Download presentation
Presentation is loading. Please wait.

1
Should we use bivalirudin ? Fibrin 2 1 Thrombin 2 1 Thrombin 2 1 Trombina 2 1 Trombina Bivalirudin ADVANTAGES - No requirement for anti-thrombin III - Effective on clot-bound thrombin - Plasma half-life 25 minutes - No anticoagulation monitoring

3
Primary Endpoint in the ACUITY trial UFH/Enoxaparin + GPI vs. Bivalirudin Alone P NI <0.0001 P Sup = 0.015 P NI = 0.011 P Sup = 0.32 P NI <0.0001 P Sup <0.0001

4
Net Clinical Outcome Composite UFH/Enoxaparin + IIb/IIIa vs. Bivalirudin Alone Yes (n=3197) No (n=6008) Low (0-2) (n=1291) Intermed (3-4) (n=4407) High (5-7) (n=2449) Elevated (n=5368) Normal (n=3841) Risk ratio ±95% CI Risk ratio ±95% CI Bival Alone UFH/Enox + IIb/IIIa 9.2% 11.3% 12.2% 11.1% PP int 0.76 (0.65-0.89) 1.02 (0.86-1.21) 12.2% 7.1% 13.3% 9.4% 0.92 (0.80-1.06) 0.75 (0.61-0.93) 0.23 0.01 <0.001 0.83 0.35 0.02 0.18 13.0% 8.6% 13.7% 10.6% 0.96 (0.80-1.14) 0.81 (0.69-0.95) 0.61 0.01 0.42 Biomarkers (CK/Trop) ST Deviation TIMI Risk Score Pre Thienopyridine 6.4%10.2%0.63 (0.43-0.91)0.01 9.4%10.2%0.92 (0.77-1.10) 0.34 13.9%15.2%0.92 (0.76-1.11)0.36 Yes (n=5192) No (n=4023) RR (95% CI) Bivalirudin alone better UFH/Enox + IIb/IIIa better
 No (n=6008) Low (0-2) (n=1291) Intermed (3-4) (n=4407) High (5-7) (n=2449) Elevated (n=5368) Normal (n=3841) Risk ratio ±95% CI Risk ratio ±95% CI Bival Alone UFH/Enox + IIb/IIIa 9.2% 11.3% 12.2% 11.1% PP int 0.76 ( ) 1.02 ( ) 12.2% 7.1% 13.3% 9.4% 0.92 ( ) 0.75 ( ) < % 8.6% 13.7% 10.6% 0.96 ( ) 0.81 ( ) Biomarkers (CK/Trop) ST Deviation TIMI Risk Score Pre Thienopyridine 6.4%10.2%0.63 ( ) %10.2%0.92 ( ) %15.2%0.92 ( )0.36 Yes (n=5192) No (n=4023) RR (95% CI) Bivalirudin alone better UFH/Enox + IIb/IIIa better.")
6
Effetto della bivalirudina sui sanguinamenti non legati al sito di accesso arterioso allanalisi cumulativa degli studi REPLACE-2, ACUITY e HORIZONS.

8
Landmark Analysis: 30-Day Stent Thrombosis (N=3,124) Bivalirudin: 174917141711167316631591 UFH + GP IIb/IIIa: 181818051804174617241625 Patients at Risk BivalirudinUFH + GP IIb/IIIa Estimated Event Rate (%) Days from Randomisation 0 1 2 3 4 5 5101520253000.51 23 4 30 19 Data on file: The Medicines Company Analysis of safety population in all patients receiving stents
 Bivalirudin: UFH + GP IIb/IIIa: Patients at Risk BivalirudinUFH + GP IIb/IIIa Estimated Event Rate (%) Days from Randomisation Data on file: The Medicines Company Analysis of safety population in all patients receiving stents")
9
Platelet Activation Mechanisms Thrombin Thromboxane A 2 5HT P2Y 12 ADPADPADP 5HT PLATELET ACTIVATION P2Y 1 5HT 2A PAR1 PAR4 Dense granule Thrombingeneration Shapechange IIb 3 IIb 3 Fibrinogen IIb 3 Aggregation Amplification Alpha granule Coagulation factors Inflammatory mediators TP a Coagulation GPVI Collagen ATPATP P2X 1 ASPIRIN x TICLOPIDINECLOPIDOGRELPRASUGREL ACTIVEMETABOLITE x TICAGRELORCANGRELOR GP IIb/IIIa ANTAGONISTS xx Storey RF. Curr Pharm Des. 2006;12:1255-59.

10
PRIMARY COMPOSITE ENDPOINT* IN TRITON AND PLATO TRIALS CLOPIDOGREL NEW DRUG P<.001 *Death,MI,Stroke

11
CLINICAL CHARACTERISTICS OF TRITON AND PLATO POPULATION TRITON (N=13608 pts ) PLATO ( N= 18624 pts ) % PCI 99 64 % CABG 1 10 % NON-INVASIVE 0 29 % STEMI 26 38 Prasugrel (studio TRITON) e stato confrontato con clopidogrel 300 mg LD + 75 mg MD. Ticagrelor (studio PLATO) e stato confrontato con clopidogrel 300-600 mg LD + 75mg MD.
 e stato confrontato con clopidogrel mg LD + 75mg MD..")
12
Study Design, Flow and Compliance 25,087 ACS Patients (UA/NSTEMI 70.8%, STEMI 29.2%) Planned Early (<24 h) Invasive Management with intended PCI Ischemic ECG Δ (80.8%) or cardiac biomarker (42%) 25,087 ACS Patients (UA/NSTEMI 70.8%, STEMI 29.2%) Planned Early (<24 h) Invasive Management with intended PCI Ischemic ECG Δ (80.8%) or cardiac biomarker (42%) PCI 17,232 (70%) Angio 24,769 (99%) Angio 24,769 (99%) No PCI 7,855 (30%) No Sig. CAD 3,616CABG 1,809CAD 2,430 Randomized to receive (2 X 2 factorial): CLOPIDOGREL: Double-dose (600 mg then150 mg/d x 7d then 75 mg/d) vs Standard dose (300 mg then 75 mg/d) ASA: High Dose (300-325 mg/d) vs Low dose (75-100 mg/d) Efficacy Outcomes:CV Death, MI or stroke at day 30 Stent Thrombosis at day 30 Safety Outcomes:Bleeding (CURRENT defined Major/Severe and TIMI Major) Key Subgroup: PCI v No PCI
: CLOPIDOGREL: Double-dose (600 mg then150 mg/d x 7d then 75 mg/d) vs Standard dose (300 mg then 75 mg/d) ASA: High Dose ( mg/d) vs Low dose ( mg/d) Efficacy Outcomes:CV Death, MI or stroke at day 30 Stent Thrombosis at day 30 Safety Outcomes:Bleeding (CURRENT defined Major/Severe and TIMI Major) Key Subgroup: PCI v No PCI.")
13
Days Cumulative Hazard 0.0 0.01 0.02 0.03 0.04 036912151821242730 Clopidogrel: Double vs Standard Dose Primary Outcome: PCI Patients Clopidogrel Standard Clopidogrel Double HR 0.85 95% CI 0.74-0.99 P=0.036 15% RRR CV Death, MI or Stroke

