Download presentation
Presentation is loading. Please wait.

1
Acute Neurological Emergencies: Headache
1 1 1
2
Brad Bunney, MD Associate Professor Dept of Emergency Medicine
University of Illinois College of Medicine Chicago, IL

3
Michael Gerardi, MD, FAAP, FACEP Vice-Chairman, Department of Emergency Medicine Morristown Memorial Hospital Morristown, New Jersey Nina T. Gentile, MD Associate Professor Division of Emergency Medicine Temple University School of Medicine Philadelphia, PA Daniel G. Murphy, MD, FACEP Vice Chair & Medical Director Maimonides Medical Center Brooklyn, New York 1 1 1
4
The Case One hour prior to ED presentation, a 42 year old man was jogging and “hit” by the worst headache of his life. It was associated with some nausea and the feeling as if he was going to pass out. He rested for 30 minutes but the headache persisted as a diffuse, throbbing pain radiating to the base of his skull.

5
The Case (Continued) EMS was called. The patient felt as if he could not concentrate, there was no confusion, nor was there any other focal neurologic complaint. There was no past medical history, no medications, no family history, and no significant use of alcohol, tobacco or other drugs.

6
If a patient presented with the worst headache of his life, what is the work-up that should be initiated? a. Non-contrast CT b. LP after neg. CT c. LP without CT d. CT, LP, and angiography 6 5 6

7
Objectives What is the differential of a “thunderclap headache”?
What is the sensitivity of neuroimaging in subarachnoid hemorrhage (SAH)? What constitutes a “positive” lumbar puncture in SAH and when should it be performed? Do patients with suspected SAH who have a negative CT and lumbar puncture require additional imaging to “rule-out” expanded but unruptured aneurysm? 2 2 2
 What constitutes a positive lumbar puncture in SAH and when should it be performed Do patients with suspected SAH who have a negative CT and lumbar puncture require additional imaging to rule-out expanded but unruptured aneurysm")
8
Headache 1 of 10 top presenting complaints 1 to 2% of visits to ED
18 million outpatient visits 638 million days of work lost per year 78% of women and 64% of men had experienced at least one in the prior year 36% of women and 19% men suffer from recurrent headaches

9
Headache Most have primary headache disorders migraine tension
Only a few have treatable secondary causes that threaten life, limb, brain such as subarachnoid hemorrhage 1 - 4 % of headache visits

10
“Worst” Headache Normal exam: 12- 33% SAH Abnormal exam: 25% SAH
Initial hemorrhage may be fatal Early definitive surgery improves outcomes Patients with greatest likelihood of benefiting from surgery are most likely to receive incorrect diagnosis

11
Physicians Consistently Misdiagnose SAH
1. Failure to appreciate spectrum of clinical presentation 2. Failure to understand limitations of CT 3. Failure to perform and correctly interpret the results of LP

12
ED Goals in Headache Patients
1. Differentiate life-threatening from benign 2. Initiate prompt treatment 3. Provide prompt pain relief 4. Prevent drug seeking and refer 5. Minimize resource utilization in ED 6. Optimize patient use of ED 7. Increase pre-ED treatment and reduce ED use

13
Medical Conditions That Present With Headache
Pheochromocytoma Hyperthyroidism SLE Giant Cell Arteritis Fibromyalgia

14
Types of Headaches in the ED
Final Diagnosis Percentage Infection - not intracranial Tension HA Miscellaneous Post-traumatic Hypertension related Vascular (Migraine) No diagnosis SAH Meningitis
 4.5. No diagnosis 6.0. SAH 0.9. Meningitis 0.6.")
15
Causes of Headache That Require Specific Therapy
Subarachnoid hemorrhage Meningitis Encephalitis Cervicocranial-artery dissection Temporal arteritis Acute angle-closure glaucoma Hypertensive emergency

16
Causes of Headache That Require Specific Therapy
Carbon Monoxide poisoning Pseudotumor cerebri Cerebral venous and dural sinus thrombosis Acute stroke (hemorrhagic or ischemic) Mass Lesion tumor abscess intracranial hematoma parameningeal infection
 Mass Lesion. tumor. abscess intracranial. hematoma. parameningeal infection.")
17
Headache Danger Signals
Onset after 40 years new or different headache subacute HA that worsens exertion, sex, coughing, straining Worst ever experienced

18
Headache Danger Signals: Associated With Neurologic Change
Memory impairment Ataxia Drowsiness Sensory loss Signs of meningeal irritation

19
Headache Danger Signals: Associated With Neurologic Change
Progressive visual or neurologic change Confusion Weakness Loss of coordination Asymmetry of pupils, DTRs

20
Headache Danger Signals: Abnormal Medical Evaluation
Fever Chronic malaise Arthralgia HTN Myalgia Wt loss Tender, poorly pulsatile temporal arteries

21
Subarachnoid Hemorrhage
Incidence of 16 /100,000 about 33,600 cases per year 54% secondary to ruptured aneurysm Without treatment, 40% of aneurysm pts. have recurrent bleeding Aneurysm pt who survives initial rupture and is treated conservatively: 50% survival at one year

22
Time of Death Following SAH by Cause

23
Current Problems in Management of Subarachnoid Hemorrhage
Errors and delays in diagnosis Treatment of acute effects Prevention of recurrent hemorrhage Prevention or treatment of vasospasm or cerebral ischemia

