Download presentation
Presentation is loading. Please wait.

1
National COPD Programme Building QI into Your Audit from the Start Prof. Mike Roberts Royal College of Physicians Barts Health/ UCLPartners On behalf of the team

2
Programme Overview 3 plus 2 year programme 2013-8 Commissioned & funded by HQIP Led by the Royal College of Physicians (RCP) working in close partnership with – British Thoracic Society (BTS) – British Lung Foundation (BLF) – Primary Care Respiratory Society (PCRS-UK) and – Royal College of General Practitioners (RCGP)
 working in close partnership with – British Thoracic Society (BTS) – British Lung Foundation (BLF) – Primary Care Respiratory Society (PCRS-UK) and – Royal College of General Practitioners (RCGP)")
3
Programme Workstreams Primary care audit – Collection of clinical audit data from General Practice patient record systems looking back over a year. Spring 2015 then annual. Secondary care snapshot audit – Admissions to hospital with COPD exacerbation process and outcomes at 30 and 90 days. Organisation and Resources over data collection period. Spring 2014 & 2016. Pulmonary rehabilitation snapshot audits – Service quality and patient outcomes over 3 months. Includes resources and organisation. Jan 2015 start. Repeat 2017. PREM – One year development work exploring the potential/feasibility for Patient Reported Experience Measures to be incorporated into the programme in the future. Patient identifiable data linked across the workstreams and to external sources such as HES and ONS

4
Measures - Process and Outcome Primary care e.g. compliance against NICE standard- diagnosis confirmed, smoking cessation, annual review, referral to PR, correct treatment etc. Secondary care e.g. Essential investigations and interventions in first 24 hours, integrated discharge. Pulmonary Rehab e.g. Compliance with BTS standards, completion, better QoL, improved exercise capacity. Mortality, Hospital Stay, Readmission.

5
UK COPD Audit Progression 1997 36 hospitals process and outcomes 2001 30 hospitals process/outcomes + organisation and resources 2004 94% all UK Trusts (as per 2001) 2008 98% of all UK Trusts process/outcomes + resources and organisation + patient experience + primary care record 2010 Euro Audit of hospital care & resources
 % of all UK Trusts process/outcomes + resources and organisation + patient experience + primary care record 2010 Euro Audit of hospital care & resources")
6
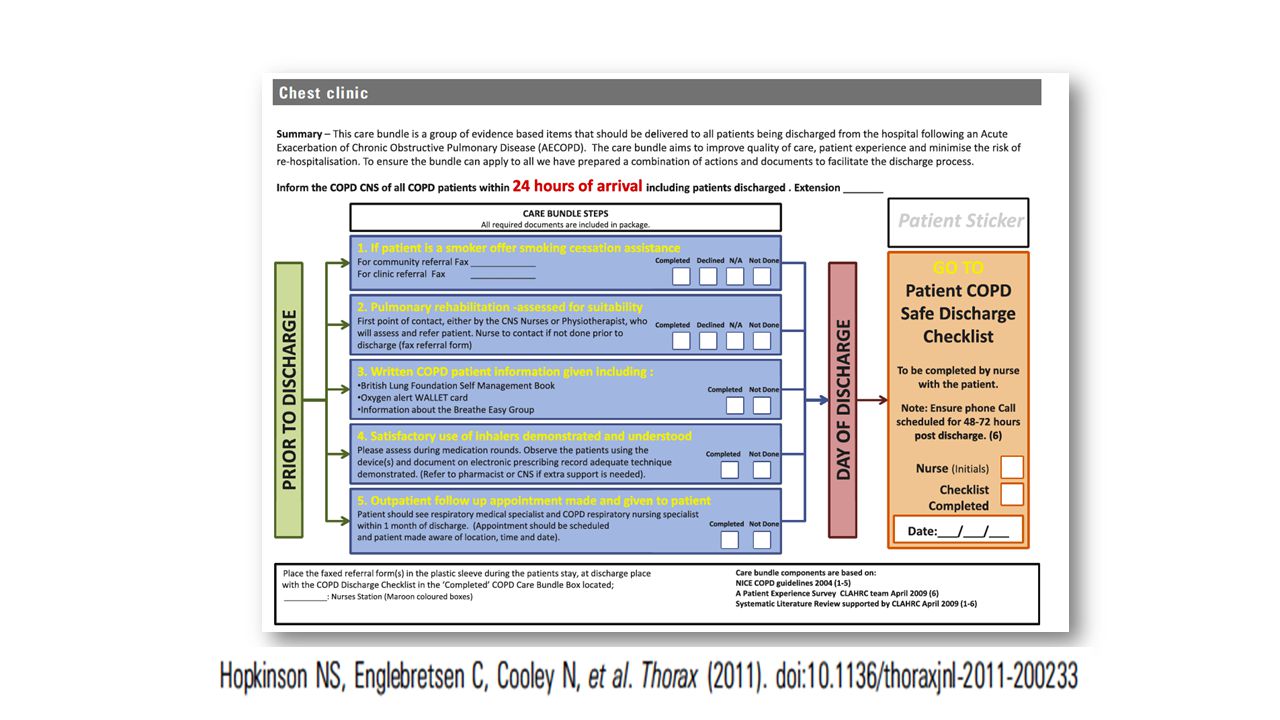
Audit is a quality improvement process

