Download presentation
Presentation is loading. Please wait.

1
Acute Pain Management Parisa Partownavid, MD Assistant Clinical Professor David Geffen School of Medicine at UCLA Department of Anesthesia

4
Definition of Pain An Unpleasant Sensory and Emotional Experience Associated with Actual or Potential Tissue Damage, or Described in Terms of Such Damage.

5
Acute Pain Pain in Perioperative Setting
Pain in Patients with Severe or Concurrent Medical Illnesses (Pancreatitis) Acute Pain Related to Cancer or Cancer Treatment Labor Pain
 Acute Pain Related to Cancer or Cancer Treatment. Labor Pain.")
8
Acute Perioperative Pain
Pain that is Present in a Surgical Patient Because of Preexisting Disease, the Surgical Procedure, or a Combination of Both

9
Importance of Pain Management
Adequate Pain Control Reduce the Risk of Adverse Outcomes Maintain the Patient’s Functional Ability, as well as Psychological Well-being Enhance the Quality of Life Shortened Hospital Stay and Reduced Cost

10
Adverse Outcomes Associated with Management of Acute Pain
Respiratory Depression Circulatory Depression Sedation Nausea and Vomiting Pruritus Urinary Retention Impairment of Bowel Function

11
Adverse Outcome of Undertreatment of Acute Pain
Thromboembolic or Pulmonary Complications Needless Suffering Development of Chronic Pain

12
The Incidence of Moderate to Severe Pain with Cardiac, Abdominal, and Orthopedic Inpatient Procedures has been Reported as High as 25%-50%, and Incidence of Moderate Pain after Ambulatory Procedures is 25% or Higher.

13
Goal Pain Management Interventions Should be Offered Around the Clock
Pain Management is to Provide Continuous Pain Relief Patient Should be Assessed for Adequacy of Pain Control

16
Preoperative Evaluation of the Patient
Type of Surgery Expected Severity of Postoperative Pain Underlying Medical Condition (Respiratory or Cardiac Disease)
")
17
Preoperative Preparation of the Patient
Adjustment or Continuation of Medications (Sudden Cessation may Provoke a Withdrawal Syndrome) Treatment to Reduce Preexisting Pain and Anxiety Patient and Family Education
 Treatment to Reduce Preexisting Pain and Anxiety. Patient and Family Education.")
18
Pain Assessment Tools

19
Pain Assessment Tools In Adults: Self Report Measurement Scales, such as Numerical Scales

20
Pain Assessment Tools In Pediatric Patients:
Physiologic and Behavioral Indicators of Pain ( Infants, Toddlers, Nonverbal or Critically Ill Children) Face Scale (Age 3-10 yrs) Visual Analogue Scales (Age 10-18)
 Face Scale (Age 3-10 yrs) Visual Analogue Scales (Age 10-18)")
23
Management of Acute Pain
Pharmacologic Interventional

24
Pharmacologic Management
Alter Nerve Conduction (Local Anesthetics) Modify Transmission in the Dorsal Horn (Opioids, Antidepressants)
 Modify Transmission in the Dorsal Horn (Opioids, Antidepressants)")
25
Routes of Administration
PO PR IV IM Transdermal Transmucosal Epidural Intrathecal

26
Opioid Analgesics Bind to Opioid Receptors: Mu, Delta and Kappa
Morphine, Hydromorphone, Meperidine, Fentanyl, Codeine, Methadone, Oxycodone, Hydrocodone, Tramodol Opioids may be Combined with NSAIDs to Enhance the Opioid Analgesic Effect

27
Opioid Analgesics Equianalgesic Conversion Charts are used when Converting form one Opioid to Another, or Converting from Parenteral to Oral Form Respiratory Monitors may be Used Depending on the Patients Age, Co-existing Medical Problems, or Route of Opioid Administered

28
Opioid Analgesics Conversions: Morphine
Oral Parenteral Epidural Intrathecal

29
Opioids Drug PO mg IV mg Comments 30 10 15-30 7.5 1.5 4-8 300 75 20
Starting Oral Dose mg Comments Morphine 30 10 15-30 MS Contin, Release 8-12 hrs MSIR for BTP Hydro-morphone 7.5 1.5 4-8 Duration Slightly Shorter than Morphine Meperidine 300 75 Normeperidine Causes CNS Toxicity Methadone 20 5-10 Qd Long Half-Life, hrs Accumulates on Days 2-3 Fentanyl Fentanyl Patch, 12 hrs Delay Onset and Offset

