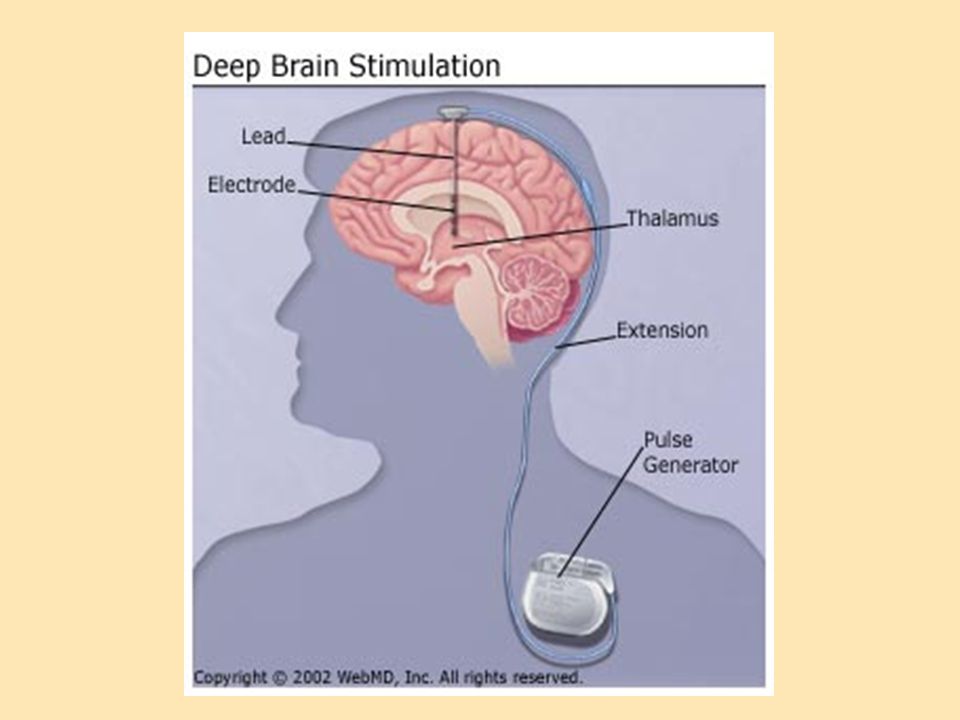
Neurosurgical Techniques Deep brain stimulation (DBS) Selective ablation electrodes Implantation viral vectors stem cells Cranial nerve/ peripheral electrical stimulation
 Selective ablation electrodes Implantation viral vectors stem cells Cranial nerve/ peripheral electrical stimulation")
6
Functional Neurosurgery Began in mid-1900’s Eclipsed by effective medications Now: Non-responders Advanced cases

7
Neurosurgical Techniques Deep brain stimulation Best established use: Parkinson’s Disease Vagal nerve stimulation Best established use: Seizure disorders

8
DBS/VNS Studies in Progress Obesity Fibromyalgia Cluster headache Tourette’s Syndrome Depression Obsessive Compulsive Disorder

9
DBS for Parkinson’s Disease

10
Clinical Features ‘Pill-rolling’ tremor Masked faces ‘Cog-wheel’ rigidity Festinating gate Bradykinesia

11
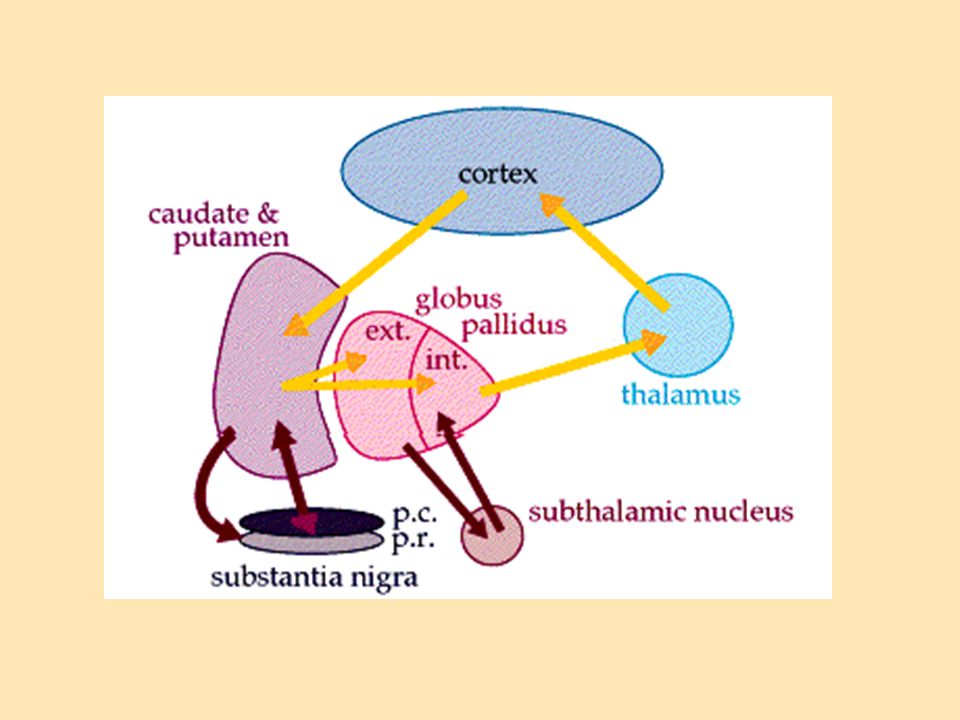
Pathologic Features Progressive neuronal death Dopamine neurons of substantia nigra Non- dopamine populations in CNS and PNS Bulbar function Sympathetic chain Parasympathetics of the gut

