Download presentation
Presentation is loading. Please wait.

1
Evaluation of Vertigo Dr. Vishal Sharma

2
Definition of vertigo A sensation of rotation or imbalance of one's self or of one's surroundings in any plane rotation of one's self = subjective vertigo rotation of one's surroundings = objective vertigo

4
Causes for vertigo A. Peripheral: lesions of vestibular end organs & vestibular nerve. Account for 85% of all cases of vertigo. B. Central: lesions of central nervous system. Account for 15% of all cases.

5
Central causes for vertigo
Vascular causes: see next slide Epilepsy: both disease & its treatment Road Traffic Accident: Head trauma Tumor: of brainstem, 4th ventricle & cerebellum Infection: Meningitis, Encephalitis Glial diseases: Multiple sclerosis Others: Parkinsonism, Psychogenic

6
Vascular Causes 2. Wallenberg’s lateral medullary syndrome: PICA
1. Vertebro-Basilar Insufficiency 2. Wallenberg’s lateral medullary syndrome: PICA Ipsilateral ataxia + vertigo + nystagmus + diplopia loss of touch, pain & temperature: I/L face, C/L body Dysphagia, hoarseness, decreased gag reflex I/L Horner’s syndrome 3. Hypertension Basilar migraine

7
Peripheral causes B.P.P.V. (commonest) Temporal bone #
Meniere’s disease Barotrauma Vestibular neuronitis Cholesteatoma Labyrinthitis Cochlear otosclerosis Vestibulotoxic drugs Autoimmune disease Vestibular schwannoma Presbystasis Perilymph fistula Paget’s disease

8
Miscellaneous causes Iatrogenic Surgical Cholesteatoma Stapedectomy Drug induced Ototoxic drugs Cervical Vertigo Neurovascular Neuromuscular Mechanical vascular Ocular Vertigo Error of refraction Extra-ocular muscle palsy

9
Psychogenic vertigo Causes: anxiety, panic disorder, phobia
Diagnostic features: Absence of organic causes Presence of vague & fleeting symptoms Dramatic presentation & attention seeking behaviour Relation b/w emotional stress & onset of vertigo

10
Vertigo-like symptoms
Faintness light-headedness unsteadiness motion intolerance imbalance floating sensation

11
Causes of Vertigo-like symptoms

12
Hematological: anemia, polycythemia
Cardiovascular Metabolic Orthostatic hypotension Diabetes mellitus Cardiac failure Hypoglycemia Obstructive cardiomyopathy Hypothyroidism Cardiac dysrhythmias Chronic renal failure Carotid sinus syndrome Alcohol intoxication Hyperventilation

13
History Taking Can diagnose 80% cases

14
Important history questions
Confirmation of vertigo: rotatory sensation Absence of syncope or light headedness Onset: sudden or gradual Episodic (isolated / recurrent) or continuous Duration of each episode of vertigo Associated symptoms Provoking or aggravating factors Systemic illness for vertigo
 or continuous. Duration of each episode of vertigo. Associated symptoms. Provoking or aggravating factors. Systemic illness for vertigo.")
15
Associated symptoms Decreased hearing: symmetric or asymmetric
Ear discharge Tinnitus Aural fullness Nausea & vomiting Imbalance

16
Associated symptoms Causes
Deafness + tinnitus + aural fullness Meniere’s disease Imbalance Vestibular neuronitis, Acoustic neuroma Headache Migraine, Acoustic neuroma Focal neurological findings Acoustic neuroma, Central vascular causes Ear discharge Labyrinthitis, perilymph fistula

17
Provoking or aggravating factors

18
1. Specific head position
2. Sudden standing up from sitting position 3. Sudden head & neck movement 4. Recent U.R.T.I. 5. Trauma to ear or head 6. Stress 7. Change in ear pressure 8. Headache 9. Drug intake 10. Diplopia

19
Provoking factor Causes
Change in head position B.P.P.V., labyrinthitis, multiple sclerosis Sudden standing up from sitting position Orthostatic hypotension Sudden neck movement Cervical spondylosis, VBI Recent URTI Vestibular neuronitis Stress Psychogenic, migraine Change in ear pressure Perilymph fistula

20
Drugs causing vertigo Alcohol Analgesic (opiate)
Anti-histamine Anti-hypertensive Anti-angina drug Anti-arrhythmic Anti-coagulant Aminoglycoside Isoniazide (INH) Rifampicin Anti-malarial Corticosteroid
 Rifampicin. Anti-malarial Corticosteroid.")
21
Systemic illness for vertigo
Hypertension / Hypotension Hypoglycemia Epilepsy Brain infection Brain tumors Parkinsonism Multiple sclerosis

22
Duration of one episode
Causes Few minutes B.P.P.V., Perilymph fistula Up to 1 hr Central vascular causes, Perilymph fistula Hours Meniere’s disease, Acoustic neuroma, Perilymph fistula, Central vascular causes, Head trauma Days Vestibular neuronitis, Multiple sclerosis, Perilymph fistula, Central vascular causes Weeks Psychogenic