15
CLOPIDOGREL TICAGRELOR

16
TCT 2009 1.6% 3.4% 1.5% 1.2% HR [95%CI] = 1.30 [0.54-3.16] P = 0.56 HR [95%CI] =2.11 [1.07,4.17] P = 0.03 1013 519 1009990969957943863 514497486480474430 Number at risk 600 mg 300 mg Def/Prob Stent Thrombosis (%) 0 1 2 3 4 5 Time in Days 013090180270365 Stent Thrombosis 1-Day Landmark Analysis: Impact of Clopidogrel Loading (Bivalirudin) 600mg Clopidogrel 300mg Clopidogrel
![TCT % 3.4% 1.5% 1.2% HR [95%CI] = 1.30 [ ] P = 0.56 HR [95%CI] =2.11 [1.07,4.17] P = Number at risk 600 mg 300 mg Def/Prob Stent Thrombosis (%) Time in Days Stent Thrombosis 1-Day Landmark Analysis: Impact of Clopidogrel Loading (Bivalirudin) 600mg Clopidogrel 300mg Clopidogrel](http://images.slideplayer.com/1/554802/slides/slide_16.jpg "TCT % 3.4% 1.5% 1.2% HR [95%CI] = 1.30 [ ] P = 0.56 HR [95%CI] =2.11 [1.07,4.17] P = Number at risk 600 mg 300 mg Def/Prob Stent Thrombosis (%) Time in Days Stent Thrombosis 1-Day Landmark Analysis: Impact of Clopidogrel Loading (Bivalirudin) 600mg Clopidogrel 300mg Clopidogrel")
18
8,688 8,763 0102030 8 6 4 2 0 Cumulative incidence (%) Clopidogrel Ticagrelor 4.77 5.43 HR 0.88 (95% CI 0.77–1.00), p=0.045 No. at risk Clopidogrel Ticagrelor 9,291 9,333 8,875 8,942 8,763 8,827 Days after randomisation 3190150 210 270330 8 6 4 2 0 Clopidogrel Ticagrelor 5.28 6.60 8,688 8,673 8,286 8,397 6,379 6,480 Days after randomisation * HR 0.80 (95% CI 0.70–0.91), p<0.001 8,437 8,543 6,945 7,028 4,751 4,822 Cumulative incidence (%) Primary efficacy endpoint over time (composite of CV death, MI or stroke) *Excludes patients with any primary event during the first 30 days
, p< ,437 8,543 6,945 7,028 4,751 4,822 Cumulative incidence (%) Primary efficacy endpoint over time (composite of CV death, MI or stroke) *Excludes patients with any primary event during the first 30 days.")
19
CARDIOVASCULAR DEATH IN TRITON AND PLATO TRIALS NEW DRUG CLOPIDOGREL P<.001

20
Diabetic Subgroup 0 2 4 6 8 10 12 14 16 18 0306090180270360450 HR 0.70 P<0.001 Days Endpoint (%) CV Death / MI / Stroke TIMI Major NonCABG Bleeds NNT = 20 (46) N=3146 17.0 12.2 Prasugrel Clopidogrel Prasugrel Clopidogrel 2.6 2.5
 CV Death / MI / Stroke TIMI Major NonCABG Bleeds NNT = 20 (46) N= Prasugrel Clopidogrel Prasugrel Clopidogrel")
21
ARC Definite or Probable Late Stent Thrombosis* in Patients Receiving DES HR 0.46 (0.22-0.97); P=0.04 ARC = Academic Research Consortium; DES = drug-eluting stent Days 3090150210270330390450 % of Subjects 0.0 0.5 1.0 1.5 2.0 2.5 Prasugrel Clopidogrel 0.91 0.42 P=.04
; P=0.04 ARC = Academic Research Consortium; DES = drug-eluting stent Days % of Subjects Prasugrel Clopidogrel P=.04")
22
NON-CABG RELATED TIMI MAJOR BLEEDING IN TRITON AND PLATO TRIALS CLOPIDOGREL NEW DRUG P=.03

23
FATAL BLEEDING IN TRITON AND PLATO TRIALS CLOPIDOGREL NEW DRUG P=.002

24
INTRACRANIAL HEMORRAGES IN TRITON AND PLATO TRIALS CLOPIDOGREL NEW DRUG P=.06 P<.05

26
Balance of Efficacy and Safety in Patients <75 Yrs, 60 kg, and Without TIA/Stroke Endpoint (%) 0 2 4 6 8 10 12 14 16 03090180 270360450 Hazard Ratio, 1.240 (95% CI, 0.91-1.69) P=0.17 Hazard Ratio, 0.75 (95% CI, 0.66-0.84) P<0.001 Clopidogrel Prasugrel Clopidogrel Prasugrel 1.95% 1.50% 11% 8.4% CV Death / NF MI / NF Stroke Non-CABG TIMI Major Bleeding Days NNT 37 NNH 222 Adapted from Wiviott SD et al NEJM 357: 2001, 2007 Presented at TCT 2009, San Francisco, CA
 Hazard Ratio, (95% CI, ) P=0.17 Hazard Ratio, 0.75 (95% CI, ) P<0.001 Clopidogrel Prasugrel Clopidogrel Prasugrel 1.95% 1.50% 11% 8.4% CV Death / NF MI / NF Stroke Non-CABG TIMI Major Bleeding Days NNT 37 NNH 222 Adapted from Wiviott SD et al NEJM 357: 2001, 2007 Presented at TCT 2009, San Francisco, CA")
27
CLINICAL CHARACTERISTICS OF TRITON AND PLATO POPULATION Variable\\\\ TRITON PLATO AGE (years) 61 62 % FEMALE SEX 26 28 % Cl Creat <60 ml/min 11 4 % DIABETES 23 25 % PRIOR MI 18 20 % PRIOR CABG 8 6
 % FEMALE SEX % Cl Creat <60 ml/min 11 4 % DIABETES % PRIOR MI % PRIOR CABG 8 6")
28
For High Risk, RR=0.58 [ 0.34, 0.98] P= 0.037 Parodi G. TCT 2009
![For High Risk, RR=0.58 [ 0.34, 0.98] P= Parodi G. TCT 2009](http://images.slideplayer.com/1/554802/slides/slide_28.jpg "For High Risk, RR=0.58 [ 0.34, 0.98] P= Parodi G. TCT 2009")
29
COMPOSITE ENPOINT IN CURRENT- OASIS 7 DOUBLE STANDARD P=NS P=0.036

