Download presentation
Presentation is loading. Please wait.

1
INTERSTITIAL LUNG DISEASE
SPEAKER-DR.SAGAR DNB MED.RES

2
INTRODUCTION ILDs represent a large number of conditions that involve the parenchyma of the lung—the alveoli, the alveolar epithelium, the capillary endothelium, and the spaces between these structures, as well as the perivascular and lymphatic tissues. Also called Diffuse Parenchymal Lung Disease

3
INTRODUCTION Heterogeneous group of disorders have similar clinical, roentgenographic, physiologic, or pathologic manifestations. Often associated with considerable morbidity and mortality, and there is little consensus regarding the best management of most of them.

4
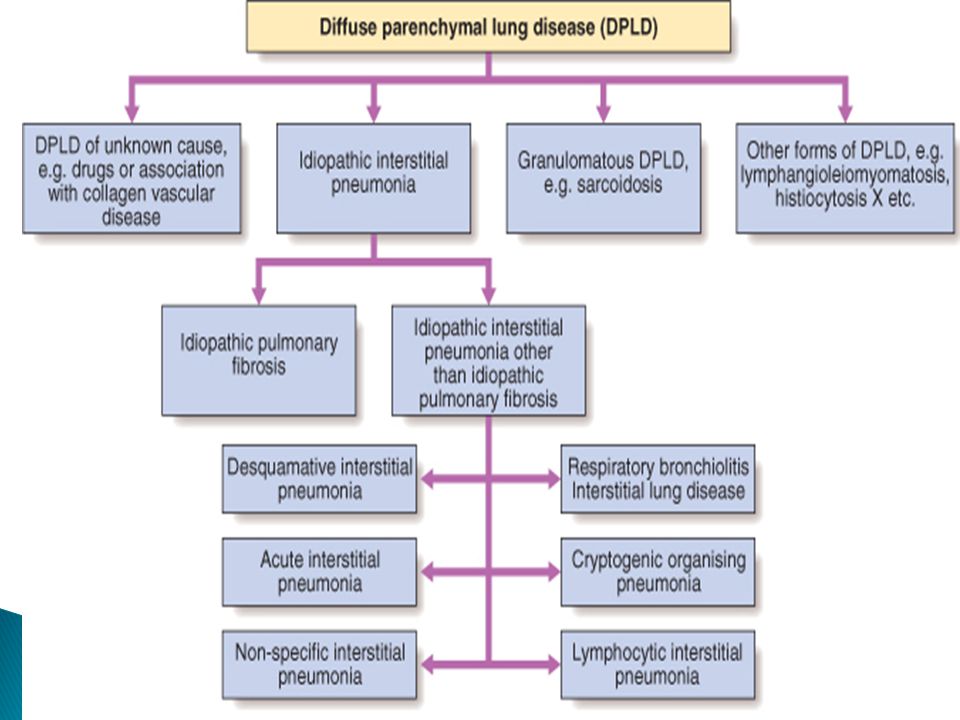
CLASSIFICATION One useful approach to classification is to separate the ILDs into two groups based on the major underlying histopathology: those associated with predominant inflammation and fibrosis, and those with a predominantly granulomatous reaction in interstitial or vascular areas Each of these groups can be further subdivided according to whether the cause is known or unknown. For each ILD there may be an acute phase, and there is usually a chronic one as well. Rarely, some are recurrent, with intervals of subclinical disease.

5
Major Categories of Alveolar and Interstitial Inflammatory Lung Disease
ON LUNG RESPONSE- Alveolitis, Interstitial Inflammation, and Fibrosis Granulomatous