24
Classic Symptoms of Subarachnoid Hemorrhage
Sudden, unusually severe or “thunderclap” headache Loss of consciousness Pain in neck, back, eye or face Nausea, vomiting, photophobia, phonophobia

25
Classic Signs of Subarachnoid Hemorrhage
Abnormal vital signs Respiratory changes, hypertension, cardiac arrhythmias Meningismus Focal neurologic signs may be present III nerve palsy – IC/PCA aneurysm Paraparesis – ACA aneurysm Hemiparesis, aphasia – MCA aneurysm Ocular hemorrhages

26
Subarachnoid Hemorrhage
Onset: Acute Location: Global Ass Sx: N,V, meningismus, focal Pain: Worst ever Duration: Brief Prior Hx: No Dx tests: CT 80-90% Phys ex: Focal signs, LOC, meningismus

27
Subarachnoid Hemorrhage
Warning leaks in 50% CT misses up to 10% small leaks Suspect if: > 35 years no previous HA no fading of HA came on with exertion altered LOC or neuro deficits stiff neck

28
Subarachnoid Hemorrhage: Neurologic Findings
Sudden HA without localizing findings Altered mentation Confusion, lethargy Bilateral extensor plantar reflex Unusual to find focal deficits

29
Causes of Non-Traumatic Subarachnoid Hemorrhage
“Berry” aneurysms AVM Cerebral angiomas Mycotic aneurysm Extension from parenchymatous hemorrhage Anticoagulation therapy

30
Causes of Non-Traumatic Subarachnoid Hemorrhage
Systemic bleeding diathesis Hemorrhagic encephalitis Hemorrhagic cerebral vasculitis Hemorrhage into CNS tumors or metastases Unknown

31
Warning Headache unusually severe distinct “Thunderclap” headache
% patients with SAH have HA days or weeks before index episode unusually severe distinct “Thunderclap” headache Day and Raskin 1996 intense, acute, peak intensity at onset develop in seconds maximal intensity in minutes lasts hours to days

32
“Thunderclap” Headache
25% associated with SAH “Warning” headache followed by SAH in 5% to 60% Expansion or dissection of unruptured aneurysm Cerebral venous thrombosis Exertional / coital headache

33
Misdiagnosis of SAH 217 patients from 4 institutions
54 (25%) were initially misdiagnosed 121 patients initially presented in good clinical condition 46 (38%) were initially misdiagnosed Stroke 1996;27:
 were initially misdiagnosed. 121 patients initially presented in good clinical condition. 46 (38%) were initially misdiagnosed. Stroke 1996;27:")
34
Misdiagnosis of SAH Outcome of Patients with Good Initial Presentation in Misdiagnosed and Correctly Diagnosed Patients With SAH Outcome Misdiagnosis (n=45) Correct Diagnosis (n=75) Excellent/good (53)* 68 (91)* Fair (11) ( 5) Poor/vegetative/dead 16 (36)* ( 4)* Values are number (%) in each clinical grade category. P<.001 Stroke 1996;27:
 Correct Diagnosis (n=75) Excellent/good 24 (53)* 68 (91)* Fair 5 (11) 4 ( 5) Poor/vegetative/dead 16 (36)* 3 ( 4)* Values are number (%) in each clinical grade category. P<.001. Stroke 1996;27:")
35
Misdiagnosis of SAH Rebleeds and Deteriorations Before Treatment in Misdiagnosed and Correctly Diagnosed Patients With SAH Misdiagnosis (n=54) Correct Diagnosis (n=163) Rebleeds 21* 4 Deteriorations Total *12/21 of misdiagnosed and 3/4 of correctly diagnosed patients rebled within 5 days of presentation. Stroke 1996;27:
 Correct Diagnosis (n=163) Rebleeds 21* 4. Deteriorations 5 0. Total *12/21 of misdiagnosed and 3/4 of correctly diagnosed patients rebled within 5 days of presentation. Stroke 1996;27:")
36
SAH…But not “Classic” Roughly half have minor bleeding with atypical features Nonstrenuous activities (34%) Sleep (12%) HA in any location (localized, generalized, mild) May be relieved by non-narcotic analgesics Diagnosed as migraine, tension-type, sinusitis
 HA in any location (localized, generalized, mild) May be relieved by non-narcotic analgesics. Diagnosed as migraine, tension-type, sinusitis.")
37
SAH: Most patients have...
Abrupt onset of severe, unique headache, or neck pain Abnormal findings on neurologic examination Subtle meningismus or ocular findings

38
International Headache Society
A first episode of severe headache cannot be classified as migraine: more than 4 episodes nor as tension-type headache: more than 9 episodes First or worst headache requires evaluation as do qualitatively different headaches