30
CARDIOVASCULAR DEATH IN STEMI PATIENTS INCLUDED IN TRITON PRASUGREL CLOPIDOGREL

31
STENT THROMBOSIS IN TRITON AND PLATO TRIALS CLOPIDOGREL NEW DRUG P<.001 P=.02

32
COMPOSITE ENPOINT IN DIABETIC PATIENTS CLOPIDOGREL NEW DRUG P<.001 NS

33
CARDIOVASCULAR DEATH IN TRITON AND PLATO TRIALS NEW DRUG CLOPIDOGREL P<.001

34
MYOCARDIAL INFARCTION IN TRITON AND PLATO TRIALS CLOPIDOGREL NEW DRUG P<.001 P=.005

35
CABG RELATED TIMI MAJOR BLEEDING IN TRITON AND PLATO TRIALS CLOPIDOGREL NEW DRUG P<.001

36
STROKE IN TRITON AND PLATO TRIALS CLOPIDOGREL NEW DRUG

37
FATAL HEMORRAGES IN PLATO CLOPIDOGREL NEW DRUG P=.03 P=.02

38
NON-ADHERENCE TO STUDY DRUG ( MEDIAN TREATMENT TIME FOR PLATO 9 MONTHS, FOR TRITON 14.5 MONTHS ) CLOPIDOGREL NEW DRUG
 CLOPIDOGREL NEW DRUG")
39
COMPOSITE ENPOINT IN CURRENT- OASIS 7 DOUBLE STANDARD P=.036 P=NS

41
Days Cumulative Hazard 0.0 0.004 0.008 0.012 036912151821242730 Clopidogrel Standard Dose Clopidogrel Double Dose 42% RRR HR 0.58 95% CI 0.42-0.79 P=0.001 Clopidogrel: Double vs Standard Dose Definite Stent Thrombosis (Angio confirmed)
")
42
Ticagrelor betterClopidogrel better Ti.Cl. Total Patients KM % at Month 12 HR (95% CI) Hazard Ratio (95% CI) Yes Revascularization History of CABG Sex Weight Group 65 Years Characteristic 0.51.02.0 172569.511.20.86 (0.78, 0.94) <80 kg 131213.117.30.75 (0.60, 0.99) 60 kg 528811.213.20.83 (0.71, 0.97) <60 kg 133369.211.10.85 (0.76, 0.95) Female 287816.818.30.94 (0.78, 1.12) Male 157448.610.40.82 (0.74, 0.91) 75 Years 797913.216.00.83 (0.74, 0.94) <75 Years 106437.28.50.85 (0.74, 0.97) <65 Years 115219.020.80.87 (0.66, 1.13) Age Group 174629.211.10.84 (0.76, 0.93) No 110619.521.70.88 (0.67, 1.15) Previous TIA/Non-hemorrhagic Stroke 175189.211.00.84 (0.77, 0.93)No Yes Central/South America 80 kg North America 123715.217.90.86 (0.65, 1.13) Europe/Middle East/Africa 171411.414.80.80 (0.61, 1.04) Asia/Australia 466214.116.20.88 (0.76, 1.03) Region 139628.410.20.83 (0.74, 0.92) No 95138.310.50.79 (0.69, 0.90) Medical History of DM 905511.4 12.8 0.90 (0.79, 1.01) 0.2 p- value (Interaction) 0.76 0.84 0.86 0.22 0.82 0.36 0.17 0.05 181411.99.61.25 (0.93, 1.67) 138598.811.00.80 (0.72, 0.90) 0.49 Primary endpoint in pre-defined subgroups (contd)
 Hazard Ratio (95% CI) Yes Revascularization History of CABG Sex Weight Group 65 Years Characteristic (0.78, 0.94) <80 kg (0.60, 0.99) 60 kg (0.71, 0.97) <60 kg (0.76, 0.95) Female (0.78, 1.12) Male (0.74, 0.91) 75 Years (0.74, 0.94) <75 Years (0.74, 0.97) <65 Years (0.66, 1.13) Age Group (0.76, 0.93) No (0.67, 1.15) Previous TIA/Non-hemorrhagic Stroke (0.77, 0.93)No Yes Central/South America 80 kg North America (0.65, 1.13) Europe/Middle East/Africa (0.61, 1.04) Asia/Australia (0.76, 1.03) Region (0.74, 0.92) No (0.69, 0.90) Medical History of DM (0.79, 1.01) 0.2 p- value (Interaction) (0.93, 1.67) (0.72, 0.90) 0.49 Primary endpoint in pre-defined subgroups (contd).")
43
Ticagrelor betterClopidogrel better Ti.Cl. Total Patients KM % at Month 12 HR (95% CI) Hazard Ratio (95% CI) Yes Revascularization History of CABG Sex Weight Group 65 Years Characteristic 0.51.02.0 1708611.510.91.06 (0.96, 1.16) <80 kg 129612.615.20.82 (0.60, 1.12) 60 kg 523710.710.51.01 (0.85, 1.21) <60 kg 1318411.911.41.05 (0.94, 1.16) Female 284614.213.31.04 (0.84, 1.29) Male 1557411.110.81.04 (0.94, 1.15) 75 Years 789214.413.61.07 (0.95, 1.22) <75 Years 105289.5 1.00 (0.87, 1.13) <65 Years 113614.614.90.99 (0.71, 1.37) Age Group 1728411.411.01.04 (0.95, 1.14) No 10927.37.80.94 (0.60, 1.49) Previous TIA/Non-hemorrhagic Stroke 1732911.811.41.04 (0.95, 1.14)No Yes Central/South America 80 kg North America 123015.613.21.22 (0.89, 1.66) Europe/Middle East/Africa 169210.610.81.03 (0.76, 1.40) Asia/Australia 462114.114.80.95 (0.81, 1.12) Region 1380010.810.01.08 (0.97, 1.20) No 942311.410.51.08 (0.95, 1.23) Medical History of DM 895911.7 11.9 0.99 (0.88, 1.13) 0.2 P value (Interaction) 0.68 0.77 0.42 1.00 0.76 0.12 0.35 0.75 175212.912.21.06 (0.80, 1.40) 1374711.111.01.01 (0.91, 1.13) 0.21 HRs and cumulative incidence of major bleeding in pre-defined subgroups (contd)
 Hazard Ratio (95% CI) Yes Revascularization History of CABG Sex Weight Group 65 Years Characteristic (0.96, 1.16) <80 kg (0.60, 1.12) 60 kg (0.85, 1.21) <60 kg (0.94, 1.16) Female (0.84, 1.29) Male (0.94, 1.15) 75 Years (0.95, 1.22) <75 Years (0.87, 1.13) <65 Years (0.71, 1.37) Age Group (0.95, 1.14) No (0.60, 1.49) Previous TIA/Non-hemorrhagic Stroke (0.95, 1.14)No Yes Central/South America 80 kg North America (0.89, 1.66) Europe/Middle East/Africa (0.76, 1.40) Asia/Australia (0.81, 1.12) Region (0.97, 1.20) No (0.95, 1.23) Medical History of DM (0.88, 1.13) 0.2 P value (Interaction) (0.80, 1.40) (0.91, 1.13) 0.21 HRs and cumulative incidence of major bleeding in pre-defined subgroups (contd).")
44
FATAL BLEEDING IN TRITON AND PLATO TRIALS CLOPIDOGREL NEW DRUG P=.002