6
Alveolitis, Interstitial Inflammation, and Fibrosis
Known Cause- Asbestos Fumes, gases Drugs (antibiotics, amiodarone, gold) and chemotherapy drugs Radiation Aspiration pneumonia Residual of adult respiratory distress syndrome
 and chemotherapy drugs. Radiation. Aspiration pneumonia. Residual of adult respiratory distress syndrome.")
7
UNKNOWN CAUSES Idiopathic interstitial pneumonias (IIP)-
Idiopathic pulmonary fibrosis (usual interstitial pneumonia) (UIP) Desquamative interstitial pneumonia(DIP) Respiratory bronchiolitis-associated interstitial lung disease (RB-ILD) Acute interstitial pneumonia (diffuse alveolar damage) Cryptogenic organizing pneumonia (bronchiolitis obliterans with organizing pneumonia) (COD) Nonspecific interstitial pneumonia Connective tissue diseases- Systemic lupus erythematosus, rheumatoid arthritis, ankylosing spondylitis, systemic sclerosis, Sjögren's syndrome, polymyositis-dermatomyositis Pulmonary hemorrhage syndromes Goodpasture's syndrome, idiopathic pulmonary hemosiderosis, isolated pulmonary capillaritis
 (UIP) Desquamative interstitial pneumonia(DIP) Respiratory bronchiolitis-associated interstitial lung disease (RB-ILD) Acute interstitial pneumonia (diffuse alveolar damage) Cryptogenic organizing pneumonia (bronchiolitis obliterans with organizing pneumonia) (COD) Nonspecific interstitial pneumonia. Connective tissue diseases- Systemic lupus erythematosus, rheumatoid arthritis, ankylosing spondylitis, systemic sclerosis, Sjögren s syndrome, polymyositis-dermatomyositis. Pulmonary hemorrhage syndromes. Goodpasture s syndrome, idiopathic pulmonary hemosiderosis, isolated pulmonary capillaritis.")
8
CONT… Pulmonary alveolar proteinosis
Lymphocytic infiltrative disorders (lymphocytic interstitial pneumonitis associated with connective tissue disease) Eosinophilic pneumonias Lymphangioleiomyomatosis (LAM) Amyloidosis Inherited diseases- Tuberous sclerosis, neurofibromatosis, Niemann-Pick disease, Gaucher's disease, Hermansky-Pudlak syndrome Gastrointestinal or liver diseases -(Crohn's disease, primary biliary cirrhosis, chronic active hepatitis, ulcerative colitis) Graft-vs.-host disease- (bone marrow transplantation; solid organ transplantation)
 Eosinophilic pneumonias. Lymphangioleiomyomatosis (LAM) Amyloidosis. Inherited diseases- Tuberous sclerosis, neurofibromatosis, Niemann-Pick disease, Gaucher s disease, Hermansky-Pudlak syndrome. Gastrointestinal or liver diseases -(Crohn s disease, primary biliary cirrhosis, chronic active hepatitis, ulcerative colitis) Graft-vs.-host disease- (bone marrow transplantation; solid organ transplantation)")
9
Granulomatous Known Cause-
Hypersensitivity pneumonitis (organic dusts) Inorganic dusts: beryllium, silica
 Inorganic dusts: beryllium, silica.")
10
Unknown Cause(GRANULOMATOUS)
Sarcoidosis Langerhans' cell granulomatosis (eosinophilic granuloma of the lung) Granulomatous vasculitides-- Wegener's granulomatosis, allergic granulomatosis of Churg-Strauss Bronchocentric granulomatosis Lymphomatoid granulomatosis
 Granulomatous vasculitides-- Wegener s granulomatosis, allergic granulomatosis of Churg-Strauss. Bronchocentric granulomatosis. Lymphomatoid granulomatosis.")
11
Incident Cases of ILD (Incidence of IPF=26-31 per 100,000) DILD=drug
Fibrosis=IPF (Incidence of IPF=26-31 per 100,000)
")
13
What is the Pulmonary Interstitium?
Interstitial compartment is the portion of the lung sandwiched between the epithelial and endothelial basement membrane Expansion of the interstitial compartment by inflammation with or without fibrosis Necrosis Hyperplasia Collapse of basement membrane Inflammatory cells

16
Clinical Assessment History Physical Exam Chest Imaging
Pulmonary Function Testing At Rest Exercise Serologic Studies Tissue examination