30
Opioids Drug PO mg Comments Precautions Codeine 30-60 Oxycodone 5-10
Combined With Nonnarcotic Analgesics Maximal Dose for Acetaminophen 4gm/d Oxycodone 5-10 Percocet Percodan Oxycodone 10-30mg Q 4h Oxycontin 10mg Q 12h Acetaminophen or Aspirin toxicity Hydro-codone Vicodin or Lortab Acetaminophen Toxicity Tramodol Q4-6hr Central Acting, Affinity for Mu Receptors Maximal Dose 400 mg/d

31
Patient Controlled Analgesia
Small Doses of Analgesic Drug (Usually Opioids), are Administered (IV) by Patient Allows Basal Infusion and Demand Boluses Over Dosage is Avoided by Limiting the Amount and Number of Boluses in a Set Period of Time
, are Administered (IV) by Patient. Allows Basal Infusion and Demand Boluses. Over Dosage is Avoided. by Limiting the Amount. and Number of Boluses. in a Set Period of Time.")
32
Dose Regimens for PCA Drug Bolus Dose (mg) Lock-Out (Minutes) Morphine
0.5-2 5-15 Hydromorphone 5-10 Fentanyl

33
Non-Opioid Analgesics
Acetaminophen NSAIDs (Aspirin, Ibuprofen, Ketorolac, COX-2 Inhibitors) Lidocaine Patch (Lidoderm)
 Lidocaine Patch (Lidoderm)")
34
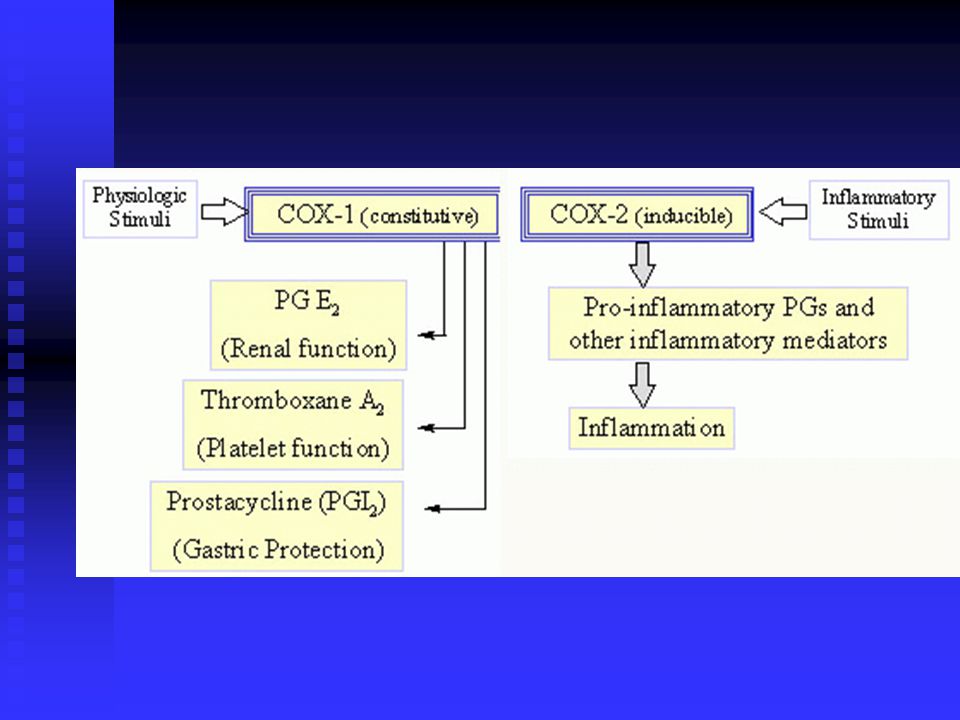
NSAIDs Relieve of Mild to Moderate Pain Complication: GI Discomfort
GI Bleeding (Inhibition of COX-1) Nephrotoxicity Inhibition of Platelet Aggregation Osteogenesis
 Nephrotoxicity. Inhibition of Platelet Aggregation. Osteogenesis.")
35
Ketorolac Potent Analgesic Parenteral (IV or IM) 15-30 mg Q 6hr
Patients Older than 16 yrs Should not Exceed 5 days