45
MAJOR BLEEDING

46
Preliminary Results Safety outcomes at 1 month Safety outcomes at 1 month NSTE-ACS 2 of 3 Criteria: Ischemic symptom, ST-T change, troponin rise with TIMI score > 3 Immediate cath Next day cath All PCIs on abciximab 1-month Follow-up IVRS RANDOMIZATION 85% of radial access

47
Preliminary Results Safety outcomes at 1 month ImmediateDelayedP Major bleeding at 1 month, (%) Major bleeding at 1 month, (%) 4.06.80.25 Non-CABG major bleeding Non-CABG major bleeding 2.35.10.26 CABG-related major bleeding CABG-related major bleeding 1.7 1.00 Transfusion > 2 units Transfusion > 2 units 3.45.60.32 Transfusion > 5 units Transfusion > 5 units 1.1 1.00 Thrombocytopenia at 1 month, (%) Thrombocytopenia at 1 month, (%) 2.94.50.41 Non-CABG thrombocytopenia, (%) Non-CABG thrombocytopenia, (%) 2.34.00.54 Post-CABG thrombocytopenia, (%) Post-CABG thrombocytopenia, (%) 0.6 1.00
 Major bleeding at 1 month, (%) Non-CABG major bleeding Non-CABG major bleeding CABG-related major bleeding CABG-related major bleeding Transfusion > 2 units Transfusion > 2 units Transfusion > 5 units Transfusion > 5 units Thrombocytopenia at 1 month, (%) Thrombocytopenia at 1 month, (%) Non-CABG thrombocytopenia, (%) Non-CABG thrombocytopenia, (%) Post-CABG thrombocytopenia, (%) Post-CABG thrombocytopenia, (%)")
48
Preliminary Results Sites of Major Bleedings 1- Gastro-Intestinal 4 2- Puncture-related 4 3- Hemopericardium 2 4- Intracranial 1 5- Epistaxis 1 6- Hematoma (not puncture-related) 1 unknown7 One patient had 2 bleeding events n
 1 unknown7 One patient had 2 bleeding events n")
50
Other findings All patients Ticagrelor (n=9,235) Clopidogrel (n=9,186) p value * Dyspnoea, % Any With discontinuation of study treatment 13.8 0.9 7.8 0.1 <0.001 Holter monitoring at first week, % Ventricular pauses =>3 sec,% Ventricular pauses =>5 sec,% (n=1451) 5.8 2.0 (N=1415) 3.6 1.2 0.01 0.10 *p values were calculated using Fischers exact test
 Clopidogrel (n=9,186) p value * Dyspnoea, % Any With discontinuation of study treatment <0.001 Holter monitoring at first week, % Ventricular pauses =>3 sec,% Ventricular pauses =>5 sec,% (n=1451) (N=1415) *p values were calculated using Fischers exact test")
51
TCT 2009 600mg Clopidogrel 300mg Clopidogrel 2.8% 2.9% 0.4% 0.4% 0% HR=0.21CI=0.01-3.88 P = 0.30 HR=1.08 CI= [0.57,2.05] P = 0.81 1035 559 1034995977963951852 557537531528521482 Number at risk 600 mg 300 mg Def/Prob Stent Thrombosis (%) 0 1 2 3 4 5 Time in Days 013090180270365 P int antithrombin x clopidogrel LD = 0.16 Stent Thrombosis 1-Day Landmark Analysis: Impact of Clopidogrel Loading (UFH+GPI)
![TCT mg Clopidogrel 300mg Clopidogrel 2.8% 2.9% 0.4% 0.4% 0% HR=0.21CI= P = 0.30 HR=1.08 CI= [0.57,2.05] P = Number at risk 600 mg 300 mg Def/Prob Stent Thrombosis (%) Time in Days P int antithrombin x clopidogrel LD = 0.16 Stent Thrombosis 1-Day Landmark Analysis: Impact of Clopidogrel Loading (UFH+GPI)](http://images.slideplayer.com/1/554802/slides/slide_51.jpg "TCT mg Clopidogrel 300mg Clopidogrel 2.8% 2.9% 0.4% 0.4% 0% HR=0.21CI= P = 0.30 HR=1.08 CI= [0.57,2.05] P = Number at risk 600 mg 300 mg Def/Prob Stent Thrombosis (%) Time in Days P int antithrombin x clopidogrel LD = 0.16 Stent Thrombosis 1-Day Landmark Analysis: Impact of Clopidogrel Loading (UFH+GPI)")
52
TCT 2009 3.0% 3.8% HR [95%CI] = 1.30 [0.86-1.95] P = 0.10 1-Year Stent Thrombosis: Impact of Clopidogrel Loading Dose (all pts) 198319061881185818321653 1034983974965952871 Number at risk 600 mg 300 mg 600mg Clopidogrel 300mg Clopidogrel Def/Prob Stent Thrombosis (%) 0 1 2 3 4 5 Time in days 0306090120150180210240270300330365
![TCT % 3.8% HR [95%CI] = 1.30 [ ] P = Year Stent Thrombosis: Impact of Clopidogrel Loading Dose (all pts) Number at risk 600 mg 300 mg 600mg Clopidogrel 300mg Clopidogrel Def/Prob Stent Thrombosis (%) Time in days](http://images.slideplayer.com/1/554802/slides/slide_52.jpg "TCT % 3.8% HR [95%CI] = 1.30 [ ] P = Year Stent Thrombosis: Impact of Clopidogrel Loading Dose (all pts) Number at risk 600 mg 300 mg 600mg Clopidogrel 300mg Clopidogrel Def/Prob Stent Thrombosis (%) Time in days")
53
TCT 2009 0.8% 2.2% 3.2% 0.8% HR [95%CI] = 0.96 [0.41-2.23] P = 0.92 HR [95%CI] = 1.47 [0.93,2.33] P = 0.18 1983 1034 197819201881185818321653 1027990974965952871 Number at risk 600 mg 300 mg Def/Prob Stent Thrombosis (%) 0 1 2 3 4 5 Time in Days 013090180270365 Stent Thrombosis 1-Day Landmark Analysis: Impact of Clopidogrel Loading 600mg Clopidogrel 300mg Clopidogrel
![TCT % 2.2% 3.2% 0.8% HR [95%CI] = 0.96 [ ] P = 0.92 HR [95%CI] = 1.47 [0.93,2.33] P = Number at risk 600 mg 300 mg Def/Prob Stent Thrombosis (%) Time in Days Stent Thrombosis 1-Day Landmark Analysis: Impact of Clopidogrel Loading 600mg Clopidogrel 300mg Clopidogrel](http://images.slideplayer.com/1/554802/slides/slide_53.jpg "TCT % 2.2% 3.2% 0.8% HR [95%CI] = 0.96 [ ] P = 0.92 HR [95%CI] = 1.47 [0.93,2.33] P = Number at risk 600 mg 300 mg Def/Prob Stent Thrombosis (%) Time in Days Stent Thrombosis 1-Day Landmark Analysis: Impact of Clopidogrel Loading 600mg Clopidogrel 300mg Clopidogrel")
54
TCT 2009 2.8% 3.6% HR [95%CI] = 0.78 [0.44-1.37] P = 0.38 727693685678668592 829793778768759698 Number at risk Eptifibatide Abciximab Def/Prob Stent Thrombosis (%) 0 1 2 3 4 Time in days 0306090120150180210240270300330365 Eptifibatide Abciximab 1-Year Stent Thrombosis: Impact of GPI in the UFH Group
![TCT % 3.6% HR [95%CI] = 0.78 [ ] P = Number at risk Eptifibatide Abciximab Def/Prob Stent Thrombosis (%) Time in days Eptifibatide Abciximab 1-Year Stent Thrombosis: Impact of GPI in the UFH Group](http://images.slideplayer.com/1/554802/slides/slide_54.jpg "TCT % 3.6% HR [95%CI] = 0.78 [ ] P = Number at risk Eptifibatide Abciximab Def/Prob Stent Thrombosis (%) Time in days Eptifibatide Abciximab 1-Year Stent Thrombosis: Impact of GPI in the UFH Group")
55
November 15, 2007