17
History: Age and Gender
FEMALES- LAM Tuberous sclerosis MALES- Pneumoconiosis

18
History: Medications www.pneumotox.com
Schwartz, ILD text book, 4th edition

19
History: Occupational and Environmental
INORGANIC

20
ORGANIC: Hypersensitivity Pneumonitis

21
Occupational ????

22
History: Duration of Illness
Acute Diseases (Days to weeks) AIP, EP, Drugs, Hypersensitivity ________________________________________________________________________________________________________________ Subacute Diseases (weeks to months) Sarcoid, Drug, COP __________________________________________________________________________________________________________________ Chronic Diseases (months to years) IPF, Pneumoconioses,LCH,Sarcoidosis
 AIP, EP, Drugs, Hypersensitivity. ________________________________________________________________________________________________________________. 2. Subacute Diseases (weeks to months) Sarcoid, Drug, COP. __________________________________________________________________________________________________________________. 3. Chronic Diseases (months to years) IPF, Pneumoconioses,LCH,Sarcoidosis.")
23
PRESENTATION Dyspnea is a common and prominent complaint in patients with ILD. Non-Productive Cough Fatigue,Weight loss Symptoms associated with other diseases Clubbing ,cyanosis

24
EXAMINATION Late inspiratory ‘Velcro’ crackles unaltered by coughing at lung bases are heard. Features of RV failure Loud P2 present.

25
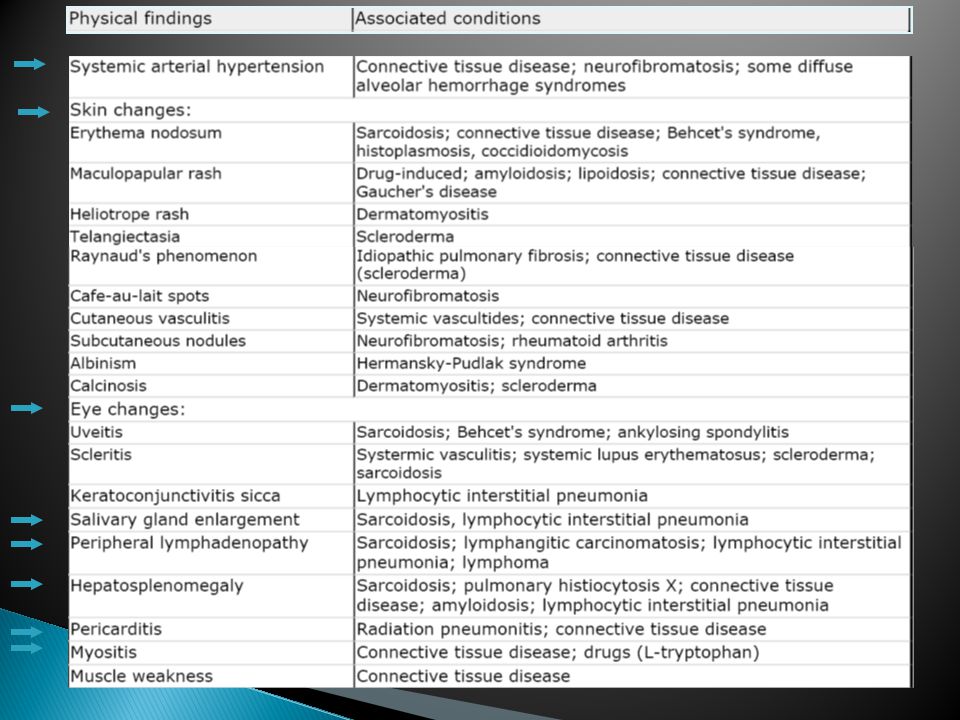
Physical Findings Resting Tachypnea Shallow breathing Dry crackles
Digital clubbing Pulmonary HTN Non-pulmonary findings In a normal finger, the length of the perpendicular dropped from point A to point B should be greater than a similar line from C to D. In clubbing, the relationships are reversed - that is, the distance C-D is greater than the distance A-B. The other important change is the angle described by A-C-E. In the normal finger this is usually <180 degrees whereas in clubbing it is >180 degrees. Redrawn from DeRemee, RA. Facets of the algorithmic synthesis. In: DeRemee, RA, (Ed), Clinical profiles of diffuse interstitial pulmonary disease, Mount Kisco, NY, Futura Publishing Company, Inc, 1990, pp
, Clinical profiles of diffuse interstitial pulmonary disease, Mount Kisco, NY, Futura Publishing Company, Inc, 1990, pp")
27
Localized thickening and tightness of the skin of the fingers or toes
Localized thickening and tightness of the skin of the fingers or toes. Sclerodactyly is commonly associated with atrophy of the underlying soft tissues.