25
Routine ENT OPD tests for vertigo evaluation

26
Test for spontaneous & gaze-evoked nystagmus
Head shake test Positional tests Positioning tests (Dix-Hallpike & Roll tests) Fistula test Caloric tests Tests for dysequilibrium Tests for coordination Cranial nerve examination
 Fistula test. Caloric tests. Tests for dysequilibrium. Tests for coordination. Cranial nerve examination.")
27
Nystagmus Involuntary, rhythmical oscillatory movement of eye
Vestibular disorders cause jerk nystagmus with slow & fast phases Direction of nystagmus given by its fast phase Vestibular nystagmus gets enhanced by looking in direction of faster phase & diminished by looking away from it (Alexander’s law)
")
28
Alexander’s Classification
Intensity grading of vestibular nystagmus: 1° only present while looking towards fast phase 2° present while looking towards fast phase & also while looking straight 3° present while looking towards fast phase, looking straight & looking towards slow phase

29
Nystagmus Vestibular lesion nystagmus gets suppressed by optic fixation & gets enhanced with removal of optic fixation (with Frenzel glasses or in dark) Irritative vestibular labyrinthine lesion: Ipsilateral nystagmus Paralytic vestibular labyrinthine lesion: Contralateral nystagmus
 Irritative vestibular labyrinthine lesion: Ipsilateral nystagmus. Paralytic vestibular labyrinthine lesion: Contralateral nystagmus.")
30
Features Peripheral Central
1. Nystagmus character a. Direction Fixed Changes b. Duration Short (days) Long (weeks) c. Effect of optic fixation Inhibited Unchanged d. Latency Present Absent 2. Imbalance Mild Severe 3. Nausea & vomiting Variable 4. Deafness & tinnitus Common Rare 5. Neurological deficit
 Long (weeks) c. Effect of optic fixation. Inhibited. Unchanged. d. Latency. Present. Absent. 2. Imbalance. Mild. Severe. 3. Nausea & vomiting. Variable. 4. Deafness & tinnitus. Common. Rare. 5. Neurological deficit.")
31
Nystagmus (slow component)
")
32
Nystagmus (fast component)
")
33
Semicircular canal stimulated Nystagmus Direction (fast phase)
Right Lateral Right horizontal Left Lateral Left horizontal Right Superior Down beating, counter-clockwise Left Superior Down beating, clockwise Right Posterior Up beating, counter-clockwise Left Posterior Up beating, clockwise

34
Other eyeball movements
Opsoclonus: non-rhythmic, bizarre eye movements Seen in brain stem & cerebellar pathology. Ocular Flutter: mild form of opsoclonus lasting for few seconds Ocular Myoclonus: pendular movement of eyeball with rhythmic movement of soft palate & tongue Ocular Bobbing: irregular, abrupt downward jerks seen in CNS lesions

35
Test for spontaneous nystagmus
Patient’s eyes examined with: pt’s looking straight ahead with fixed head; no visual or vestibular stimulus; no optic fixation Best examined in dark room with infra-red video goggles over open eyes or during electro-nystagmography with eyes closed Spontaneous nystagmus seen in unilateral peripheral vestibular lesion

36
Infra-red video goggles

37
Test for gaze-evoked nystagmus

38
Test for gaze-evoked nystagmus
Finger kept centrally 30 cm from pt's eyes & moved in horizontal & vertical planes Pt is asked to follow it with his / her eyes Keep displacement from midline to maximum of 30° (avoids physiological end-point nystagmus) Bidirectional vertigo seen in CNS lesions
 Bidirectional vertigo seen in CNS lesions.")
39
Head Shake Test Patient’s head grasped by physician & rapidly shaken from side to side for 20 times. Repeat in vertical plane for 20 times. Presence of horizontal nystagmus indicates peripheral vestibular disorder. Lt lesion Rt nystagmus. Vertical nystagmus indicates brainstem or cerebellar lesion.

40
Head Shake Test Starting from neutral position (A), rapid head thrust to Rt in horizontal plane compensatory eye movement to left pt's eyes remain stable on examiner (B) On similar head movement to left (C), I/L hypoactive labyrinth results in delayed catch up saccade (D) to maintain gaze. Arrow shows direction of saccade
, rapid head thrust to Rt in horizontal plane compensatory eye movement to left pt s eyes remain stable on examiner (B) On similar head movement to left (C), I/L hypoactive labyrinth results in delayed catch up saccade (D) to maintain gaze. Arrow shows direction of saccade.")
41
Positional Nystagmus Placing pt’s head slowly in different positions, detects response to changes in direction of gravitational force 11 specific head position: a. Sitting position: 5 head positions b. Supine position: 6 head positions Each position to be maintained for 30 sec

42
Head positions Sitting position Supine position Head upright
Right side down Left side down Head extended Head flexed Supine position Head straight Right side down Left side down Head hanging Head hanging with right turn Head hanging with left turn

43
Positioning Nystagmus
Helps to detect anomalies in otolith system Provoked by placing head rapidly in different positions Tests Dix-Hallpike Test Roll Test

44
Fistula test Transmission of increased air pressure in E.A.C., via middle ear, into inner ear through a labyrinthine fistula causes vertigo + nystagmus towards affected ear E.A.C. pressure is increased by intermittent tragal pressure or Siegelization

45
Fistula Test

46
Sites of labyrinthine fistula
1. Horizontal semicircular canal Cholesteatoma destruction Fenestration operation 2. Oval window Post-stapedectomy 3. Round window membrane rupture

47
Hennebert’s sign False positive fistula sign in absence of labyrinthine fistula. Seen in: 1. Meniere's disease: fibrosis b/w stapes footplate & utricle 2. Hyper mobile stapes footplate Congenital syphilis Idiopathic