39
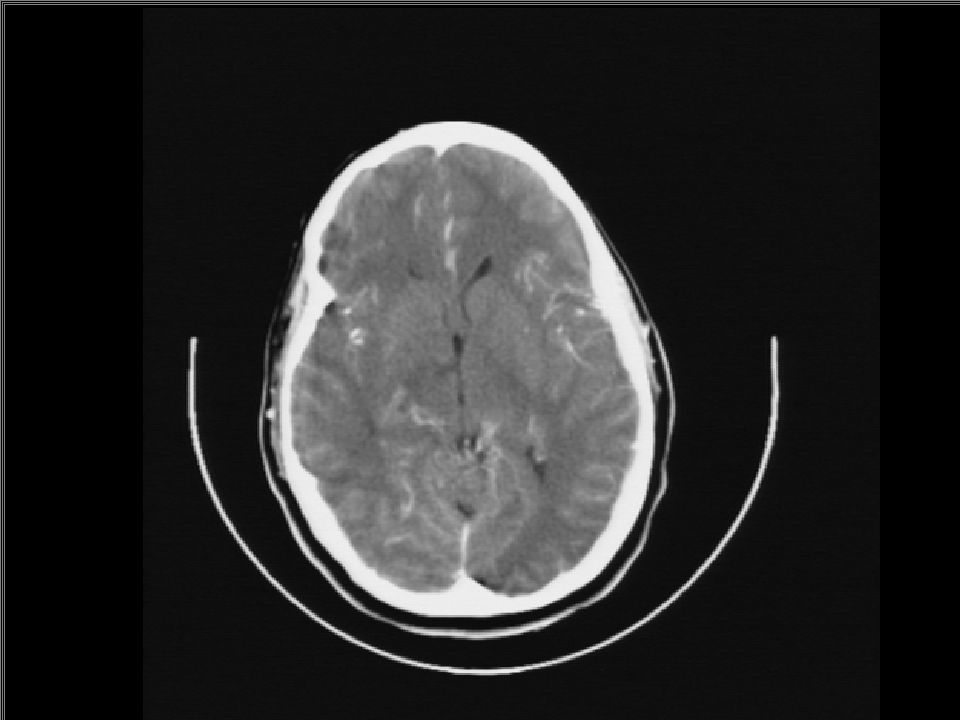
Can a CT Scan Safely “Rule Out” SAH?
First diagnostic study Thin cuts ( 3 mm) through base of brain Blood on CT function of Hgb Hgb < 10: blood isodense Sensitivity decreases over time from onset of symptoms
 through base of brain. Blood on CT function of Hgb. Hgb < 10: blood isodense. Sensitivity decreases over time from onset of symptoms.")
41
SAH CT Findings High density hemorrhage injury
(1) Interhemospheric fissure (2) Inferior frontal sulci (3) Third ventricle (4) Ambient cistern (5)Sylvian fissure
 Interhemospheric fissure. (2) Inferior frontal sulci. (3) Third ventricle. (4) Ambient cistern. (5)Sylvian fissure.")
43
SAH: CT Sensitivity Sames: Acad Emerg Med Jan 1996
181 patients; aged with SAH Sensitivity % pain < 24 hrs % pain > 24 hrs % LP 100% sensitive if neg CT “A normal NGCT does not reliably exclude the need for LP”

44
SAH Diagnosis: LP Needed Sidman: Acad Emerg Med Sep 1996
140 patients; aged 10-88 Sensitivity of CT < 12 hrs 80/ % > 12 hrs 49/ % Overall, 11/140 had (-) CT and (+) LP overall sensitivity %
 CT and (+) LP. overall sensitivity 92.1%")
45
Morgenstern LB, et al: Worst headache and SAH: Prospective, modern CT and spinal fluid analysis. Ann Emerg Med Sept 1998. 38,730 patients over 16 months, prospectively screened for “worst HA” Blinded neuroradiologists Neg CT LP cell count x 2 visual and spectrophotometric detection of xanthochromia CSF D-dimer assay

46
Morgenstern, et al: Ann Emerg Med 1998
455 headaches & 107 “worst headache” CT: 18 of 107 (17%): (+) SAH (-) CT/ (+) SAH: Only 2 (2.5%) (95% CI, 0.3%to 8.8%) Modern CT is sufficient to exclude 98% of SAH in patients
: (+) SAH. (-) CT/ (+) SAH: Only 2 (2.5%) (95% CI, 0.3%to 8.8%) Modern CT is sufficient to exclude 98% of SAH in patients.")
47
Morgenstern, et al: Ann Emerg Med 1998 (107 “Worst HA’s)
Variables CT-/LP CT+ CT-/LP+ Photophobia Stiff neck Nausea Lethargy Time < 24 h Migraine Headache

48
CT is Normal: Do LP? Yes!

49
What about LP First? Duffy et al; 1982: 55 patients who underwent LP as initial w/u Condition deteriorated immediately in 7 patients Hillman et al; 1986: 4 alert patients with SAH who deteriorated after lumbar puncture Both studies: clots on CT or a dilated pupil

50
Traumatic Taps 20% of LPs 0.5% and 6% has incidental intracranial aneurysm Impression or “3-tube” method not reliable in detecting traumatic tap Erythrocytes disseminate rapidly Released Hgb oxyhemoglobin xanthochromia bilirubin

51
Xanthochromia Bilirubin, enzyme-dependent process, is diagnostically more reliable but: takes up to 12 hours Timing is important CSF should be centrifuged and examined promptly so RBCs don’t undergo lysis in vitro, causing xanthochromia from oxyhemoglobin

52
Xanthochromia vs. Erythrocytes
primary criterion for SAH if neg CT advocates: spectrophotometry Erythrocytes considered more accurate by some used visual inspection which can miss discoloration in up to 50%

53
Timing the Tap With spectrophotometry, and waiting 12 hours after onset of headache: very accurate traumatic tap done earlier does not lead to xanthochromia and confusion Waiting: prolongation of ED stay risk “ultra-early” rebleeding

54
Normal CT & Persistently Bloody CSF ???
Not prudent to delay LP Without xanthochromia and clinical suspicion is high? Vascular imaging Xanthochromia present and clinical suspicion is high?