29
Laboratory

30
ILD: Evaluation Radiographic Physiologic testing Lung Sampling CXR
HRCT Physiologic testing PFT Exercise test Lung Sampling BAL Lung biopsy: (TBBx, Surgical)
")
31
CXR CLUES Interstitial Infiltrates Nodular Linear or reticular Mixed
Honeycomb Cysts and traction bronchiectasis GGO nodules, lines, honeycombing, and groundglass opacification.

32
CXR CLUES Alveolar Filling Air-bronchograms Acinar rosettes
Diffuse consolidation Nodule like, poor boarder definition Silhouetting: obliteration of normal structures

33
Radiographic Patterns in ILD
Pleural Involvement Adenopathy Sarcoidosis Lymphoma Lymphangitic CA Amyloidosis Berylliosis Silicosis Kerley B lines Lymphangitic Carcinomatosis LAM Drug Induced Radiation Pneumonitis Asbestosis Effusion Thickening Plaques Mesothelioma Collagen vascular disease Chronic LV failure Lymphangitic CA Lymphoma LAM Veno-occlusive disease Acute Eosinophilic Pneumonia

34
IPF: CXR Reduced lung volume Basal and peripheral reticulation
Chest Radiograph in IPF These chest radiographs show peripheral reticular opacities that predominate at the lung bases, but also involve the mid-lung zones. Lung volume is reduced. Reduced lung volume Basal and peripheral reticulation Images courtesy of W. Richard Webb, MD.

35
CXR: LlMITATIONS CXR is normal:
in 10 to 15 % of symptomatic patients with proven infiltrative lung disease 30% of those with bronchiectasis ~ 60 % of patients with emphysema CXR has a sensitivity of 80% and a specificity of 82% percent for detection of DPLD CXR can provide a confident diagnosis in ~ 23 % of cases

36
A normal CXR does not rule out the presence of ILD

37
HRCT 2 essential technical factors: Does not use contrast
Narrow collimation Use of a high spatial frequency reconstruction algorithm Does not use contrast Prone and supine Inspiratory and expiratory

38
Characteristic HRCT findings
Bibasilar interstitial and intralobular reticular opacities Interlobular septal thickening Subpleural honeycomb changes Traction bronchiectasis in the lower lobes. There may also be a variable amount of ground-glass opacity.

39
HRCT Conventional Supine Prone

40
The terminal bronchiole in the center divides into respiratory bronchioles with acini that contain alveoli. Lymphatics and veins run within the interlobular septa Centrilobular area in blue (left) and perilymphatic area in yellow (right) It is the smallest lung unit that is surrounded by connective tissue septa. It measures about 1-2 cm and is made up of 5-15 pulmonary acini, that contain the alveoli for gas exchange. The secondary lobule is supplied by a small bronchiole (terminal bronchiole) in the center, that is parallelled by the centrilobular artery. Pulmonary veins and lymphatics run in the periphery of the lobule within the interlobular septa. Under normal conditions only a few of these very thin septa will be seen. There are two lymphatic systems: a central network, that runs along the bronchovascular bundle towards the centre of the lobule and a peripheral network, that is located within the interlobular septa and along the pleural linings.
 and perilymphatic area in yellow (right) It is the smallest lung unit that is surrounded by connective tissue septa. It measures about 1-2 cm and is made up of 5-15 pulmonary acini, that contain the alveoli for gas exchange. The secondary lobule is supplied by a small bronchiole (terminal bronchiole) in the center, that is parallelled by the centrilobular artery. Pulmonary veins and lymphatics run in the periphery of the lobule within the interlobular septa. Under normal conditions only a few of these very thin septa will be seen. There are two lymphatic systems: a central network, that runs along the bronchovascular bundle towards the centre of the lobule and a peripheral network, that is located within the interlobular septa and along the pleural linings.")
41
HRCT Clues What is the dominant HR-pattern:
Reticular Nodular High attenuation (ground-glass, consolidation) Low attenuation (emphysema, cystic) Where is it located within the secondary lobule (centrilobular, perilymphatic or random) Is there an upper versus lower zone? Central versus peripheral predominance Are there additional findings (pleural involvement, lymphadenopathy, traction bronchiectasis)
 Low attenuation (emphysema, cystic) Where is it located within the secondary lobule (centrilobular, perilymphatic or random) Is there an upper versus lower zone Central versus peripheral predominance. Are there additional findings (pleural involvement, lymphadenopathy, traction bronchiectasis)")
42
HRCT: Radiographic Pattern