48
False negative fistula sign
Negative fistula sign in presence of labyrinthine fistula. Seen in: 1. Cholesteatoma matrix / granulation covering labyrinthine fistula 2. Dead Labyrinth 3. Total E.A.C. obstruction (impacted wax)
")
49
Dix – Hallpike maneuver (Nylen – Barany maneuver)
")
50
Step 1

51
Step 2

52
Step 3

53
Step 4

54
Steps 1 to 3

55
Step 3 to 4

56
Dix-Hallpike Manoeuvre
1. Pt in sitting position on a couch looking ahead 2. Pt’s head turned 45° towards diseased ear 3. Pt moved rapidly into supine position with head hanging 30° below couch. Pt’s eyes observed for nystagmus for 1 minute 4. Pt moved rapidly back into sitting position 5. Manoeuvre repeated for opposite ear

57
Frenzel glasses

58
Roll Test for lateral canal BPPV

59
1 2 3 4 5

60
Roll test for lateral canal BPPV
1. Patient lies supine with nose pointing up 2. Head turned 900 right rapidly & kept for 30 sec 3. Head turned back to supine position for 30 sec 4. Head turned 900 left rapidly & kept for 30 sec 5. Head turned back to supine position for 30 sec Watch for nystagmus after each step

61
Caloric testing

62
Methods of caloric tests

63
Fitzgerald-Hallpike Bithermal Caloric Test
Contraindications: 1. E.A.C. obstruction 2. Ear infection 3. T.M. perforation 4. Bradyarrythmias 5. Labyrinthine sedatives (for 24 hrs)
")
64
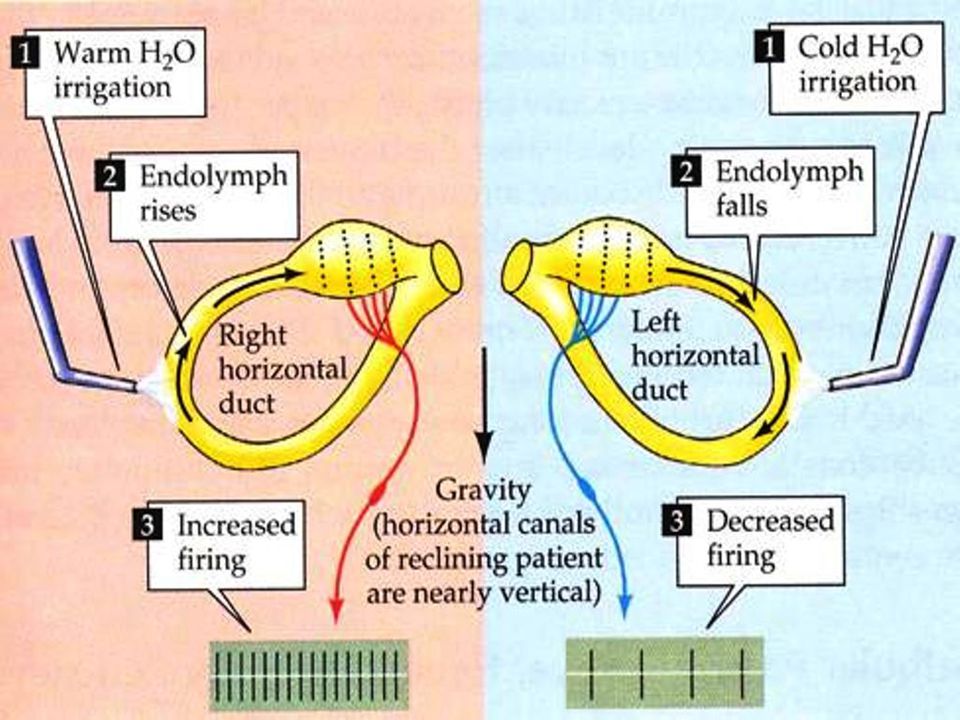
Mechanism of caloric stimulation