56
August 30, 2009

57
Conclusioni (1) La bivalirudina riduce i sanguinamenti locali e dorgano nei pazienti con SCA sottoposti a PCI, soprattutto in quelli a maggior rischio emorragico ( anziani ). Per una efficace copertura antiischemica deve essere associata ad un regime di doppia anti-aggregazione piastrinica (aspirina + bloccante recettore P2Y12).
..")
58
Conclusioni (2) - I nuovi farmaci che bloccano il recettore P2Y12 ( prasugrel, ticagrelor ) sono risultati piu efficaci del clopidogrel grazie alla loro migliore farmacocinetica e farmacodinamica. Ad essi si associa tuttavia un maggior rischio emorragico. - Lanalisi di efficacia e di rischio in particolari sottogruppi di pazienti con SCA potra permettere di utilizzare il farmaco piu vantaggioso per la condizione clinica del singolo paziente.

59
TCT 2009 Independent Predictors of Subacute ST (Cox Model) VariableHR [95% CI]P-value Insulin-treated diabetes4.43 [2.03, 9.65]0.0002 History of CHF4.16 [1.61, 10.76]0.003 Pre-PCI TIMI flow 0/12.21 [1.05, 4.63]0.04 Final TIMI flow 0/13.72 [1.10, 12.55]0.03 Stent to lesion length ratio1.44 [1.20, 1.71]<0.0001 Clopidogrel loading dose 600 mg (vs. 300 mg) 0.49 [0.27, 0.89]0.01
![TCT 2009 Independent Predictors of Subacute ST (Cox Model) VariableHR [95% CI]P-value Insulin-treated diabetes4.43 [2.03, 9.65] History of CHF4.16 [1.61, 10.76]0.003 Pre-PCI TIMI flow 0/12.21 [1.05, 4.63]0.04 Final TIMI flow 0/13.72 [1.10, 12.55]0.03 Stent to lesion length ratio1.44 [1.20, 1.71]< Clopidogrel loading dose 600 mg (vs.](http://images.slideplayer.com/1/554802/slides/slide_59.jpg "300 mg) 0.49 [0.27, 0.89]0.01.")
60
Montalescot et al. ESC 2008 Stent thrombosis (ARC Definite/probable ) HR=0.58 (0.36–0.93) NNT=83 p=0.02 RRR=42% 0100200300400 0 1 2 3 Proportion of patients (%) Time (Days) 2.4 1.2 2.8 1.6 p=0.008 RRR=51% Clopidogrel Prasugrel Age-adjusted HR=0.59 (0.37-0.96)
 HR=0.58 (0.36–0.93) NNT=83 p=0.02 RRR=42% Proportion of patients (%) Time (Days) p=0.008 RRR=51% Clopidogrel Prasugrel Age-adjusted HR=0.59 ( ).")
61
ARC Definite or Probable Stent Thrombosis (day 0 to day 450) 2.35 1.13 HR 0.48 (0.36-0.64); P<0.0001 Prasugrel Clopidogrel 1 year: 1.06 vs. 2.15% HR 0.48 (0.36-0.65); P<0.0001 ARC = Academic Research Consortium Days 050100150200250300350400450 % of Subjects 0.0 0.5 1.0 1.5 2.0 2.5 52% RRR
; P< ARC = Academic Research Consortium Days % of Subjects % RRR.")
64
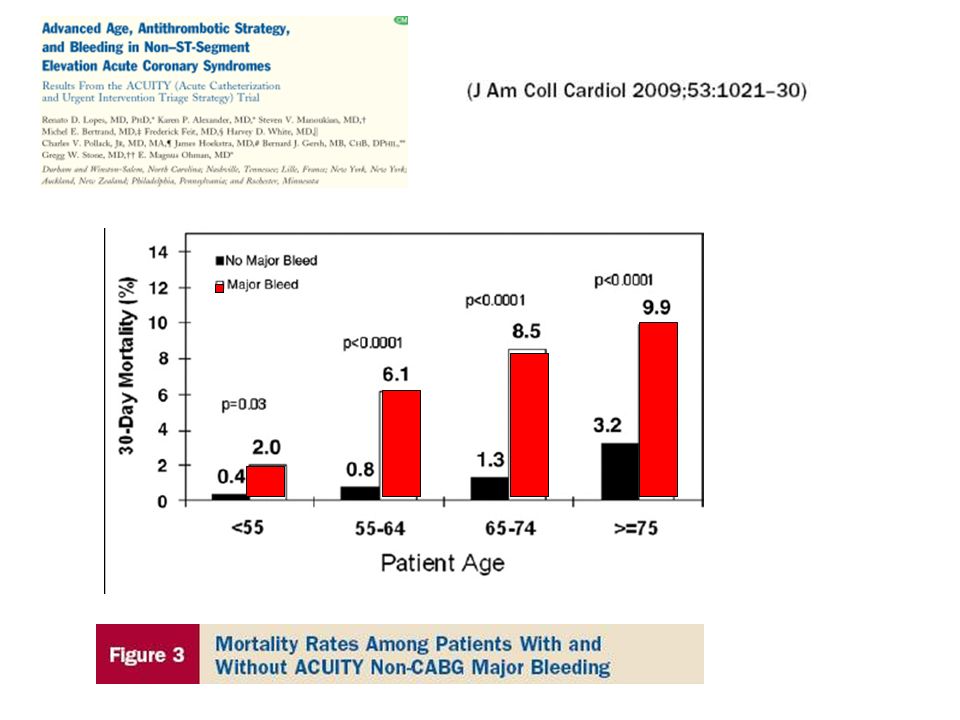
BIVALIRUDIN UFH + GPIIbIIIa INH. DEATH RATE IN ELDERLY PATIENTS IN THE ACUITY TRIAL