43
HRCT Findings in Late IPF
Characteristic HRCT findings include bibasilar interstitial and intralobular reticular opacities, interlobular septal thickening, subpleural honeycomb changes, and traction bronchiectasis in the lower lobes, without pleural abnormalities. There may also be a variable amount of ground-glass opacity. However, extensive ground-glass opacity on CT of the lung (involvement of ≥30% of lung) should prompt consideration of another cause of IIF This HRCT scan shows a reticular pattern with a predominantly subpleural distribution in a patient with mid- to late-stage IPF Septa[ thickening and honeycombing are also seen. American Thoracic Society, European Respiratory Society. Idiopathic pulmonary fibrosis: diagnosis and treatment. International Consensus Statement. Am J Respir Crit Care Med. 2000;161: Slide courtesy of Ganesh Raghu, MD.
 should prompt consideration of another cause of IIF. This HRCT scan shows a reticular pattern with a predominantly subpleural distribution in a patient with mid- to late-stage IPF Septa[ thickening and honeycombing are also seen. American Thoracic Society, European Respiratory Society. Idiopathic pulmonary fibrosis: diagnosis and treatment. International Consensus Statement. Am J Respir Crit Care Med. 2000;161: Slide courtesy of Ganesh Raghu, MD.")
44
Honeycomb lung

45
Classic IPF HRCT Basal and subpleural predominance Reticular opacities
HRCT near the lung bases shows subpleural reticulation with traction bronchiectasis. Subpleural honeycombing is also present. Honeycombing can be confidently diagnosed if air-filled cysts are visible in a subpleural location. Reticular opacities Traction bronchiectasis Honeycombing Image courtesy of W. Richard Webb, MD.

46
Ground Glass Pattern HP PCP pneumonia DIP NSIP PAP DAH Fluid

47
Cysts or Cyst Like Bronchiectasis LAM EG E

48
PFT: Lung Volumes Restrictive Disease
TLC RV VC Normal ILD NM Disease

49
DLCO AND ABG DLCO reduced but nonspecific.
Does not correlate with severity of disease ABG- Normal to severe hypoxemia Retained CO2 rare ..in end stage disease

50
Fiberoptic Bronchoscopy and Bronchoalveolar Lavage (BAL)
In selected diseases (e.g., sarcoidosis, hypersensitivity pneumonitis, DAH syndrome, cancer, pulmonary alveolar proteinosis) Useful in narrowing D/D Usefulness of BAL in the clinical assessment and management remains to be established
 Useful in narrowing D/D. Usefulness of BAL in the clinical assessment and management remains to be established.")
51
Tissue and Cellular Examination
Most effective method in confirming diagnosis and assessment of disease May identify a more treatable process than originally suspected Avoids confusion and anxiety later in the clinical course if the patient does not respond to therapy or suffers serious side effects from it.

52
Biopsy Fiberoptic bronchoscopy initial procedure of choice.
If specific diagnosis not made. Then VATS or Surgical biopsy can be done