37
Cox-2 Inhibitors Drug Dose Celecoxib (Celebrex) 100-200mg PO Bid
Rofecoxib (Vioxx) Valdecoxib (Bextra) 10-20mg PO Qd Parecoxib 20-40mg IM 20-100mg IV
 Valdecoxib (Bextra) 10-20mg PO Qd. Parecoxib mg IM mg IV.")
38
Lidoderm

39
Lidoderm 5% Lidocaine Patch
Indicates for Pain Relief in Post-herpetic Neuralgia Each Patch Contains 700 mg of Lidocaine Should be Applied to Intact Skin About 3% is Absorbed 1-3 Patches Once a Day for 12 hrs

40
Interventional Management
Epidural Analgesia (Continuous Lumbar or Thoracic Epidural Catheter Placement, PCEA) Spinal Analgesia Peripheral Nerve Block ( Single Shot or Continuous)
 Spinal Analgesia. Peripheral Nerve Block ( Single Shot or Continuous)")
41
Anatomy of Epidural Space
Surrounds the Dural Sac Anteriorly: Post. Long. Ligament Posteriorly: Ligamentum Flavum Laterally: Pedicles and Intervertebral Foramina

42
Anatomy of Epidural Space
AP Dimension of the Epidural Space is Largest in the Lumbar Region, 5-6 mm In Thoracic Region the AP Dimension Decreases but the Space is More Continuous

43
MIDLINE SAGITTAL VIEW OF THE LUMBAR SPINE

53
Epidural Anesthesia Anesthestizes the Emerging Nerve Roots of the Spinal Cord Epidural Injection of Anesthetic Produces a Regional Dermatomal “band” of Anesthesia Spreading Cephalad and Caudad from the Site of Injection Level of Anesthesia Depends on : Volume of the Drug Level of Injection

54
Epidural Anesthesia Lumbar Epidural: Lower Extrimity, Pelvic, and Lower Abdominal Procedures Thoracic Epidural: Upper Abdomen and Thoracic Procedures Caudal Injection: More Commonly Used for Pediatric Patients (Genitourinary and Lower Abdominal Procedures)
")
55
Advantages Superior Pain Relief Less Systemic Side Effects
Lower Incidence of DVT and Pulmonary Emboli Decrease Blood Loss Intraoperatively during Orthopedic, Urologic, Gynecologic and Obstetric Procedures More Rapid Recovery of Bowel Function Earlier Ambulation Better PFT Suppression of Neuroendocrine Stress Response Grass JA. The Role of Epidural Anesthesia and Analgesia in Postoperative Outcome. Anesthesiol Clin North America 01-JUN-2000; 18(2):
:")
56
Contraindications Absolute Patient Refusal Coagulopathy Increased ICP
Skin Infection Relative Uncooperative Patient Pre-existing Neurologic Disorder Anatomical Abnormalities

57
Factors Affecting Epidural Dosage
Patient Factors: Age , Height, Weight, Pregnancy Site of Injection

58
Drugs Used for Epidural Anesthesia
Local Anesthetics Opioids

59
Local Anesthetics in Epidural Space
Lidocaine: 1-2% , min. Bupivacaine: % , min.

60
Opioids in Epidural Space
Drug Dosage Onset (min) Duration (hrs) Morphine 2-3 mg 30-90 6-24 Hydromor-phone mg 20-30 6-18 Fentanyl mcg 5-15 2-4
 Duration (hrs) Morphine. 2-3 mg Hydromor-phone mg Fentanyl mcg")
61
Hydrophilic Opioids Morphine, Hydromorphone Slow Onset, Long Duration, High CSF Solubility
Advantages Prolonged Single Dose Analgesia Thoracic Analgesia with Lumbar Administration Minimal Dose Compared with IV Administration Disadvantages Delayed Onset of Analgesia Unpredictable Duration Delayed Respiratory Depression