65
Net Clinical Benefit Bleeding Risk Subgroups OVERALL >=60 kg < 60 kg < 75 >=75 No Yes 0.512 Prior Stroke / TIA Age Wgt Risk (%) + 37 -16 -16 +3 -14 -13 Prasugrel BetterClopidogrel Better HR P int = 0.006 P int = 0.18 P int = 0.36 Post-hoc analysis
 Prasugrel BetterClopidogrel Better HR P int = P int = 0.18 P int = 0.36 Post-hoc analysis")
66
TCT 2009 2.8% 3.6% HR [95%CI] = 0.78 [0.44-1.37] P = 0.38 727693685678668592 829793778768759698 Number at risk Eptifibatide Abciximab Def/Prob Stent Thrombosis (%) 0 1 2 3 4 Time in days 0306090120150180210240270300330365 Eptifibatide Abciximab 1-Year Stent Thrombosis: Impact of GPI in the UFH Group
![TCT % 3.6% HR [95%CI] = 0.78 [ ] P = Number at risk Eptifibatide Abciximab Def/Prob Stent Thrombosis (%) Time in days Eptifibatide Abciximab 1-Year Stent Thrombosis: Impact of GPI in the UFH Group](http://images.slideplayer.com/1/554802/slides/slide_66.jpg "TCT % 3.6% HR [95%CI] = 0.78 [ ] P = Number at risk Eptifibatide Abciximab Def/Prob Stent Thrombosis (%) Time in days Eptifibatide Abciximab 1-Year Stent Thrombosis: Impact of GPI in the UFH Group")
67
TCT 2009 3.0% 3.8% HR [95%CI] = 1.30 [0.86-1.95] P = 0.10 1-Year Stent Thrombosis: Impact of Clopidogrel Loading Dose (all pts) 198319061881185818321653 1034983974965952871 Number at risk 600 mg 300 mg 600mg Clopidogrel 300mg Clopidogrel Def/Prob Stent Thrombosis (%) 0 1 2 3 4 5 Time in days 0306090120150180210240270300330365
![TCT % 3.8% HR [95%CI] = 1.30 [ ] P = Year Stent Thrombosis: Impact of Clopidogrel Loading Dose (all pts) Number at risk 600 mg 300 mg 600mg Clopidogrel 300mg Clopidogrel Def/Prob Stent Thrombosis (%) Time in days](http://images.slideplayer.com/1/554802/slides/slide_67.jpg "TCT % 3.8% HR [95%CI] = 1.30 [ ] P = Year Stent Thrombosis: Impact of Clopidogrel Loading Dose (all pts) Number at risk 600 mg 300 mg 600mg Clopidogrel 300mg Clopidogrel Def/Prob Stent Thrombosis (%) Time in days")
68
TCT 2009 1.6% 3.4% 1.5% 1.2% HR [95%CI] = 1.30 [0.54-3.16] P = 0.56 HR [95%CI] =2.11 [1.07,4.17] P = 0.03 1013 519 1009990969957943863 514497486480474430 Number at risk 600 mg 300 mg Def/Prob Stent Thrombosis (%) 0 1 2 3 4 5 Time in Days 013090180270365 Stent Thrombosis 1-Day Landmark Analysis: Impact of Clopidogrel Loading (Bivalirudin) 600mg Clopidogrel 300mg Clopidogrel
![TCT % 3.4% 1.5% 1.2% HR [95%CI] = 1.30 [ ] P = 0.56 HR [95%CI] =2.11 [1.07,4.17] P = Number at risk 600 mg 300 mg Def/Prob Stent Thrombosis (%) Time in Days Stent Thrombosis 1-Day Landmark Analysis: Impact of Clopidogrel Loading (Bivalirudin) 600mg Clopidogrel 300mg Clopidogrel](http://images.slideplayer.com/1/554802/slides/slide_68.jpg "TCT % 3.4% 1.5% 1.2% HR [95%CI] = 1.30 [ ] P = 0.56 HR [95%CI] =2.11 [1.07,4.17] P = Number at risk 600 mg 300 mg Def/Prob Stent Thrombosis (%) Time in Days Stent Thrombosis 1-Day Landmark Analysis: Impact of Clopidogrel Loading (Bivalirudin) 600mg Clopidogrel 300mg Clopidogrel")
73
No. at risk Clopidogrel Ticagrelor 9,291 9,333 8,560 8,678 8,405 8,520 8,177 Days after randomisation 6,703 6,796 5,136 5,210 4,109 4,191 060120180240300360 6 5 4 3 2 1 0 7 Cumulative incidence (%) Clopidogrel Ticagrelor 5.8 6.9 8,279 HR 0.84 (95% CI 0.75–0.95), p=0.005 060120180240300360 6 4 3 2 1 0 Clopidogrel Ticagrelor 4.0 5.1 HR 0.79 (95% CI 0.69–0.91), p=0.001 7 5 9,291 9,333 8,865 8,294 8,780 8,822 8,589 Days after randomisation 7079 7119 5,441 5,482 4,364 4,4198,626 Myocardial infarction Cardiovascular death Cumulative incidence (%) Secondary efficacy endpoints over time
 Clopidogrel Ticagrelor ,279 HR 0.84 (95% CI 0.75–0.95), p= Clopidogrel Ticagrelor HR 0.79 (95% CI 0.69–0.91), p= ,291 9,333 8,865 8,294 8,780 8,822 8,589 Days after randomisation ,441 5,482 4,364 4,4198,626 Myocardial infarction Cardiovascular death Cumulative incidence (%) Secondary efficacy endpoints over time.")
76
TICAGRELOR (AZD6140) A non-thienopyridine, in the chemical class CPTP (CycloPentylTriazoloPyrimidine) 1) First oral reversible ADP P2Y 12 receptor antagonist 2) Direct acting via the P2Y 12 receptor - metabolism not required for activity ( not a pro-drug ) 3) More potent platelet inhibitor than clopidogrel HO HN HO OH OS F F N N N N N
 A non-thienopyridine, in the chemical class CPTP (CycloPentylTriazoloPyrimidine) 1) First oral reversible ADP P2Y 12 receptor antagonist 2) Direct acting via the P2Y 12 receptor - metabolism not required for activity ( not a pro-drug ) 3) More potent platelet inhibitor than clopidogrel HO HN HO OH OS F F N N N N N")
79
BIVALIRUDIN UFH + GPIIbIIIa INH. DEATH RATE IN ELDERLY PATIENTS UNDERGOING PCI