65
Convection current formation in endolymph due to temperature gradient → ampullo-petal flow for warm water activation of Vestibulo-Ocular Reflex OR ampullo-fugal flow for cold water inhibition of Vestibulo-Ocular Reflex vertigo + horizontal nystagmus (slow phase away from side of VOR activation & toward side of VOR inhibition)
")
66
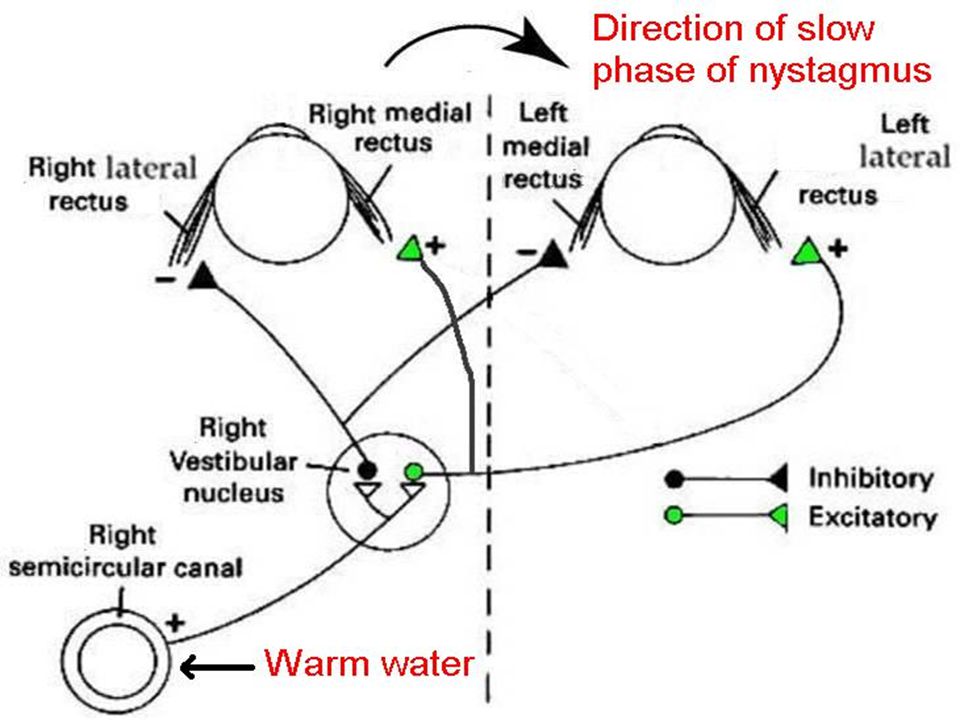
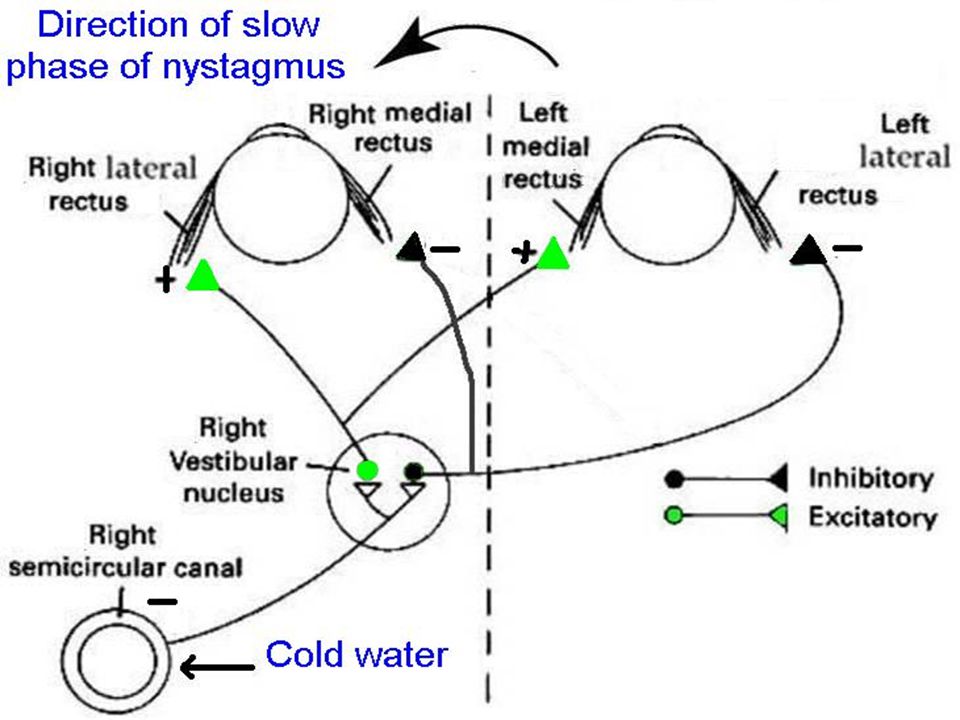
Anatomy of vestibulo-ocular reflex

70
Fitzgerald-Hallpike Bithermal Caloric Test
Pt supine + 30° head elevation. Each ear irrigated in turn for 40 sec with warm water at 44°C & then cold water at 30°C. Duration of nystagmus is from start of irrigation to end point of nystagmus. Normal = 90–140 sec Direction of fast component: Cold → Opposite ear; Warm → Same ear

71
Fitzgerald-Hallpike Bithermal Caloric Test

72
Fitzgerald-Hallpike Bithermal Caloric Test

73
Normal Calorigram

74
Canal Paresis Duration of nystagmus with both 44°C &
30°C irrigations in one ear is 30 % less than opposite ear. Seen in same sided peripheral vestibular lesion. C. P. (%) = (R30 + R44) – (L30 + L44) X 100 R30 + R44 + L30 + L44
 = (R30 + R44) – (L30 + L44) X 100. R30 + R44 + L30 + L44.")
75
Right Canal Paresis

76
Left Canal Paresis

77
Directional Preponderance
Duration of nystagmus in one direction is 30 % more than opposite direction. Seen in same sided central vestibular lesion & opposite peripheral vestibular lesion. D.P. (%) = (L30 + R44) – (R30 + L44) X 100 R30 + R44 + L30 + L44
 = (L30 + R44) – (R30 + L44) X 100. R30 + R44 + L30 + L44.")
78
Right Directional Preponderance

79
Left Directional Preponderance

80
Special cases Same sided canal paresis + same sided directional preponderance: Acoustic Neuroma Same sided canal paresis + opposite sided directional preponderance: Meniere’s disease