55
Differentiate Between
Traumatic LP and SAH CSF characteristic Traumatic tap True SAH Color gets lighter with subsequent tubes yes no RBC count in first & last tube count decrease stay constant Clotting of blood in CSF yes no present withi4 hrs of SAH, max at 1 wk, persists for about 3 weeks Xanthochromia in supernatant rare with RBC count less than 200,000

56
Thunderclap Headache: NL CT & NL LP Vascular Imaging?
Wijdicks et al; Lancet, 1988 Retrospective evaluation 71 patients no SAH in 3.3 years f/u Half dx’d with migraine or tension HA Markus 1991; Linn 1994; Harling 1989 117 patients no SAH, no sudden deaths

57
Vasospasm Occurs in 70% of patients with SAH
Appears after 3-4 days, peaks at 7-10 days, and resolves over 2-4 weeks Can be localized or involve several arteries Caused by factors released at time of bleeding that induce vasoconstriction and reduced blood flow

58
Calcium Channel Blocking Drugs
Drugs that limit transmembrane fluxes Vascular smooth muscle contraction Cell ischemia Platelet aggregation Selective cerebrovascular effects Cross blood-brain barrier Limited cardiovascular effects

59
Clinical Trials of Nimodipine
Nimodipine improves survival and functional recovery after SAH Benefits are due to its antihypertensive and neuronal protective effects

60
The Case (Continued) The patient had labs drawn, was given 5mg of morphine and sent off to CT scan. The CT scan revealed an acute SAH. The neurosurgeon ordered an angiogram which revealed an aneurysm. The patient went to the OR that day and was release with a normal neurological status 4 days later.

61
Case #2

62
First ED Visit: Late Friday Night
24 yo female with headache for 2 weeks, worse over the last 2 days 104/76, 80, 18, 98.1F Right frontal forehead, sharp, non-radiating, constant but waxing/waning, worse when she moved. (+) nausea (-) fever, photophobia, neck pain or visual changes
 nausea. (-) fever, photophobia, neck pain or visual changes.")
63
Past Medical/Social History
No recent trauma Smoker 1 PPD Social drinker No hx of headaches, except for last 2 weeks No allergies No meds except ibuprofen and acetaminophen recently – not helpful Worked as a part-time sales clerk

64
Exam: First Visit Alert, oriented, looked well except for discomfort of headache Face normal, Perrl, EOMI, fundi normal, TMs normal, mastoids non-tender, neck supple, motor neuro exam normal, normal gait, mental status normal

65
ED Therapy and Work Up Prochlorperazine 10 mg, by vein Acetaminophen 325/Oxycodone 5, orally CBC, Chem 7, UCG, CT Head without contrast

66
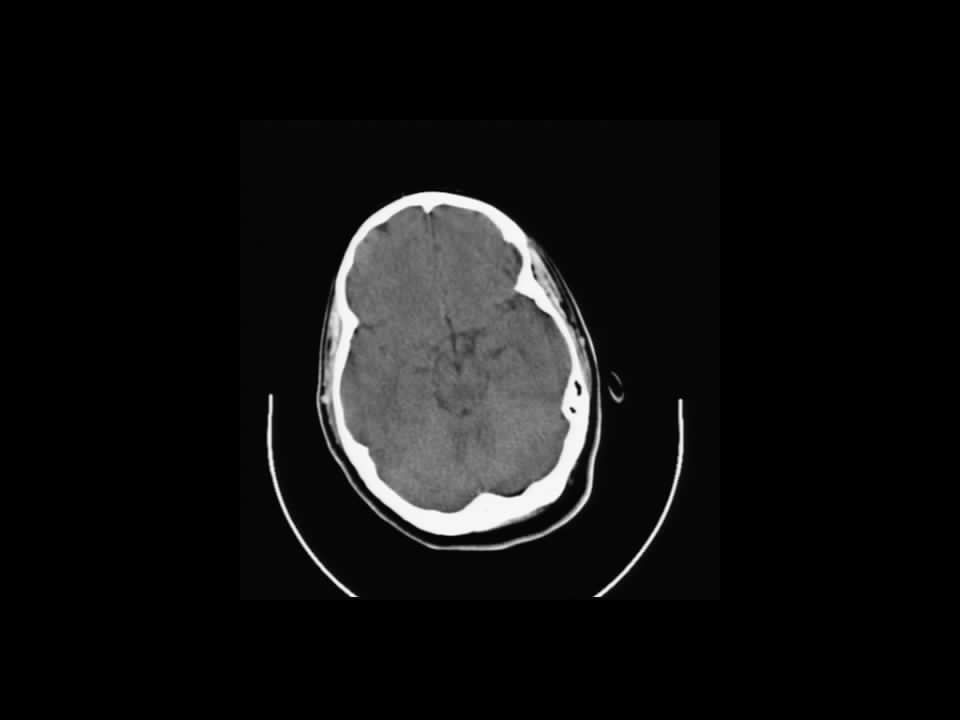
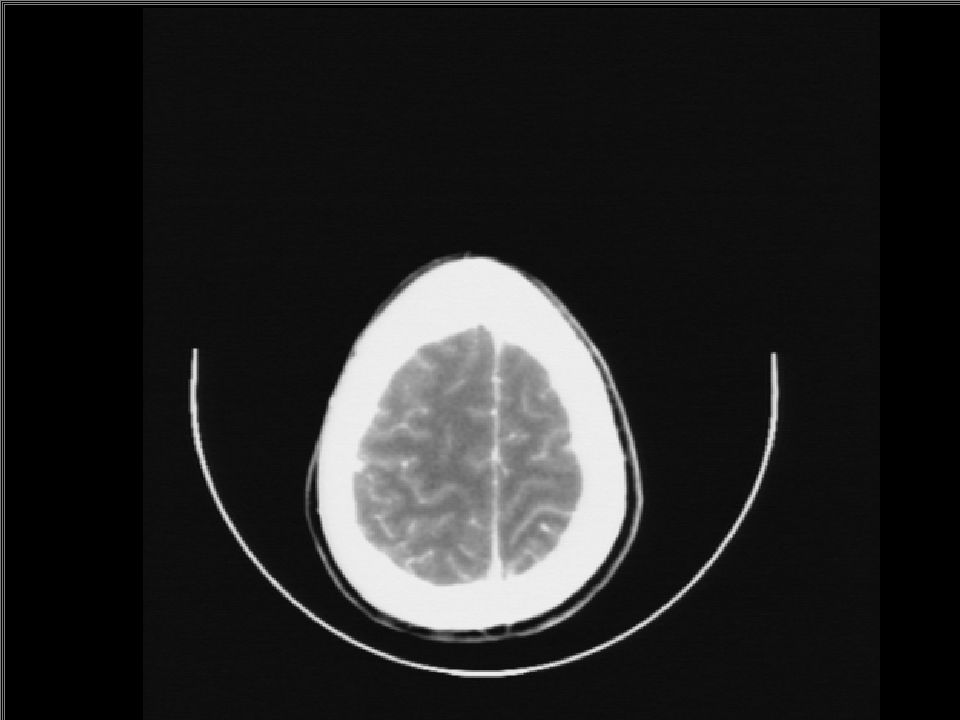
ED Diagnostic Results: Visit 1
WBC count 12.4K CT head reviewed by ED attending and radiology resident as negative