62
Lipophilic Opioids Fentanyl Rapid Onset, Short Duration, Low CSF Solubility
Disadvantages Systemic Absorption Brief Single Dose Analgesia Limited Thoracic Analgesia with Lumbar Administration Advantages Rapid Analgesia Ideal for Continuous Infusion or PCEA

63
PCEA Technique that Allows Basal Infusion and Demand Boluses into the Epidural Space Solutions Used: Local Anesthetics: % Bupivacaine Opioids: Morphine 50 mcg/ml Hydromorphone 10 mcg/ml Fentanyl 2-5 mcg/ml

64
Complications of Epidural Analgesia
Failure of Block (Patchy or Unilateral Block) Injury to Nerve Infection Epidural Hematoma or Abscess Dural Puncture (Total Spinal or PDPH)
 Injury to Nerve. Infection. Epidural Hematoma or Abscess. Dural Puncture (Total Spinal or PDPH)")
65
Complications of Epidural Analgesia
Side Effect of Drugs in Epidural Space - Hypotension Secondary to Sympathetic Blockade - Intravascular Injection (Local Anesthetic Toxicity) - Respiratory Depression - Sedation - Bladder Distention - Difficulty in Ambulation
 - Respiratory Depression. - Sedation. - Bladder Distention. - Difficulty in Ambulation.")
66
Spinal Anesthesia Spinal Anesthesia is Induced by Injecting Small Amount of Local Anesthetic (Bupivicaine) in the CSF Results in Rapid Onset of Block More Rapid Onset and Requiring less Medicine Compared to Epidural Analgesia

67
Spinal Anesthesia CSE, Used in Labor
Preservative Free Morphine (Duramorph) Provides Pain Relief for Abdominal, Pelvic, or Lower Extrimity Surgeries Complications Similar to Epidural Technique Except for Higher Risk of PDPH
 Provides Pain Relief for Abdominal, Pelvic, or Lower Extrimity Surgeries. Complications Similar to Epidural Technique Except for Higher Risk of PDPH.")
70
Peripheral Nerve Block
Anesthetizing the Nerve that is Innervating Surgical or Painful Area Single Shot or Continuous Infusion through Catheter Upper Extrimity: Brachial Plexus, Median, Ulnar or Radial Nerve

71
Peripheral Nerve Block
Lower Extrimity: Sciatic, Femoral, Posterior Tibial, Sural, Saphenous, Deep and Superficial Peroneal Nerve Intercostal Nerve Block Surgical Wound Infiltration of Local Anesthetic

80
Acute Pain Management for Pediatric Patients
Consider Physiologic and Anatomic Differences Pain Assessment and Communication Pain and Anxiety Associated with Minor Procedures or Unfamiliar Situations

83
Caudal Block Single Injection or Continuous Infusion through a Catheter Excellent Intraoperative and Postoperative Pain Control Easier to Perform in Children Analgesia that Last About 12 hrs if Bupivacaine Used Performed Following Induction of General Anesthesia

84
Indications for Caudal Block
Surgeries in Sacral Segments, (Circumcision and other Urologic Surgeries, Rectal Dilation) Combined with Light General Anesthesia Provides Adequate Intraoperative Analgesia
 Combined with Light General Anesthesia Provides Adequate Intraoperative Analgesia.")
85
Complications of Caudal Block
Infection Dural Puncture and Spinal Anesthesia Intravascular Injection of Local Anesthetics

87
Acute Pain Management in Elderly
Patient Population Older than 65 yrs of Age is Growing Age Related Physiologic Changes (Decreased Muscle Strength): Decreased Cough Decreased Mental Status (Dementia): Decreased Narcotic Dose
: Decreased Cough. Decreased Mental Status (Dementia): Decreased Narcotic Dose.")
88
Acute Pain Management in Elderly
Age Related Anatomic Changes: Difficulty in Placing Epidural Catheter Multiple Drug Therapy: Withdrawal or Interaction with Other Drugs

Similar presentations













































 Medical University of Sofia, Faculty of Medicine Department of Pharmacology and Toxicology.>")