81
Left C.P. + Left D.P.

82
Left C.P. + Right D.P.

83
Caloric test in comatose patient
With brainstem intact: Only slow phase movements to cool or warm irrigation. Fast corrective phase absent. With B/L MLF damage (internuclear ophthalmoplegia) in Multiple Sclerosis: only lateral movement of one eye possible as B/L medial rectus muscles are denervated With B/L low brainstem lesion at vestibular nuclei: no nystagmus in either warm or cool water irrigation
 in Multiple Sclerosis: only lateral movement of one eye possible as B/L medial rectus muscles are denervated. With B/L low brainstem lesion at vestibular nuclei: no nystagmus in either warm or cool water irrigation.")
86
Modified Kobrak's Test E.A.C. irrigated for 60 sec with ice cold water in increasing quantity (5, 10, 20 & 40 ml) till nystagmus is noticed If nystagmus noticed with: 5 ml = Normal vestibular labyrinth 10 / 20 / 40 ml = Hypoactive labyrinth No nystagmus (40 ml) = Dead labyrinth
 = Dead labyrinth.")
87
Dundas Grant Cold Air Caloric Test
Done in T.M. perforation as water syringing is contraindicated Air in coiled copper tube is cooled by pouring ethyl chloride in it Effluent cool air is blown into E.A.C. to produce vertigo + nystagmus

88
Tests for dys-equilibrium
Standing test Tandem gait test Romberg test Modified Romberg test Unterberger / Fukuda stepping test Babinski Weill test

89
Standing Test Patient stands normally, with eyes closed
In peripheral vestibular lesion, pt assumes Discus Thrower’s position: Head turned towards side of lesion Trunk twisted to side of lesion Raising of hand on healthy side & lowering on side of lesion Falling to side of lesion

90
Discus thrower position

91
Tandem gait test Patient made to walk with eyes open in a straight line in tandem position (toes of one feet right behind heel of other feet). Stopped suddenly & asked to walk back. Test repeated with eyes closed Falling towards side of peripheral vestibular lesion
. Stopped suddenly & asked to walk back. Test repeated with eyes closed. Falling towards side of peripheral vestibular lesion.")
92
Tandem gait test

93
Romberg test

94
Subject stands with feet together, eyes open & hands by the sides for 1 minute. Observe for swaying.
Subject closes eyes in same position for 1 minute. Observe for swaying. Romberg test sharpened by tandem position of feet. Positive Romberg = swaying towards side of lesion, only when eyes are closed. Seen in sensory ataxia (loss of proprioception). Negative Romberg = swaying even when eyes are open. Seen in cerebellar ataxia.
. Negative Romberg = swaying even when eyes are open. Seen in cerebellar ataxia.")
95
Unterberger test Patient blindfolded, arms extended
Asked to step on same spot 90 times in 1 minute Peripheral vestibular lesion: pt deviates / rotates to side of lesion by > 30 degrees Deviation if <30 degrees on either side is considered normal

96
Babinski Weill test Patient asked to walk with eyes closed 5 pace forwards & 5 pace backwards 6 times in 30 sec U/L vestibular lesion: patient walks in star shaped trajectory

97
Tests for coordination
Past pointing Fukuda writing test Tests for cerebellar function Finger nose test Heel knee test Rapid alternating task test

98
Past pointing test Pt. made to sit with hands up & index finger extended Examiner raises his index finger in front of pt Pt asked to touch examiners finger with eyes open & then with eyes closed If pt cannot perform task smoothly past pointing

99
Fukuda writing test Patient asked 8-10 capital letter vertically in a straight line first with eyes open then with eyes closed In U/L vestibular lesion: Letter deviates >20 deg towards involved side but are legible In cerebellar lesion: Letters are illegible

100
Finger nose test Pt asked to touch her nose & then touch examiner’s index finger with her index finger. Cerebellar lesion pt cannot do it.

101
Rapid alternating task test
Heel shin test Pt asked to move heel of one leg over shin of other leg in a straight line. Cerebellar lesion pt cannot do it. Rapid alternating task test Patient asked to alternately perform supination & pronation of one palm over other palm at rapid rate. Cerebellar lesion pt cannot do it (adiadochokinesia) or has difficulty doing it (dysdiadochokinesia).
 or has difficulty doing it (dysdiadochokinesia).")
102
Heel shin test

103
Rapid alternating task test

104
Cranial nerve examination
I = Smell test II = Snellen chart III / IV / VI = Ocular movement V = Corneal Reflex , Facial sensation VII = Facial muscle movement VIII = Tuning fork test IX / X = Palatal movement & gag reflex XI = Shrugging of shoulder & neck rotation XII = Tongue movement

105
Olfactory

106
Optic

107
Lt oculomotor nerve palsy

108
Lt trochlear nerve palsy
Primary position showing left superior oblique palsy with lack of its depressor effect

109
Lt abducens nerve palsy
Lack of abduction of left eye

110
Trigeminal

111
Trigeminal + Facial

112
Auditory

113
Glossopharyngeal & Vagus

114
Spinal Accessory

115
Hypoglossal

116
Other Specific Investigations

117
Electro-nystagmography
Computerized dynamic posturography Cranio-corpography Galvanic test Vestibular rotation tests Vestibular evoked potential Brain Electrical Activity Mapping (BEAM) Dynamic visual acuity
 Dynamic visual acuity.")
118
Electro-nystagmography

119
Principle Retina is negative charged compared to positive cornea resulting in corneo-retinal potential Movement of eyeball causes movement of electrical field currents & detected by electrodes around eye