53
Probability of Histologic Diagnosis of Diffuse Diseases
Transbronchial Biopsy Surgical Biopsy 1. Granulomatous diseases Often 2. Malignant tumors/lymphangitic 3. DAD (any cause) 4. Certain infections 5. Alveolar proteinosis 6. Eosinophilic pneumonia 7. Vasculitis Sometimes 8. Amyloidosis 9. EG/HX/PLCH 10. LAM Probability of Histologic Diagnosis of Diffuse Diseases UIP is histologically identified by surgical lung biopsy (SLB). SLB is recommended if IPF is suspected, and particularly in cases with atypical clinical or radiologic features. Transbronchial biopsy (TBBx) has limited value in making a definitive diagnosis of UIP. TBBx is most useful in identifying diseases that affect the central structures within the lung lobule, such as granulomatous diseases, malignant tumors, DAD, and the rest of the diseases listed as 16 in the table. It is sometimes useful if the diagnostic lesion is encompassed in the transbronchial biopsy, as in amyloidosis or vasculitis. However, TBBx is almost never a useful diagnostic tool for diseases such as UIP, even though features may be suggestive of UIP. 11. RB/RBILD/DIP Never 12. UIP/NSIP/LIP COP 13. Small airways disease 14. PHT and PVOD Courtesy of Kevin O. Leslie, MD.
 4. Certain infections. 5. Alveolar proteinosis. 6. Eosinophilic pneumonia. 7. Vasculitis. Sometimes. 8. Amyloidosis. 9. EG/HX/PLCH. 10. LAM. Probability of Histologic Diagnosis of Diffuse Diseases. UIP is histologically identified by surgical lung biopsy (SLB). SLB is recommended if IPF is suspected, and particularly in cases with atypical clinical or radiologic features. Transbronchial biopsy (TBBx) has limited value in making a definitive diagnosis of UIP. TBBx is most useful in identifying diseases that affect the central structures within the lung lobule, such as granulomatous diseases, malignant tumors, DAD, and the rest of the diseases listed as 16 in the table. It is sometimes useful if the diagnostic lesion is encompassed in the transbronchial biopsy, as in amyloidosis or vasculitis. However, TBBx is almost never a useful diagnostic tool for diseases such as UIP, even though features may be suggestive of UIP. 11. RB/RBILD/DIP. Never. 12. UIP/NSIP/LIP COP. 13. Small airways disease. 14. PHT and PVOD. Courtesy of Kevin O. Leslie, MD.")
54
Video Assisted Thoracic Surgery (VATS)
VATS is the preferred procedure for obtaining a lung biopsy High diagnostic accuracy Less morbidity and mortality than open lung biopsy BAL and TBBx limited to excluding other IPF mimickers Ideal biopsy Two or more surgical wedge biopsies with areas of normal lung Samples should measure 35 cm in length and 23 cm in depth Outpatient thoracoscopic lung biopsy can be a safe and effective procedure for patients with interstitial or focal lung disease Video Assisted Thoracic Surgery (VATS) The surgical lung biopsy is often indicated to establish a diagnosis of UIP. Video Assisted Thoracic Surgery (VATS) is a less invasive alternative to open lung biopsy for obtaining sufficient tissue and has been shown to provide a high degree of diagnostic accuracy and safety. Videothoracoscopy reduces postoperative pain and pulmonary dysfunction and is often associated with no or lower mortality compared with open lung biopsy. A recent study demonstrated that outpatient thoracoscopic lung biopsy was safe and effective in diagnosing patients with ILD. 72.5% of patients in the study were discharged within 8 hours of admission and 22.5% went home within 23 hours. American Thoracic Society. Idiopathic pulmonary fibrosis: diagnosis and treatment. International Consensus Statement. Am J Respir Crit Care Med. 2000;161: Chang AC, Yee J, Orringer MB, Iannettoni MD. Diagnostic thoracoscopic lung biopsy: an outpatient experience. Ann Thorac Surg ; Rena O, Casadio C, Leo F, et al. Videothoracoscopic lung biopsy in the diagnosis of interstitial lung disease. Eur J Cardiothorac Surg. 1999;16:
 The surgical lung biopsy is often indicated to establish a diagnosis of UIP. Video Assisted Thoracic Surgery (VATS) is a less invasive alternative to open lung biopsy for obtaining sufficient tissue and has been shown to provide a high degree of diagnostic accuracy and safety. Videothoracoscopy reduces postoperative pain and pulmonary dysfunction and is often associated with no or lower mortality compared with open lung biopsy. A recent study demonstrated that outpatient thoracoscopic lung biopsy was safe and effective in diagnosing patients with ILD. 72.5% of patients in the study were discharged within 8 hours of admission and 22.5% went home within 23 hours. American Thoracic Society. Idiopathic pulmonary fibrosis: diagnosis and treatment. International Consensus Statement. Am J Respir Crit Care Med. 2000;161: Chang AC, Yee J, Orringer MB, Iannettoni MD. Diagnostic thoracoscopic lung biopsy: an outpatient experience. Ann Thorac Surg ; Rena O, Casadio C, Leo F, et al. Videothoracoscopic lung biopsy in the diagnosis of interstitial lung disease. Eur J Cardiothorac Surg. 1999;16:")
55
Major goals of treatment
Permanent removal of the offending agent, when known Early identification and aggressive suppression of the acute and chronic inflammatory process thereby reducing further lung damage