80
Messaggi finali (1) - La doppia terapia antiaggregante e un cardine fondamentale del trattamento delle sindromi coronariche acute. - Lo studio CURRENT ha mostrato che nei pazienti con sindrome coronarica acuta il doppio dosaggio di clopidogrel ( 600 mg seguito da 150 mg per una settimana ) migliora i risultati clinici ad 1 mese solo nei pazienti sottoposti a PCI.
 migliora i risultati clinici ad 1 mese solo nei pazienti sottoposti a PCI..")
81
Messaggi finali (2) - I nuovi farmaci che bloccano il recettore P2Y12 ( prasugrel, ticagrelor ) sono risultati piu efficaci del clopidogrel negli studi di confronto a lungo termine grazie alla loro migliore farmacocinetica e farmacodinamica. Da non sottovalutare tuttavia il maggior rischio emorragico ad essi associato. - Lanalisi di efficacia e di rischio di questi nuovi farmaci antipiastrinici in particolari sottogruppi di pazienti con SCA potra permettere di utilizzare il farmaco piu vantaggioso per la condizione clinica del singolo paziente.

83
TRITON TIMI-38 STEMI cohort Efficacy endpoints at 30 days Montalescot et al. ESC 2008 * ARC def/probable 0 2 4 6 8 10 All DeathMIUTVRStent Thrombosis* CV Death/ MI CV Death/ MI/UTVR CV Death/ MI/Stroke Proportion of population (%) p= 0.04 p= 0.01 p= 0.13 p= 0.008 p= 0.004 p= 0.02 p= 0.002 Clopidogrel Prasugrel
 p= 0.04 p= 0.01 p= 0.13 p= p= p= 0.02 p= Clopidogrel Prasugrel.")
84
Other findings – laboratory parameters All patients Ticagrelor (n=9,235) Clopidogrel (n=9,186) p value * % increase in creatinine from baseline At 1 month At 12 months Follow-up visit 10 22 11 22 10 22 8 21 9 22 10 22 <0.001 0.59 % increase in uric acid from baseline At 1 month At 12 months Follow-up visit 14 46 15 52 7 43 7 44 7 31 8 48 <0.001 0.56 Values are mean % SD; *p values were calculated using Fishers exact test
 Clopidogrel (n=9,186) p value * % increase in creatinine from baseline At 1 month At 12 months Follow-up visit < % increase in uric acid from baseline At 1 month At 12 months Follow-up visit < Values are mean % SD; *p values were calculated using Fishers exact test")
85
CREDO: Benefits of Clopidogrel Plus Aspirin to 1 Year Following PCI CV Death, MI or Stroke *Plus ASA and other standard therapies. Steinhubl S, et al. JAMA. 2002;288:2411-2420 Combined Endpoint Occurrence (%) Months From Randomization 27% RRR P=.02 Placebo* Clopidogrel* 0 5 10 15 8.5% 11.5% 036912
 Months From Randomization 27% RRR P=.02 Placebo* Clopidogrel* % 11.5%")
87
2485 PATIENTS WITH STENT PLACEMENT PRETREATED WITH CLOPIDOGREL 600 mg

94
August 30, 2009 at 08.00 CET

95
Diabetic Subgroup 0 2 4 6 8 10 12 14 16 18 0306090180270360450 HR 0.70 P<0.001 Days Endpoint (%) CV Death / MI / Stroke TIMI Major NonCABG Bleeds NNT = 20 (46) N=3146 17.0 12.2 Prasugrel Clopidogrel Prasugrel Clopidogrel 2.6 2.5
 CV Death / MI / Stroke TIMI Major NonCABG Bleeds NNT = 20 (46) N= Prasugrel Clopidogrel Prasugrel Clopidogrel")
96
990 patients with ACS

97
Patients with age 60 Kg and no prior CVA/TIA Patients with age 60 Kg and no prior CVA/TIA CLOPIDOGREL(n=5383) PRASUGREL (n=5421) CV EVENTS 11% (12,1%) 11% (12,1%) 8,3% (9,9%) (DEATH,MI,STROKE) P<.001 NNT=37 (46)
 PRASUGREL (n=5421) CV EVENTS 11% (12,1%) 11% (12,1%) 8,3% (9,9%) (DEATH,MI,STROKE) P<.001 NNT=37 (46)")
98
Other findings All patients Ticagrelor (n=9,235) Clopidogrel (n=9,186) p value * Dyspnoea, % Any With discontinuation of study treatment 13.8 0.9 7.8 0.1 <0.001 Neoplasms arising during treatment, % Any Malignant Benign 1.4 1.2 0.2 3.6 1.2 0.4 0.17 0.69 0.02 *p values were calculated using Fischers exact test
 Clopidogrel (n=9,186) p value * Dyspnoea, % Any With discontinuation of study treatment <0.001 Neoplasms arising during treatment, % Any Malignant Benign *p values were calculated using Fischers exact test")
99
Holter monitoring & Bradycardia related events Holter monitoring at first week Ticagrelor (n=1,451) Clopidogrel (n=1,415)p value Ventricular pauses 3 seconds, % Ventricular pauses 5 seconds, % 5.8 2.0 3.6 1.2 0.01 0.10 Holter monitoring at 30 days Ticagrelor (n= 985) Clopidogrel (n=1,006)p value Ventricular pauses 3 seconds, % Ventricular pauses 5 seconds, % 2.1 0.8 1.7 0.6 0.52 0.60 Bradycardia-related event, % Ticagrelor (n=9,235) Clopidogrel (n=9,186) p value Pacemaker Insertion Syncope Bradycardia Heart block 0.9 1.1 4.4 0.7 0.9 0.8 4.0 0.7 0.87 0.08 0.21 1.00
 Clopidogrel (n=1,415)p value Ventricular pauses 3 seconds, % Ventricular pauses 5 seconds, % Holter monitoring at 30 days Ticagrelor (n= 985) Clopidogrel (n=1,006)p value Ventricular pauses 3 seconds, % Ventricular pauses 5 seconds, % Bradycardia-related event, % Ticagrelor (n=9,235) Clopidogrel (n=9,186) p value Pacemaker Insertion Syncope Bradycardia Heart block")
100
Kaplan Meier estimates of non-CABG-related TIMI Major bleeding Non-ideal populationIdeal population