120
Electrode positioning
Lateral to outer canthus both sides: horizontal movement Above & below eye one side: vertical movement Glabella: ground electrode

121
Electrode placement

122
Electro-nystagmograph
Y axis: 1 cm = 20 degree ocular movement X axis: 1 cm = 1 sec

123
Identification of movement
Horizontal movement of eye: Right movement = upward deflection Left movement = downward deflection Vertical movement of eye: Upward movement = upward deflection Downward movement = downward deflection

124
Nystagmus Identification
Nystagmus beat should be triangular in shape Upward & downward deflection should have different slopes Gradual slope = slow component Steep slope = fast component Both slopes equal = perpendicular nystagmus

125
E.N.G. procedures Vestibular tests Oculomotor tests
Spontaneous nystagmus Pursuit test Gaze nystagmus Saccade test Positional nystagmus Optokinetic test Positioning nystagmus Fixation test Fistula test Bi-thermal caloric tests

126
Fixation: holds image of stationary object on fovea
Vergence: moves eyes in opposite directions to place images of single object on both foveas at one time Saccade: brings images of objects of interest onto fovea Optokinetic tracking: holds images steady on retina during sustained head rotation Smooth pursuit: holds image of moving target on fovea Vestibulo-ocular reflex: holds images steady on retina during brief head rotation Nystagmus (quick phase): resets eyes during prolonged rotation & directs gaze toward oncoming visual scene
: resets eyes during prolonged rotation & directs gaze toward oncoming visual scene.")
128
ENG smooth pursuit movement

129
Culmination Frequency
No. of nystagmus beats in 30 seconds of most prolific phase of nystagmus duration in ENG Caloric test values: Right warm = beats / second Right cold = beats / second Left warm = beats / second Left cold = beats / second

130
Response graded as: 0 = normal response 1 = hypoactive response 2 = hyperactive response Result given as code of 4 digits in order of: Right warm, Right cold, Left warm, Left cold Graphical presentation of this data called Claussen’s Butterfly chart

131
Claussen’s Butterfly chart

132
0000 = Normal 1111 = B/l vestibular lesion or brain stem lesion 2222 = B/L brain stem + cerebellar lesion 1100 = Rt canal paresis in Rt vestibular lesion 0011 = Lt canal paresis in Lt vestibular lesion 0110 = Lt brain stem lesion 1001 = Rt brain stem lesion 0220 = Lt directional preponderance 2002 = Rt directional preponderance 0022 = Lt nystagmus dysinhibition in Rt cerebellar lesion 2200 = Rt nystagmus dysinhibition in Lt cerebellar lesion

133
Findings in central disorder
Spontaneous or positional nystagmus with normal caloric results Direction-changing nystagmus Failure of nystagmus suppression by optic fixation Bilateral reduced or absent caloric responses without history of labyrinthine or middle ear disease Abnormal saccade or pursuit results Hyperactive caloric responses (cerebellar disease)
")
134
Findings in peripheral disorder
Unilateral caloric weakness Bilateral caloric weakness with history of labyrinthine disease or administration of ototoxic drugs Fatiguing positional nystagmus Nystagmus suppression by optic fixation Direction-fixed nystagmus

135
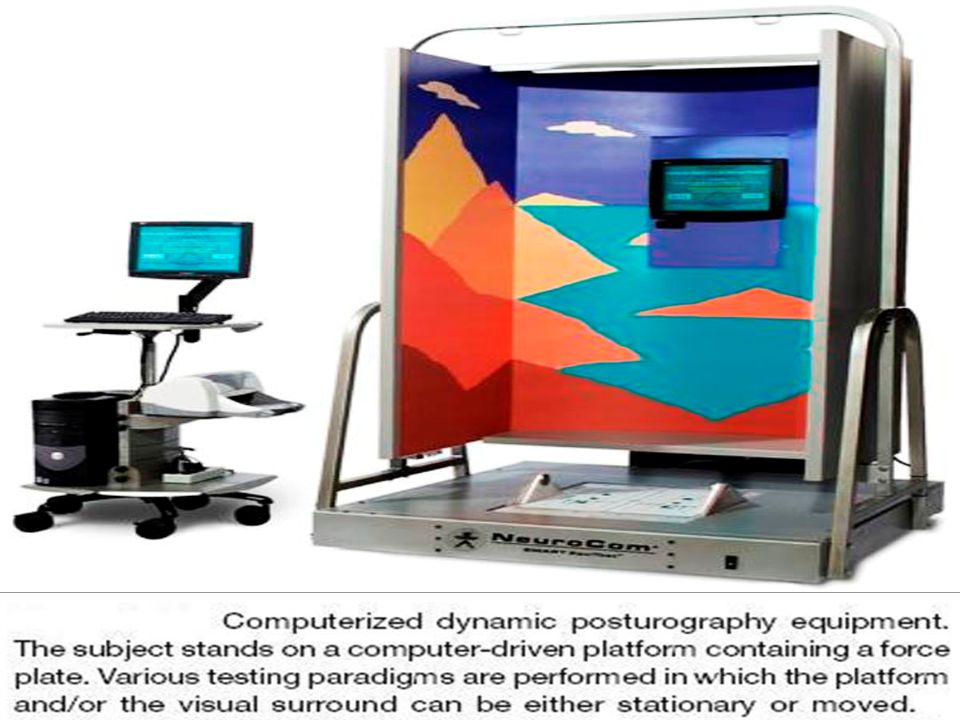
Computerized dynamic posturography
Consists of computer-controlled platform & visual booth used to evaluate both sensory + motor components of balance Has 2 parts: a. Sensory organization test b. Motor coordination / Motor control test Posturography not a substitute for careful gait examination & is more valuable in rehabilitation