12
Basal Ganglia in PD

14
Treatment Medications L-dopa + periph. inhibitor (Sinamet) Dopamine agonists MAO inhibitors COMT inhibitors Amantadine
 Dopamine agonists MAO inhibitors COMT inhibitors Amantadine.")
15
DBS Surgery Goal: Improvement in PD symptoms Tremor Rigidity Hypokinesia Gait Balance

17
DBS Surgery Placement of stereotactic frame prior to procedure MRI to confirm coordinates

18
DBS Surgery Stereotactic head frame attached to bed Pt placed in sitting position

19
DBS Stereotactic Surgery Drill hole in skull to allow electrode placement for recording & stimulation

20
DBS Stereotactic Surgery Electrode passed slowly to record single cells in nucleus of interest

21
DBS Stereotactic Surgery Visual and auditory feedback of cell location and characteristics

22
DBS Stereotactic Surgery Listening for cell response during leg movement

23
DBS Surgery Find best location within the nucleus Place stimulating electrode Close burr hole, remove frame Induce general anesthesia Tunnel leads Place generator in upper chest wall Wait to activate stimulator in outpatient setting

24
Anesthesia: DBS Generator placement General anesthesia for generator placement No particular anesthetic Propofol or inhaled agent work well Avoid dopamine antagonists Avoid demerol Muscle relaxants OK Prevent or treat emergence hypertension Not much pain in post-op setting

25
PD: Specific Issues Risk of exacerbation Consider intraoperative continuation of medications Hemodynamics may be labile Degeneration of sympathetic ganglia Dopamine-related hypotension, hypovolemia

26
PD: Specific Issues Airway or pulmonary compromise Upper airway obstruction Dysarthria and history of choking Restrictive ventilatory pattern Aspiration risk

27
Patients with Existing DBS DBS is usually on 24/7 for PD pts May be off at night in other conditions Consider turning off prior to surgery

28
DBS: Surgical Risks Intracerebral hemorrhage Venous air embolism Emotional lability

29
DBS: Surgical Risks Intracerebral hemorrhage Monitor patient for neurologic changes Risk: 1.6% per lead Avoid hypertension Keep SBP < 140 Consider arterial line Antihypertensives: labetalol, hydralazine

30
DBS: Surgical Risks Venous air embolism Early detection Communicate with surgeon Support blood pressure Provide O2 Airway plan

31
DBS: Surgical Risks Emotional Lability Usually no treatment needed Consider sedation PRN

32
DBS Outcomes Bilateral DBS of STN: N = 49 Assessed at 1,3, and 5 years Assessed on and off meds and stimulation (Krack, et al, NEJM 349, 2003)
")
33
DBS Outcomes Stimulation alone: significant improvement Synergy between meds and stimulation Allows decrease in medication doses Improvement in L-dopa dyskinesias Akinesia, speech, and freezing of gait all worsened (Krack, et al, NEJM 349, 2003)
")
34
DBS vs Medical Therapy Randomized-pair trial: DBS + optimized medical tx Optimized medical tx 75% of pairs favored DBS + meds Quality of life Severity of motor sxs off medication (Deuschl et al, NEJM, 355, 2006)
")
35
DBS: other motor diseases Essential tremor Dystonia More sedation during MRI

36
DBS and Tourette’s Motor/speech tics Up to 1% school age children 1/3 persist into adulthood

37
DBS for Tourette’s (Visser-Vandewalle, J. Neurosurg 99: 2003)
")
38
DBS and Psychiatric Disease Depression Pilot in 2005 4/6 patients improved >50% on testing Currently at least 3 ongoing NIH trials 10 to 20 patients per study

39
Vagus Nerve Stimulation

40
Vagus: Mixed Sensory and Motor 20% efferent: parasympathetic control of the heart and gut viscera 80% afferent: extensive connections to limbic and higher cortical systems Animal studies VNS: EEG changes and seizure cessation