68
ED Disposition: Visit 1 Patient’s pain responded to medications
Patient discharged with prescription for acetaminophen/butalbital/caffeine = Fioricet

69
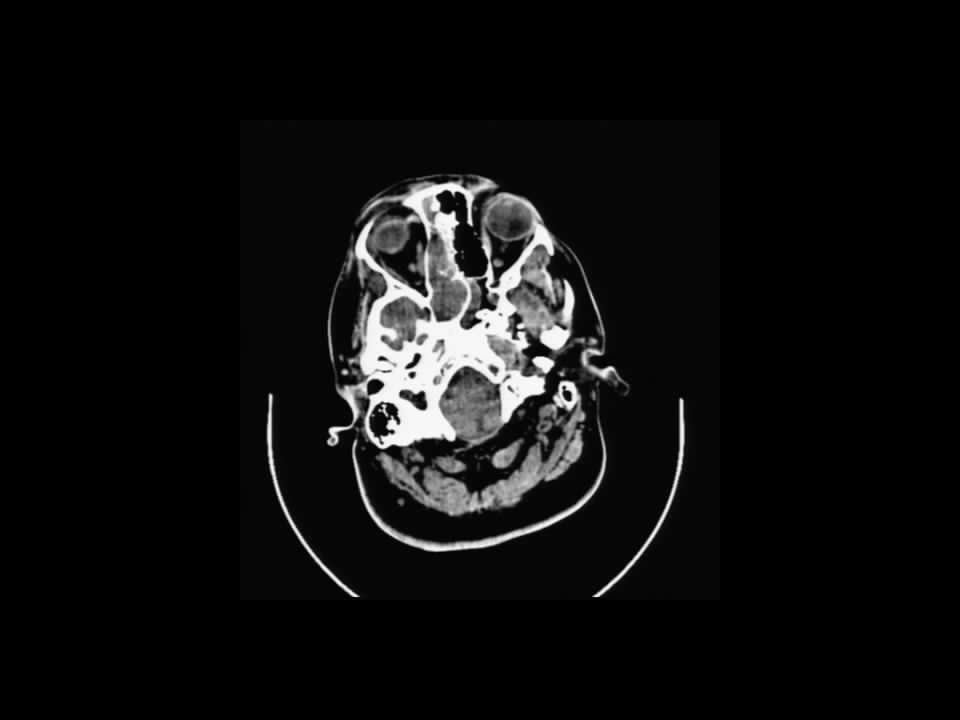
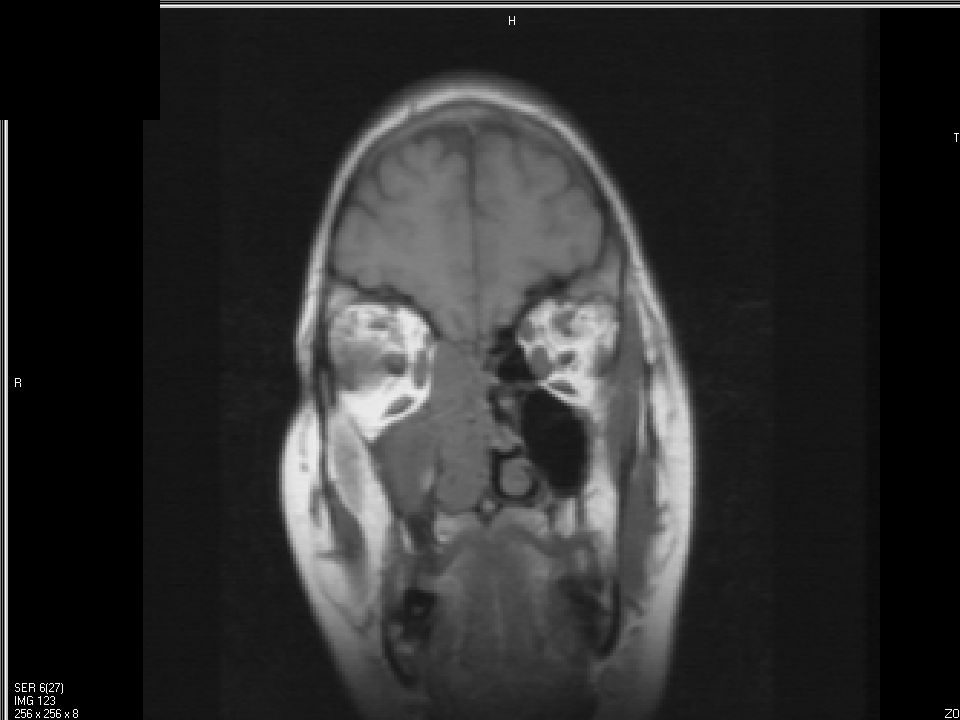
Radiology Over-Read: Monday AM (2.5 days since 1st ED visit)
Opacification of the right ethmoid and right sphenoid sinuses with expansion of the sphenoid septations toward the left. No intracranial disease