137
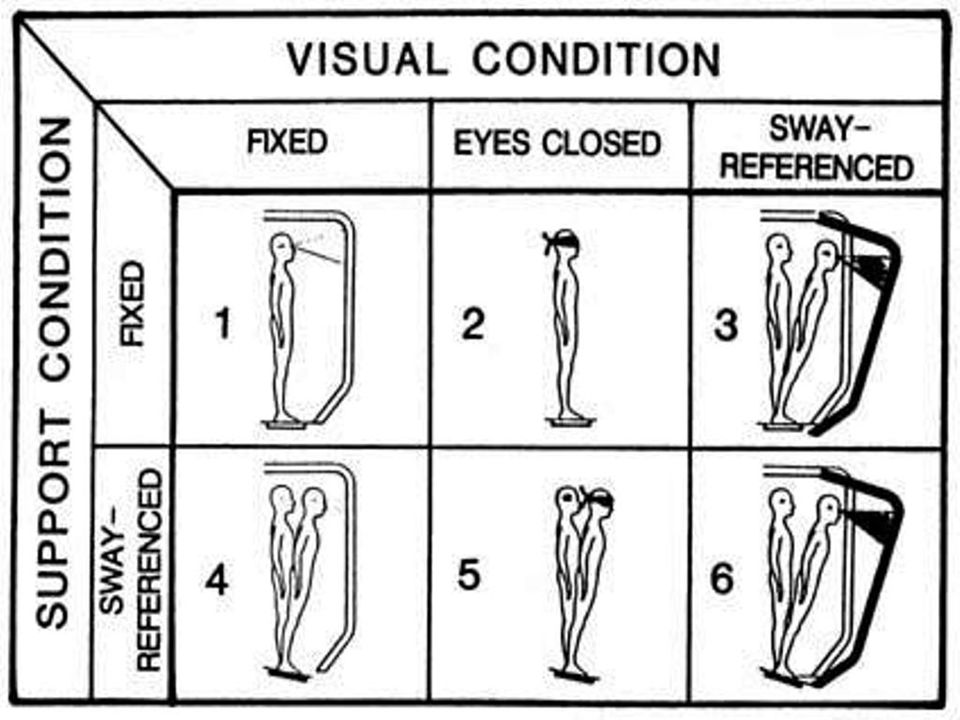
Sensory organization test
Detects defect in subject’s ability to use vestibular, somatosensory & visual inputs to maintain balance These 3 systems are singly or collectively manipulated to test subject’s ability to maintain balance under these stressful conditions. Analyzed by computer. Sensory test useful in peripheral lesions, vestibular rehabilitation & medico legal cases

139
Eye Visual Base Equilibrium Inputs
1 Open Steady Vestibular + Visual + Somatosensory 2 Close Absent Vestibular + Somatosensory 3 Sway Vestibular + Somatosensory + Visual (altered) 4 Vestibular + Visual + Somatosensory (altered) 5 Vestibular + Somatosensory (altered) 6 Vestibular + Visual (altered) + Somatosensory (altered)
 4. Vestibular + Visual + Somatosensory (altered) 5. Vestibular + Somatosensory (altered) 6. Vestibular + Visual (altered) + Somatosensory (altered)")
140
Dysfunction Pattern Abnormal Test Condition
Vestibular , 6 Visual + vestibular , 5, 6 Visual preference , 6 Visual preference + vestibular , 5, 6 Somatosensory + vestibular , 3, 5, 6 Severe dysfunction , 2, 3, 4

141
Motor coordination test
Evaluation of efferent motor pathway of balance Support surface of CDP machine suddenly moved: 1. forward & backward 2. upward & downward Lower limb muscle responds by movement of ankle & hip joints. Motor output assessed by CDP

142
Motor coordination test

143
Cranio-corpography Pt wears helmet with light bulbs
Photographic representation of pt's movement patterns on performing Romberg & Unterberger tests Wide angular deviation (> 700 away from sagittal axis) indicates peripheral dysfunction on side of deviation Lateral sway > 20 cm suggests central pathology
 indicates peripheral dysfunction on side of deviation. Lateral sway > 20 cm suggests central pathology.")
144
Cranio-corpography