41
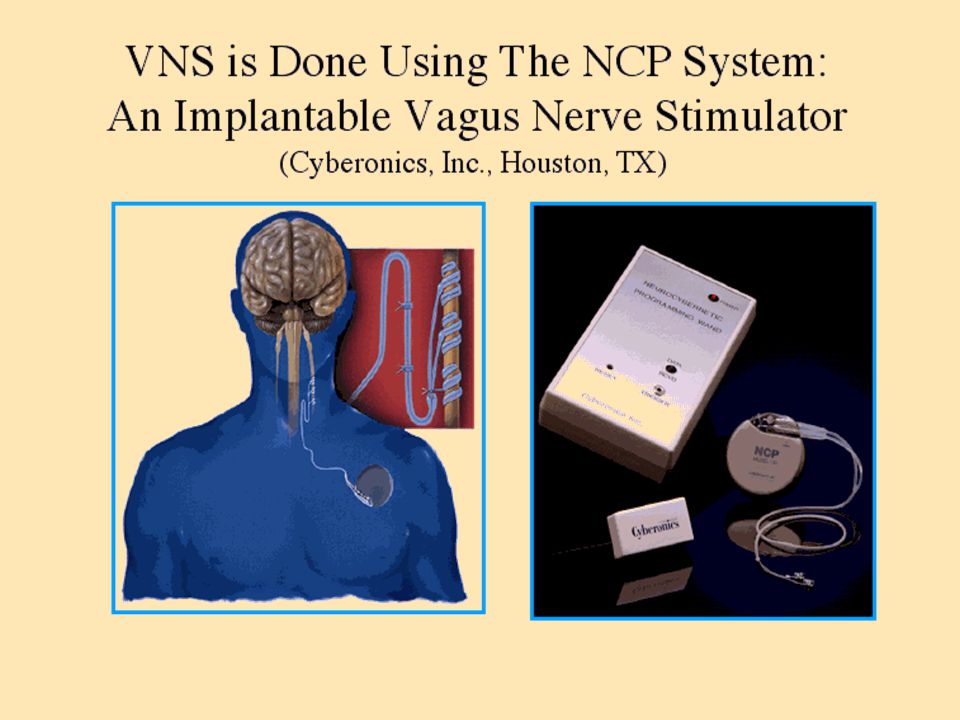
Vagal Nerve Stimulation Approved device made by Cyberonics Chronic, intermittent stimulation to cervical vagus Prevents and aborts seizures

43
Vagal Nerve Stimulation Typical settings: Automatic: 30 sec stimulation q 5 min Additional manual: if pt feels aura, may wave wand over generator to activate stimulator

44
Vagal Nerve Stimulation Results from 3 studies: Significant decrease in seizures: 24%-35% Controls: low-level stimulation Seizure frequency decreased further over time Decreased medication doses

45
VNS Surgery Performed under general anesthesia Leads wrapped around L vagus in neck Only L, and only unilateral Generator placed upper left chest

46
Final Electrode/tether Placement Negative Electrode Positive Electrode Anchor Tether

47
VNS Surgery Possible intraop complications with lead testing: Arrhythmias- transient sinus arrest Labile hemodynamics Airway obstruction (vocal cord stimulation)- if not intubated
- if not intubated")
48
VNS Surgery Surgical complications: Infection: 2.9% Hoarseness or temporary vocal cord paralysis: 0.7% Hypesthesia or lower left facial paralysis: 0.7%

49
VNS Surgery: Chronic Side Effects Hoarseness Cough Paresthesias Dyspepsia Disrupted sleep Worsening sleep apnea

50
VNS: Anesthesia Pre-op considerations: Take usual seizure medications CBC, electrolytes EKG cardiac medications?

51
VNS: Anesthesia May use local, MAC, or GA Usually GA- no restriction on agents Endotracheal tube Blood loss is minimal

52
VNS: Anesthesia Anti-seizure medications induce hepatic enzymes-- higher anesthetic doses? Post-op seizures are common- be prepared Incidence of transient vocal cord paralysis

53
Chronic VNS Turn off for other surgery Restart in recovery

54
VNS for Depression Seizure pts with VNS: happier over time! N = 60 pts previously failed numerous treatments 2 weeks on meds only 2 weeks stim adjust + meds 8 weeks fixed stimu + meds

55
VNS for Depression Open label study: 30.5% of patients responded with significant decrease in depression rating scale 15% full remission Substantial functional improvement, even in non-responders

56
VNS for Depression Placebo controlled study: N= 225 VNS-responding patients: 15% Placebo-responding patients: 10% Lower levels of stimulation Much to figure out, although now FDA approved

57
Other ongoing VNS studies Cervical VNS: PTSD Panic disorder OCD Rapid-cycling bipolar disorder Bilateral diaphragmatic VNS Morbid obesity

58
Functional Neurosurgery DBS Targets stimulation based on neuroanatomy. Tailors stim to the disorder. Invasive. Requires neurosurgery VNS Simultaneous stimulation of multiple tracts & nuclei. No specific target. Same stimulation for a number of disorders. Much less invasive. Does not require neurosurgeon. Procedure in search of an application?

Similar presentations




>")









>")