71
ED Discrepancy Procedure
Patient was contacted by phone and informed of sinus problem on CT Patient went to her PMD that afternoon PMD discharged her with prescription for levofloxacin

72
2nd ED Visit: Tuesday Morning (3.5 days after 1st ED visit)
New onset swelling and severe pain around left eye Continued, worsening right-sided headache Slept poorly, confused, hallucinating? 100/80, 96, 18, 101.9F

73
Morning Exam: 2nd Visit Left peri-orbital edema, erythema, proptosis, chemosis, severe pain with EOMs. Left pupil reacted to light. Ambulated in with normal gait. No obvious motor deficits. Awake. Followed simple commands, but mildly confused, answering slowly or incorrectly, with difficulty concentrating. (+) Nuchal rigidity
 Nuchal rigidity.")
74
ED Therapy & Work Up 2 grams ceftriaxone by vein after cultures
Repeat CT of brain and sinuses with contrast LP ID and ENT consults; vancomycin and metronidazole given by vein Admitted to MICU

77
Afternoon Exam: 2nd Visit
Deteriorating mental status. Mild left sided weakness left upper and left lower extremities.

78
ED Admitting Diagnoses
Orbital Cellulitis Meningitis Rule out Cavernous Sinus Thrombosis

79
Septic Dural Sinus Thrombosis Suppurative Intracranial Thrombophlebitis
Infected venous thrombosis of cortical veins or sinuses From meningitis, subdural empyema, epidural abscess, infection in the skin of the face, paranasal sinuses, middle ear, mastoid, maxillary teeth or neck. Iatrogenic cases have been associated with rhinoplasty, hip surgery and oral/dental surgery.

80
Non-Septic Dural Sinus Thrombosis
Dehydration from vomiting Hypercoagulable states Immunologic abnormalities, including the presence of circulating antiphospholipid antibodies