145
Left angular deviation

146
Broad lateral sway

147
Galvanic test

148
Current of 1 mA passed through saline pad to 1 ear
Pt. stands with feet together, eyes closed, arms outstretched. Saline pads placed in EAC or over mastoid. Electrodes placed over sternum. Current of 1 mA passed through saline pad to 1 ear Normal person sways away from side of cathode (+ve) current & nystagmus (fast phase) towards cathode Current of >1mA required in vestibular neuronitis, long standing Meniere’s disease Response absent in vestibular schwannoma 148
 current & nystagmus (fast phase) towards cathode. Current of >1mA required in vestibular neuronitis, long standing Meniere’s disease. Response absent in vestibular schwannoma")
149
Vestibular rotation tests
Barany’s Chair Rotation Test Sinusoidal Acceleration Test Slow Harmonic Acceleration Test Vestibular Auto-rotation Test (VAT)
")
150
Barany’s chair rotation test Subject seated in dental chair pt’s head bent 300 forwards (lateral SSC lies in plain of rotation) chair rotated 10 times in 20 sec rotation stopped abruptly nystagmus direction + intensity noted both clockwise & anti-clockwise rotations done Sinusoidal acceleration test Pt placed in suspended torsion swing chair chair rotated to one side & let go spring action of bar helps in sinusoidal to & fro rotation in vertical axis
 chair rotated 10 times in 20 sec rotation stopped abruptly nystagmus direction + intensity noted both clockwise & anti-clockwise rotations done Sinusoidal acceleration test Pt placed in suspended torsion swing chair chair rotated to one side & let go spring action of bar helps in sinusoidal to & fro rotation in vertical axis")
151
Slow harmonic acceleration test
Sinusoidal rotation of chair controlled by computer & intensity of nystagmus calculated by computer Findings in rotation tests Rt rotation (clockwise) Rt beating nystagmus Lt rotation (anti-clockwise) Lt beating nystagmus Intensity of nystagmus same for both rotations Asymmetrical intensity vestibular pathology Intensity not ed on optic fixation central lesion 151
 Rt beating nystagmus. Lt rotation (anti-clockwise) Lt beating nystagmus. Intensity of nystagmus same for both rotations. Asymmetrical intensity vestibular pathology. Intensity not ed on optic fixation central lesion")
152
Gain = ratio of maximum eye velocity to maximum chair velocity
Depressed gain values usually seen in incorrect testing conditions Depressed gain values under good testing conditions suggest bilateral peripheral lesions Abnormally high gain can indicate presence of cerebellar lesion that is decreasing vestibular inhibition

153
Vestibular Autorotation Test
Head band worn by patient has microchip circuitry Pt asked to perform head movements in synchrony with computerized auditory clues Records horizontal & vertical eye movements with ENG electrodes Records horizontal & vertical head movements with microchip angular velocity sensors

154
Vestibular autorotation test

155
Vestibular evoked potentials
Vb.E.P study is like BERA with vestibular stimulus (head movement) instead of auditory stimulus Response recorded by electrode placed on pt’s vertex Short latency response: recorded from first 10 msec Middle latency response: 10 – 100 msec Long latency response: msec (also known as Long latency rotational evoked potential)
 instead of auditory stimulus. Response recorded by electrode placed on pt’s vertex. Short latency response: recorded from first 10 msec. Middle latency response: 10 – 100 msec. Long latency response: msec (also known as Long latency rotational evoked potential)")
156
Vestibular evoked potentials

157
Vestibular Evoked Myogenic Potentials (VEMP)
")
158
VEMP = Electromyography response of I/L sterno-cleidomastoid muscle to loud click. Afferent reflex limb from saccule via inferior vestibular nerve & efferent limb via medial vestibulo-spinal tract. Low audio thresholds (60 dB) for VEMP or Tullio effect seen in Meniere’s disease, superior SCC dehiscence, multiple sclerosis, acoustic neuromas & vestibular neuronitis. Normal threshold > 75 dB.
 for VEMP or Tullio effect seen in Meniere’s disease, superior SCC dehiscence, multiple sclerosis, acoustic neuromas & vestibular neuronitis. Normal threshold > 75 dB.")
159
VEMP with threshold of 85 dB

160
Brain Electrical Activity Mapping
Synonym: quantitative electro-encephalography Method of plotting brain electrical activity in response to auditory or vestibular stimuli at a given point of time Electrical activity measured by placing 20 electrodes on scalp, unlike Vb.E.P which places only 1 electrode

161
Interpretation of BEAM
Electrical activities from different part of scalp computed into topographical map for continuous plotting of electrical activity measurement In colour map: Red yellow green blue indicates transformation from positive voltage to negative voltage In black & white map: Black = +ve & grey = -ve

163
Dynamic Visual Acuity Movement of head causes significant retinal slip & loss of visual acuity unless vestibulo-ocular reflex produces compensatory response Rotational velocity sensors + computer screen evaluates vision during head movement providing functional assessment of vestibulo-ocular reflex Vestibular vertigo pt have greater reduction in dynamic visual acuity compared with non-vestibular vertigo

164
Referral to other departments
Internal Medicine: cardiovascular & metabolic causes Neurology: central nervous system causes Ophthalmology: ocular pathology Orthopedics: cervical spine problems Psychiatry: psychogenic vertigo Pediatric: in pediatric migraine Radiology: anatomic & physiologic brain imaging

165
Imaging indications in vertigo
Unilateral or asymmetric hearing loss Vertical nystagmus, nystagmus not suppressed with fixation, inability to stand unassisted Direction-changing spontaneous nystagmus Presence of cerebellar signs New-onset severe headache Stroke risk (DM, HTN, smoking, h/o myocardial infarct) Acute vertigo with neck pain
 Acute vertigo with neck pain.")
166
Plain X-ray indications:
Cervical spine problems C.T. scan brain indications: Ischemic strokes Cerebral & cerebellar hemorrhage M.R.I. brain indications: Cerebellar stroke Cerebello-pontine angle tumors Multiple sclerosis

167
Thank You

Similar presentations




















>")