56
Hypoxemia (PaO2 < 55 mmHg) at rest and/or with exercise should be managed by supplemental oxygen.
If cor pulmonale develops, diuretic therapy and phlebotomy may occasionally be required

57
TREATMENT Glucocorticoid therapy is recommended-
for symptomatic ILD patients with eosinophilic pneumonias, COP, CTD, sarcoidosis, acute inorganic dust exposures, acute radiation pneumonitis, DAH, and drug- induced ILD In organic dust disease, glucocorticoids are recommended for both the acute and chronic stages.

58
GLUCOCORTICOIDS A common starting dose is prednisone, 0.5–1 mg/kg in a once-daily oral dose for 4–12 weeks. If the patient is stable or improved, the dose is tapered to 0.25–0.5 mg/kg for an additional 4– 12 weeks depending on the course. Rapid tapering or a shortened course of glucocorticoid treatment can result in recurrence. If the patient's condition continues to decline while on glucocorticoids, a second agent added and the prednisone dose is lowered to or maintained at 0.25 mg/kg per day.

59
Other agents Cyclophosphamide and azathioprine (1–2 mg/kg lean body weight per day), with or without glucocorticoids in IPF, vasculitis, and other ILDs. An objective response usually requires at least 8–12 weeks to occur Other agents, including methotrexate, colchicine, penicillamine, and cyclosporine, have been tried. However, their role in the treatment of ILDs remains to be determined
, with or without glucocorticoids in IPF, vasculitis, and other ILDs. An objective response usually requires at least 8–12 weeks to occur. Other agents, including methotrexate, colchicine, penicillamine, and cyclosporine, have been tried. However, their role in the treatment of ILDs remains to be determined.")
60
LUNG TRANSPLANTATION Many cases of ILD are chronic and irreversible despite the therapy discussed above, and lung transplantation may then be considered

61
Idiopathic Pulmonary Fibrosis: Treatment
No therapy effective in the management of acute exacerbations of IPF Often mechanical ventilation is required but is usually not successful, with a hospital mortality rate of up to three-fourths of the patients. In those that survive, a recurrence of acute exacerbation is common and usually results in death at those times.

62
Nonspecific Interstitial Pneumonia (NSIP)
DIP AIP Idiopathic BOOP.

63
NSIP

64
TREATMENT OF NSIP Unlike patients with IPF (UIP),
Majority of patients with NSIP have a good prognosis (5-year mortality rate estimated at <15%) with most showing improvement after treatment with glucocorticoids, often used in combination with azathioprine
 with most showing improvement after treatment with glucocorticoids, often used in combination with azathioprine.")
65
Acute Interstitial Pneumonia (AIP, Hamman-Rich Syndrome)
Fulminant form of lung injury -RARE Diffuse alveolar damage on lung ARDS like presentation.D/D Idiopathic ARDS Pathologic confirmation of organizing diffuse alveolar damage Treatment –supportive-Ventilation. Steroids role controversial

66
Cryptogenic Organizing Pneumonia
Idiopathic BOOP clinicopathologic syndrome of unknown etiology. 5-6th decade Distinctive Xray-bilateral, patchy, or diffuse alveolar opacities in the presence of normal lung volume. 2/3rd pts recovery by Glucocorticoids

68
THANK YOU

Similar presentations

 Infections (pneumonia, airways disease)>")












 (Restrictive pulmonary Diseases)>")




 How we could do better Dr. D. K. Pillai Wednesday, 13 th August 2014 Medical Update Group at UoM.>")