81
Septic Dural Sinus Thrombosis
Rare; 155 reported cases since 1940 Cavernous Sinus Thrombosis (CST) is the predominant subset (62%?) Fulminant, aggressive disease: mortality CST =30%, superior sagittal sinus thrombosis =78% Morbidity CST: 50% cranial nerve deficit; 17% visually impaired
 is the predominant subset (62% ) Fulminant, aggressive disease: mortality CST =30%, superior sagittal sinus thrombosis =78% Morbidity CST: 50% cranial nerve deficit; 17% visually impaired.")
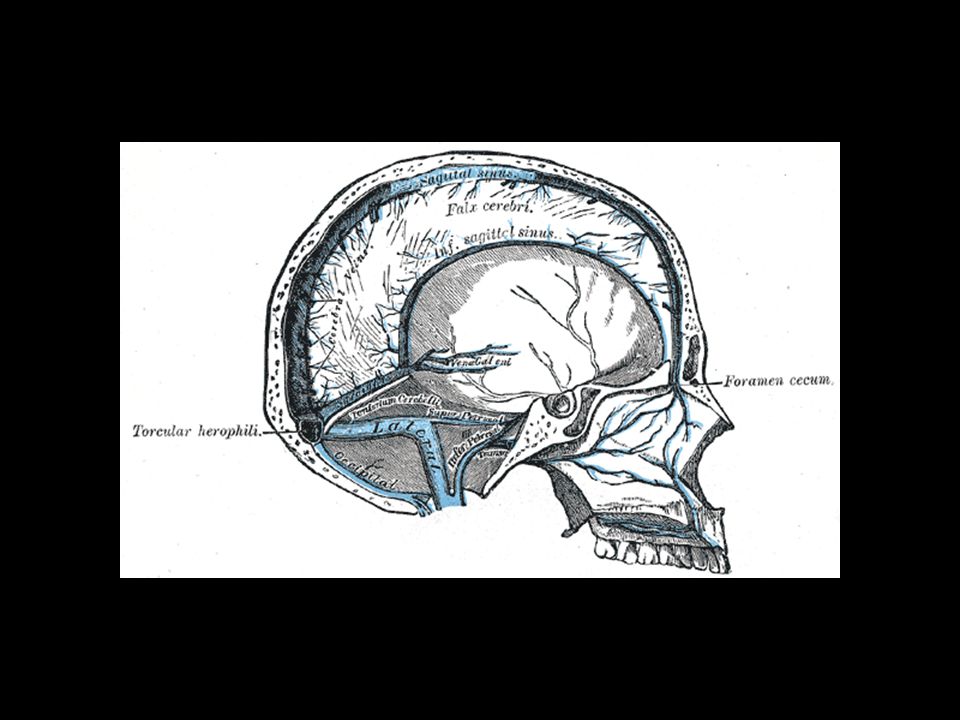
85
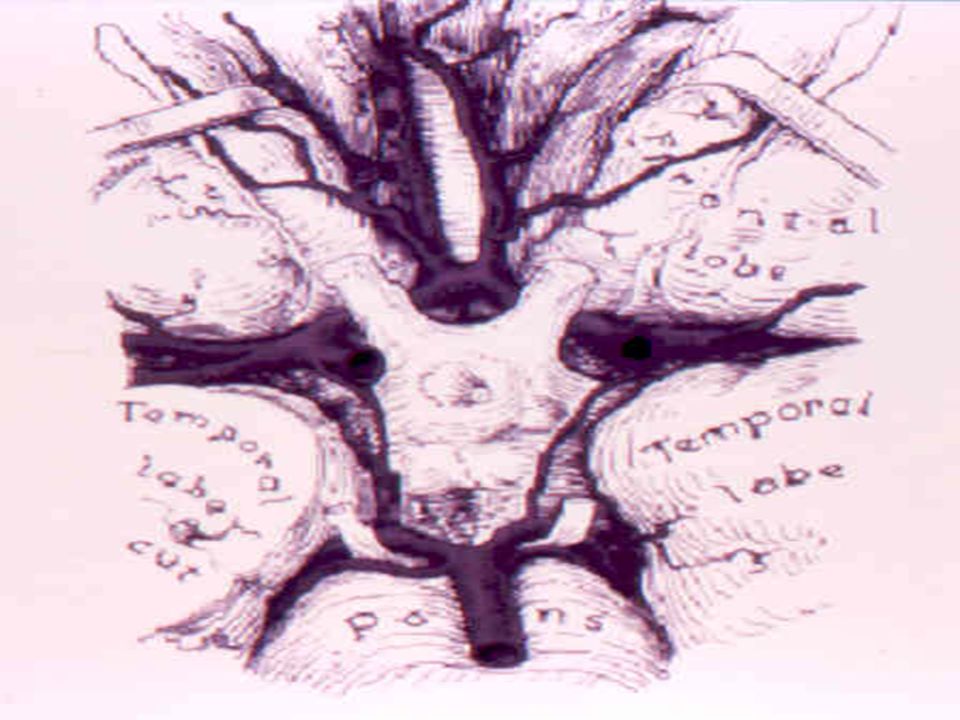
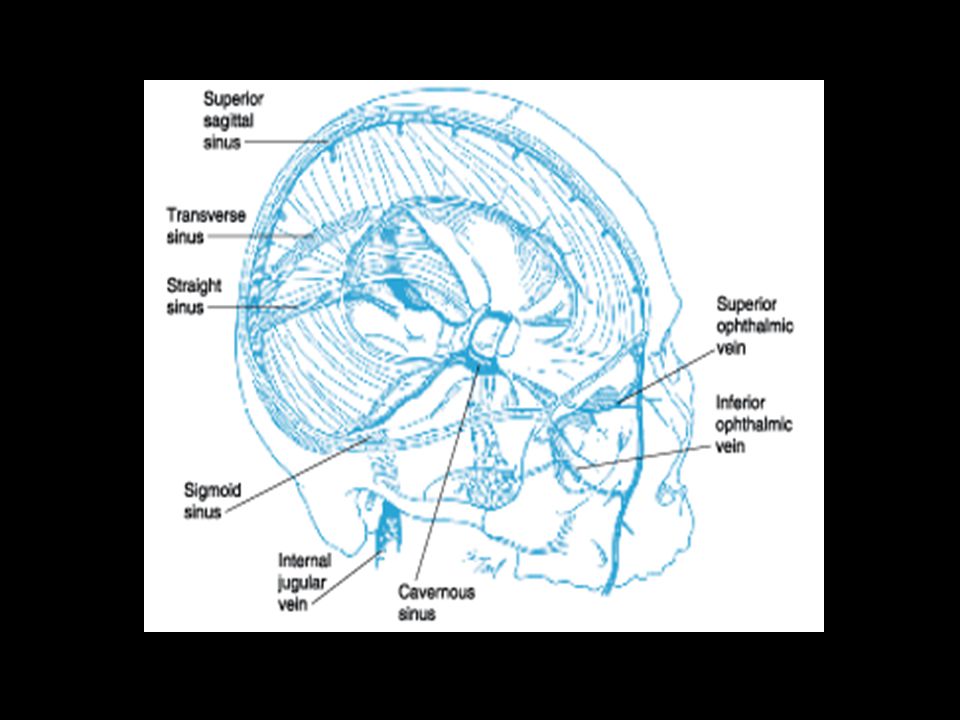
Schematic axial projection of the cavernous sinus and its venous anastomoses.