7
UK National COPD Audit % patients with pH< 7.35 Receiving Ventilatory Support by Individual Units

8
8

9
Quality indicators for North West SHA acute units (14 - 27) Acute unitOrg scoreNIVPREDSLTOT Site 148188868389 Site 157779827882 Site 167771827232 Site 178175958393 Site 1880638610079 Site 19666377082 Site 2077679510064 Site 2151091086 Site 226367820100 Site 2345460036 Site 246867918396 Site 255425595661 Site 2672831009493 Site 278458918986
 Acute unitOrg scoreNIVPREDSLTOT Site Site Site Site Site Site Site Site Site Site Site Site Site Site")
10
Hospital Report

11
NICE Management Guidelines for COPD NICE COPD Quality Standards DH Outcomes Strategy for COPD NHS COPD Commissioning Toolkit

12
Over Time Some resources have increased Wider service provision But Little evidence of improved processes But Length of stay reduced Readmissions have increased Mortality remains high

13
What Have We Done Differently? Acknowledge QI is key Establish a QI group Look for links with external organisations Emphasise to participants the QI opportunities Suggest QI options to participants Engagement, engagement, engagement! ‘Make it as easy as possible to do the right thing for the patient’

15
Engaging with Professionals Radical Message Kept simple (but with significant range of consequences) Balanced with the good Something that appeals to professionals and patients alike Strap line – ‘Who Cares Matters’ Supported by National Professional bodies
 Balanced with the good Something that appeals to professionals and patients alike Strap line – ‘Who Cares Matters’ Supported by National Professional bodies")
16
Engaging Commissioners CCG/LHB Level Reports- what do you want to see? CCG engagement (e.g. via CCG Champion Networks of partner organisations) Identifying CCG priorities Targeted messaging Benchmarking against NICE standards Potential for peer review (e.g. accreditation of Pulmonary Rehabilitation)
 Identifying CCG priorities Targeted messaging Benchmarking against NICE standards Potential for peer review (e.g. accreditation of Pulmonary Rehabilitation).")
17
National Engagement All Party Parliamentary Group on Respiratory Health NHSE Domains NHS Wales – Policy leads (NCA; Respiratory; Primary Care; Adult & Children’s Health) National Respiratory Director NHSE – Head of Patient Experience NHSIQ
 National Respiratory Director NHSE – Head of Patient Experience NHSIQ")
18
Engaging Patients and Carers British Lung Foundation – Including network of Breatheasy Groups Patient involvement groups – professional bodies (e.g. RCP PIU) The plain English version Conferences and newsletters And in an ideal world patient access to their own data!
 The plain English version Conferences and newsletters And in an ideal world patient access to their own data!.")
20
Summary Reporting of data has limited impact Acknowledging QI is critical element at outset Having a QI strategy Engaging key parties We have no resource or contract to deliver QI Over to you- Health Quality Improvement Partnership

21
To Find Out More If you would like to register to receive updates: Email: copd@rcplondon.ac.ukcopd@rcplondon.ac.uk Or visit: www.rcplondon.ac.uk/COPDwww.rcplondon.ac.uk/COPD #COPDaudit #COPDwhocares?

Similar presentations

? Helen Ellis, Primary Care Contracting.>")





>")