101
TIMI major non-CABG bleeding Montalescot et al. ESC 2008 0.5 1.0 2.0 2.5 1.5 2.1 2.4 HR=1.11 (0.70–1.77) NNH=333 Proportion of patients (%) Time (Days) p=0.65 0100200300400 0 Clopidogrel Prasugrel Age-adjusted HR=1.19 (0.75-1.89)
 NNH=333 Proportion of patients (%) Time (Days) p= Clopidogrel Prasugrel Age-adjusted HR=1.19 ( ).")
102
Montalescot et al. ESC 2008 Stent thrombosis ARC Definite/probable HR=0.58 (0.36–0.93) NNT=83 p=0.02 RRR=42% 0100200300400 0 1 2 3 Proportion of patients (%) Time (Days) 2.4 1.2 2.8 1.6 p=0.008 RRR=51% Clopidogrel Prasugrel Age-adjusted HR=0.59 (0.37-0.96)
 NNT=83 p=0.02 RRR=42% Proportion of patients (%) Time (Days) p=0.008 RRR=51% Clopidogrel Prasugrel Age-adjusted HR=0.59 ( ).")
103
Diabetic Subgroup 0 2 4 6 8 10 12 14 16 18 0306090180270360450 HR 0.70 P<0.001 Days Endpoint (%) CV Death / MI / Stroke TIMI Major NonCABG Bleeds NNT = 20 (46) N=3146 17.0 12.2 Prasugrel Clopidogrel Prasugrel Clopidogrel 2.6 2.5
 CV Death / MI / Stroke TIMI Major NonCABG Bleeds NNT = 20 (46) N= Prasugrel Clopidogrel Prasugrel Clopidogrel")
105
ARC Definite or Probable Early Stent Thrombosis (0–30 days) Prasugrel Clopidogrel 1.56 0.64 HR 0.41 (0.29-0.59); P<0.0001 Days 051015202530 % of Subjects 0.0 0.5 1.0 1.5 2.0 2.5 ARC = Academic Research Consortium
 Prasugrel Clopidogrel HR 0.41 ( ); P< Days % of Subjects ARC = Academic Research Consortium")
106
ARC Definite or Probable Late Stent Thrombosis* in Patients Receiving DES HR 0.46 (0.22-0.97); P=0.04 ARC = Academic Research Consortium; DES = drug-eluting stent Days 3090150210270330390450 % of Subjects 0.0 0.5 1.0 1.5 2.0 2.5 Prasugrel Clopidogrel 0.91 0.42 P=.04
; P=0.04 ARC = Academic Research Consortium; DES = drug-eluting stent Days % of Subjects Prasugrel Clopidogrel P=.04")
107
COMPOSITE ENPOINT IN CURRENT- OASIS 7 DOUBLE STANDARD P=.036 P=NS

108
Clopidogrel: Double vs Standard Dose Primary Outcome and Components StandardDoubleHR95% CIPIntn P CV Death/MI/Stroke PCI (2N=17,232)4.53.90.850.74-0.990.036 0.016 No PCI (2N=7855)4.24.91.170.95-1.440.14 Overall (2N=25,087)4.44.20.950.84-1.070.370 MI PCI (2N=17,232)2.62.00.780.64-0.950.012 0.025 No PCI (2N=7855)1.41.71.250.87-1.790.23 Overall (2N=25,087)2.21.90.860.73-1.030.097 CV Death PCI (2N=17,232)1.9 0.960.77-1.190.68 1.0 No PCI (2N=7855)2.82.70.960.74-1.260.77 Overall (2N=25,087)2.22.10.960.81-1.140.628 Stroke PCI (2N=17,232)0.4 0.880.55-1.410.59 0.50 No PCI (2N=7855)0.80.91.110.68-1.820.67 Overall (2N=25,087)0.5 0.990.70-1.390.950
 No PCI (2N=7855) Overall (2N=25,087) MI PCI (2N=17,232) No PCI (2N=7855) Overall (2N=25,087) CV Death PCI (2N=17,232) No PCI (2N=7855) Overall (2N=25,087) Stroke PCI (2N=17,232) No PCI (2N=7855) Overall (2N=25,087)")
109
Death, MI, urgent revascularization

110
Clopidogrel in ACS Clopidogrel + ASA* 369 Placebo + ASA* Months of Follow-Up p = 0.00009 N = 12,562 0 12 * In addition to other standard therapies. The CURE Trial Investigators. N Engl J Med. 2001;345:494 20% Relative Risk Reduction Primary End Point – MI/Stroke/CV Death

113
TIMI major and minor bleeding

114
Should we use bivalirudin ? Fibrin 2 1 Thrombin 2 1 Thrombin 2 1 Trombina 2 1 Trombina Bivalirudin

115
Bivalirudin as an Alternative to UFH/LMWH Advantages of the direct thrombin inhibitor bivalirudin –No requirement for anti-thrombin III –Effective on clot-bound thrombin –Inhibits thrombin-mediated platelet activation –Plasma half-life 25 minutes –No requirement for anticoagulant monitoring Advantages of the direct thrombin inhibitor bivalirudin –No requirement for anti-thrombin III –Effective on clot-bound thrombin –Inhibits thrombin-mediated platelet activation –Plasma half-life 25 minutes –No requirement for anticoagulant monitoring

116
RADIAL ACCESS FEMORAL ACCESS

Similar presentations


























 No significant increase in rate of major hemorrhage 0 20 40 60 ESSENCE n = 3171 TIMI 11B n = 3910.>")



 Apixaban (oral) Betrixiban (oral) Edoxaban (oral)>")







 from UFH/Enox to Bivalirudin: Results from ACUITY Dr. Harvey White Green Lane Cardiovascular Service.>")



 ENOX < 75 y: 30 mg IV bolus SC 1.0 mg / kg q 12 h (Hosp DC) ≥ 75 y: No bolus SC 0.75.>")
 Presented.>")