89
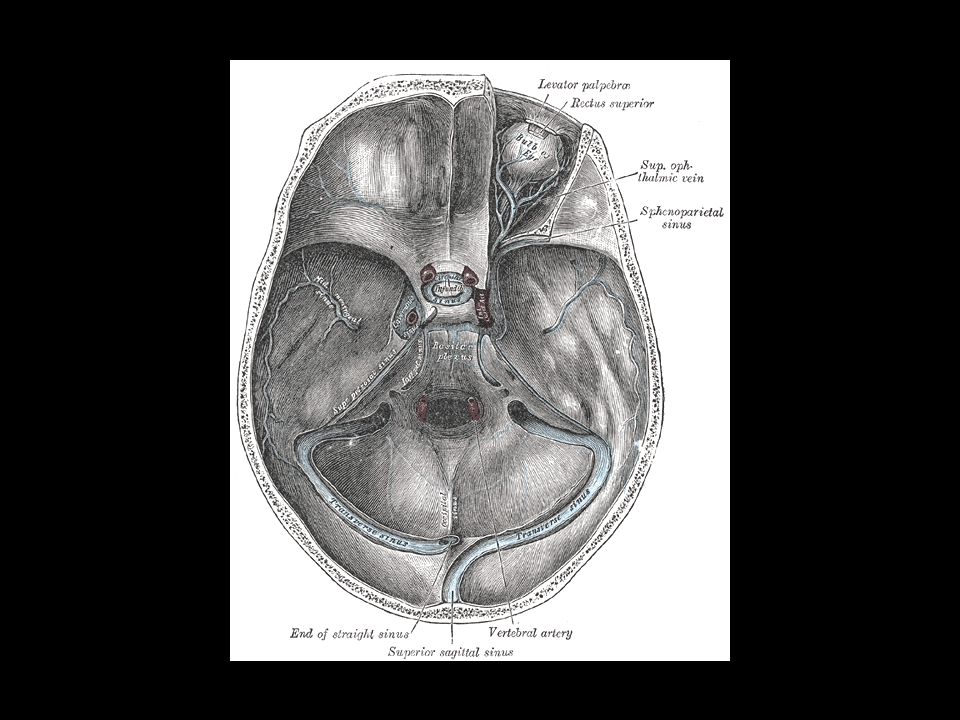
Coronal view of the cavernous sinus
Coronal view of the cavernous sinus. Cranial nerve III is the most superiorly situated nerve in the cavernous sinus. Cranial nerves III, IV, and the first two divisions of the trigeminal nerve, V1 and V2, travel in their respective nerve sheaths laterally in the cavernous sinus. Cranial nerve VI travels more medially within the cavernous sinus adjacent to the cavernous carotid artery. PG = Pituitary gland; S = sphenoid sinus; C = cavernous internal carotid artery.

90
Infected Thrombus Pathogens
CST: Staphylococcus aureus, other gram-positive organisms, and anaerobes. Lateral Sinus (otitis media and/or mastoid infection) Proteus species, Escherichia coli, S. aureus, and anaerobes. Superior Sagittal Sinus (meningitis or air sinus infection) - Streptococcus pneumoniae, S. aureus, other streptococci, and Klebsiella.
 Proteus species, Escherichia coli, S. aureus, and anaerobes. Superior Sagittal Sinus (meningitis or air sinus infection) - Streptococcus pneumoniae, S. aureus, other streptococci, and Klebsiella.")
91
ED Presentation: Superior Sagittal Sinus Thrombosis
Headache, nausea and vomiting, confusion, and focal or generalized seizures. Rapid development of stupor and coma. Weakness of the lower extremities with bilateral Babinski signs or hemiparesis is often present.

92
ED Presentation: Transverse Sinus Thrombosis
Headache and earache. Gradinego's syndrome: otitis media, sixth nerve palsy, and retro-orbital or facial pain. Sigmoid sinus and internal jugular vein thrombosis may present with neck pain.

93
ED Presentation: Cavernous Sinus Thrombosis
Sinusitis, midface infection for 5-10 days. Fever, headache, malaise, retro-orbital pain and diplopia, which generally precede….. Ptosis, proptosis, chemosis, eyelid edema, peri-orbital edema and extraocular dysmotility due to deficits of cranial nerves III, IV, and VI. Hypo- or hyperesthesia of the ophthalmic and maxillary divisions of V, decreased corneal reflex. dilated, tortuous retinal veins and papilledema. Meningeal signs: nuchal rigidity, Kernig and Brudzinski signs.

94
Diagnostic Studies CBC, diff, cultures
Sinus Films, CT, MR, MR Venography, Venous phase cerebral angiogram LP

100
ED Management Antibiotics: S aureus is the usual cause, broad-spectrum coverage for gram-positive, gram-negative, and anaerobic organisms also, pending cultures. Drain primary source of infection, if feasible (eg, sphenoid sinusitis, facial abscess). Anticoagulation in carefully selected cases of septic cavernous-sinus thrombosis, not other forms of septic dural-sinus thrombosis. Urokinase or rtPA? Corticosteroids?
. Anticoagulation in carefully selected cases of septic cavernous-sinus thrombosis, not other forms of septic dural-sinus thrombosis. Urokinase or rtPA Corticosteroids")
101
Consults ENT Neurology ID Intensive Care

102
Outcome of Case Day 1: Seizure, worsening deficit, intubated
Day 2: Heparinized, transient neuro improvement then relapse. Day 5: Sinuses drained Day 6: Brain dead Day 19: Demise

103
Acute Headache Questions ?

Similar presentations